
{kind=link}

Eczema Herpeticum This Herpes simplex virus, most commonly HSV-1, causes Eczema herpeticum, which is a serious viral skin infection that occurs mostly in people with atopic dermatitis (eczema). The condition is characterized by the sudden outbreak of painful, fluid-filled blisters and typical punched-out sores, which occur over those areas that have eczema. Systemic symptoms like fever, swollen lymph nodes, and general malaise are also commonly seen with it. Eczema herpeticum is regarded as a dermatological emergency that should be treated with antivirals urgently to avoid severe complications.[1]
What is Eczema Herpeticum?: Eczema Herpeticum This
Kaposi varicella eruption or eczema herpeticum (EHE) is an uncommon but potentially serious herpes simplex infection that occurs in patients with underlying skin disorders, most often atopic dermatitis. It is transmitted when the herpes simplex virus (typically HSV-1, which causes cold sores) enters already weakened skin and proliferates quickly within the epidermis, leading to widespread cutaneous involvement. Contrary to the normal cold sores, which localize, eczema herpeticum results in widespread skin involvement, which may involve large portions of the face, neck, and trunk.
This disease was initially defined by the Austrian dermatologist Moritz Kaposi in 1887, who initially suspected that it was chicken pox because of its extensive vesicular rash.[2] Eczema herpeticum is a name used specifically to refer to herpes simplex virus infection of eczematous skin, and the general term Kaposi varicelliform eruption refers to herpes simplex virus infection superimposed on various preexisting inflammatory or barrier-disrupting skin diseases.
The infection is a severe complication, as the broken skin barrier in eczema patients permits the virus to enter deeply and propagate widely. Eczema herpeticum is a particularly worrying issue due to its possible development into a systemic disease with a variety of affected organs in case of untimely treatment.
How Common is Eczema Herpeticum?
Eczema herpeticum is not very common and occurs in less than 3 per cent of individuals with atopic dermatitis. This percentage, however, represents a large number of cases considering the prevalence of eczema among the general population. In developed countries, atopic dermatitis is found in about 15-20% of children, and therefore, eczema herpeticum should be a significant issue for pediatricians and dermatologists.[3]
Infants and young children, especially those below 3 years of age, are mostly affected by the condition, although it may occur at any age. Children who have had the onset of atopic dermatitis at an early age seem to be more at risk. There is an equal distribution between males and females. Adults who have severe eczematous disease may also acquire eczema herpeticum, particularly in cases where they have never been exposed to the herpes simplex virus before.

The patient has eczema and has skin lesions associated with herpes being widespread on her face. Mohammad2018 — Own work,CC BY-SA 4.0(Wikimedia Commons).
Recent studies have suggested that there is a possibility that the condition is rising in prevalence, and individuals previously infected are at risk of a second infection. People who are most vulnerable to the development of this complication are those with poorly controlled or severe atopic dermatitis, particularly those involving the head and neck or large regions of the body. Additional risk factors include filaggrin gene mutations, high serum IgE levels, early-onset severe eczema, and significant skin barrier dysfunction.
Signs and Symptoms of Eczema Herpeticum
Eczema herpeticum normally manifests acutely, and the symptoms occur 5-12 days following contact with an individual infected with herpes simplex virus. The individual can or cannot possess visible cold sores.[4]
Initial Presentation:
- Suddenly, several small swellings (vesicles) appeared in groups.
- The blisters are monomorphic (similar in appearance) and dome-shaped.
- The diameter of vesicles is usually 1-3 millimeters.
- In the beginning, there is clear or yellowish fluid in the blisters.
- Some blisters can hold blood or pus.
- Painful or tingling sensation at affected sites.
- Lesions are typically umbilicated (central depression) before rupture.
Progressive Symptoms:
- In 1-2 weeks, blisters burst, leaving typical erosions known as punched out.
- Ulcers in the shape of circles with sharp edges.
- Blood crusts over erosions (hemorrhagic).
- Blisters keep appearing after 7-10 days.
- Lesions can be joined together to become bigger patches of denuded skin.
- Honey-colored crusting on the parts in case of secondary bacterial infection.
Distribution:
- The neck, upper trunk, and face are the most affected.
- Usually appears in the parts formerly or currently affected by eczema.
- Can also grow on normal skin.
- Children have a high prevalence of head and neck infections.
Systemic Symptoms:
- High fever and chills
- Lymphadenopathy
- General feeling of illness and fatigue (malaise)
- Pain is more severe than the usual episodes of eczema
- Loss of appetite
- In extreme cases, vomiting, diarrhea, and irritability may occur among children
With prompt antiviral treatment, most patients improve significantly within 48 hours, and complete healing typically occurs within 10–14 days, although residual erythema or post-inflammatory changes may persist longer.
Although mild cases may occasionally resolve spontaneously, systemic antiviral therapy is strongly recommended in all patients due to the risk of rapid progression and complications.
Is Eczema Herpeticum Contagious?
Yes, eczema herpeticum is very contagious. A strain of herpes simplex virus causes this infection and can be transmitted either when one person is in direct skin-to-skin contact with an infected person, or when the latter is not having an outburst, or does not even show signs of the infection. This renders prevention especially difficult.[5]
How It Spreads:
- Direct contact with active cold sores or herpes lesions
- Touching fluid from broken blisters
- Using other people’s personal properties such as towels, razors or utensils.
- Kissing or being physically close (particularly children through family love).
- Exposure to the virus shedding by asymptomatic people.
Autoinoculation: Autoinoculation can also occur in infected individuals, whereby people transmit the virus to other body parts. This happens when a person touches an active lesion and thereafter touches another part of the skin, especially the eczematous parts.
Contagious Period: Eczematous patients with herpeticum are infectious until all of the lesions have crusted and healed. In this period, they need not be in close contact with others, especially:
- Other persons with eczema or compromised skin barriers
- Infants and young children
- Immunocompromised persons
- Pregnant women
Dermatitis Herpeticum
Although the specific herpetic infection of atopic dermatitis is called eczema herpeticum, herpes simplex infections that infect other skin diseases with impaired barriers are also known as “dermatitis herpeticum” or “Kaposi varicella eruption”:[6]
- Seborrheic dermatitis
- Contact dermatitis (irritant or allergic)
- Darier disease
- Pemphigus foliaceus
- Ichthyosis vulgaris
- Burns
- Skin damage from cosmetic procedures (laser treatment, chemical peels)
- Long-term topical steroid use
The pathophysiology is also similar in these conditions: the defective skin barrier permits the herpes simplex virus to enter the body and spread on the surface of the skin.
What Causes Eczema Herpeticum?
Infection with the herpes simplex virus, usually HSV-1 (Herpes simplex virus type 1, the most common cause of oral cold sores) or HSV-2 (usually associated with genital herpes), may cause eczema herpeticum.
Herpes simplex virus should not be confused with varicella-zoster virus, which causes chickenpox and shingles and is a different virus.
Rarely, other viral infections may produce a similar clinical picture, but classic eczema herpeticum is caused by HSV.[7]
Role of Atopic Dermatitis:
Patients with atopic dermatitis are predisposed to this infection by some factors:
- Weakened Skin Barrier: The skin of patients with eczema is defective in structural proteins, specifically filaggrin, which is a protein that keeps the skin barrier intact. This enables easier entry of viruses.
- Disturbed Immune Response: Atopic dermatitis patients have a distorted immune system that does not effectively respond to viral infections on the skin.
- Chronic Inflammation: The chronic inflammation of the eczematous skin provides an environment in which viruses reproduce.
- Skin Trauma: Scratches in the skin lead to points of entry of the virus.
The mode of infection: The virus normally enters the body through:
- Physical contact with an infected person with HSV.
- Restoration of the dormant HSV in the body.
- Auto-inoculation of oral lesions.
- Contact with contaminated surfaces or objects.
After entering the affected skin, the virus quickly replicates, leading to the typical massive epidemic.
Eczema Herpeticum Stages
The understanding of eczema herpeticum evolution will help in the early diagnosis and treatment:
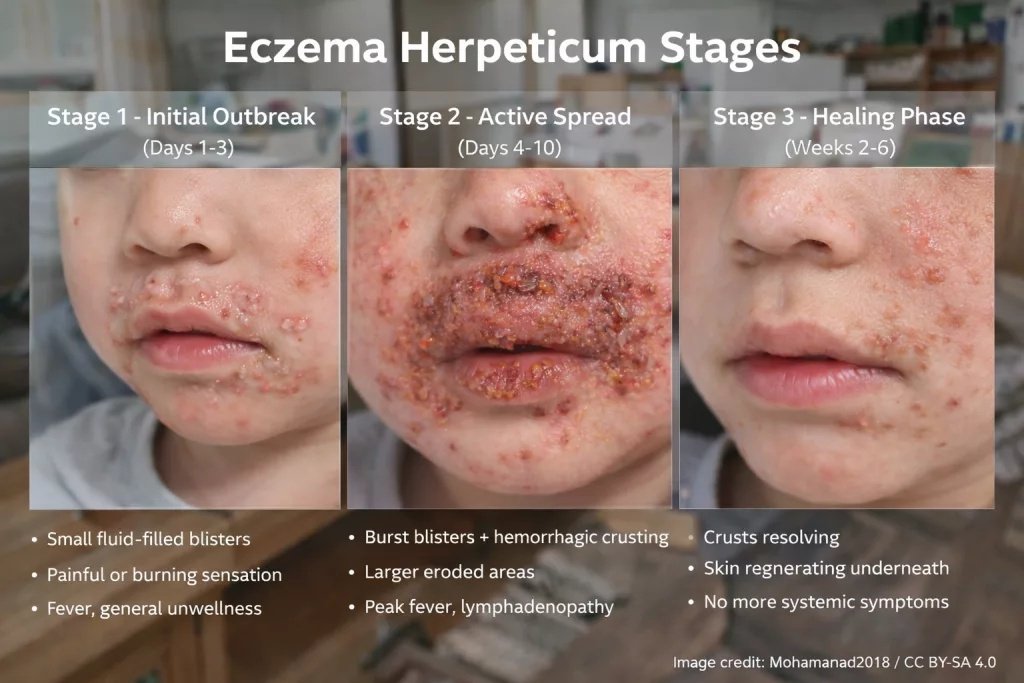
The course of Eczema herpeticum includes the development of the disease into fluid-filled blisters (days 1-3), active crust erosions (days 4-10), and a slow healing stage (weeks 2-6).
Stage 1 – Initial Outbreak (Days 1-3):
- Sudden emergence of tiny blisters that are fluid-filled.
- On eczematous or normal skin, blisters are found in groups.
- Painful or burning sensation
- Fever may begin
- Patient feels generally unwell
2nd Stage – Active Spread (Days 4-10):
- There are still new crops of vesicles appearing.
- The blisters that are present burst open, forming a punched-out erosion.
- Hemorrhagic crusting develops
- Lesions can become larger in size.
- High fever, lymphadenopathy
- Secondary bacterial infection, particularly with Staphylococcus aureus, may occur during this stage.
Stage 3 – Healing Phase (Weeks 2-6):
- With treatment, no new lesions develop (in case of an effective treatment).
- Existing erosions begin to crust over
- Gradual resolution of crusts
- Skin regeneration underneath
- Systemic symptoms resolve
- In the serious cases, scarring can take place
The initial treatment period and the overall severity are determined by how soon the patient is treated, the level of immunity, and the occurrence of complications.
Diagnosis of Eczema Herpeticum
Eczematous herpeticum is diagnosed by performing a physical examination. Physicians seek some common signs, such as groupings of painful, fluid-filled blisters that are punched-out or umbilicated. These lesions generally increase in rapid progression on the preexisting eczema areas, mostly on the face, neck, and trunk. Weeping, crusting, and bleeding may also be present on the affected skin.[8]
Patient History
An elaborate medical history is very important in proper diagnosis. Doctors will inquire about the past episodes of eczema, recent cold sore outbreaks, and whether the patient was exposed to herpes simplex virus. The fever, malaise, or swollen lymph nodes, together with the abrupt appearance of the symptoms, can give a valuable diagnosis.
Laboratory Testing
The diagnosis should be confirmed by laboratory tests. The most frequently used technique is swabbing the blister fluid and then culturing using the viral culture or polymerase chain reaction (PCR) test to determine herpes simplex virus DNA. PCR has more accurate and quicker results compared to traditional cultures. Blood tests can be ordered as well to test for systemic infection and exclude other cases.
Differential Diagnosis
Medical professionals should be able to differentiate between eczema herpeticum and other related diseases, such as impetigo, varicella, or severe exacerbation of eczema. Distribution pattern, swift progression, and typical appearance of the lesions are some of the characteristics that distinguish eczema herpeticum from other skin conditions. Some of the common differentials are discussed below:
| Condition | Key Distinguishing Features |
|---|---|
| Impetigo | Honey-colored crusts without monomorphic vesicles; usually not painful; absence of punched-out erosions; bacterial origin. |
| Varicella (Chickenpox) | Lesions at different stages (papules, vesicles, crusts simultaneously); generalized distribution; usually no underlying eczema. |
| Severe Eczema Flare | No umbilicated vesicles or punched-out erosions; intense itching rather than pain; absence of systemic viral symptoms. |
| Eczema Coxsackium | Caused by enterovirus; vesicles often involve hands, feet, and oral mucosa; milder systemic symptoms; PCR negative for HSV. |
| Allergic Contact Dermatitis | Pruritic vesicles with clear trigger exposure; lacks monomorphic appearance and systemic viral symptoms. |
Eczema Herpeticum Treatment
Eczema herpeticum is a dermatological emergency that should be treated within a short time to avoid complications. Systemic antiviral therapy is the key to the treatment.
Antiviral Medications:
In the mild to moderate cases (Outpatient Treatment):[9]
Acyclovir:
- Adults: 400mg orally 5 times per day for 7-14 days.
- Children: 30-60 mg/kg/day in 3-5 doses.
- Continue until all lesions have crusted over
Valacyclovir:
- Adults: 1000 mg orally twice daily for 7-21 days
- Pediatric dosing should be weight-based according to standard clinical guidelines.
For Severe Cases or Immunocompromised Patients (Hospital Admission):
Intravenous Acyclovir:
- 15-30 mg/kg/day divided into 3 doses
- Minimum 5-7 days of IV therapy
- Change to oral medication on improvement
Supportive Care:
- Cool compresses
- Treatment of pain using acetaminophen or ibuprofen.
- Sufficient fluid replacement, particularly in febrile children.
- Carry on with regular eczema management as tolerated.[10]
Management of Secondary Bacterial Infection:
Staphylococcus aureus is the most common bacterium that superinfects about one-third of patients:
- Topical or oral antibiotics against the Staphylococcus and Streptococcus species.
- Usual options include cephalexin, clindamycin, doxycycline, or trimethoprim-sulfamethoxazole.
- Culture-guided antibiotic selection when possible
- In case of suspected bacteremia, some patients can be on IV antibiotics.
Eye Involvement:
In case of ocular involvement:
- Emergency consultation of the ophthalmologist.
- Eye topical antiviral drops
- Untreated ocular herpes infection may lead tokeratitis and permanent corneal scarring.
Hospitalization Criteria:
Refer to hospital admission due to:[11]
- Severe or extensive disease
- Immunocompromised patients
- Newborn babies and small children.
- Eye involvement
- Failure to take oral medications.
- Failure to respond to outpatient treatment.
- Indications of secondary bacterial infection with sepsis.
Prevention of Cases that Recur:
In patients who have recurrent infections more than once:[12]
- Acyclovir 400 mg twice daily or 200 mg three times daily
- Valacyclovir twice a day, 250mg or 500mg a day.
- Suppressive long-term therapy can be taken into consideration.
Treatment Response:
The majority of patients respond and improve in 24-48 hours after taking antiviral therapy. Fevers are usually cured in 2-3 days. Healing takes 26 weeks to heal fully. The inability to improve implies potential herpes virus resistance to acyclovir, which necessitates other antiviral agents such as foscarnet.
Possible Complications of Eczema Herpeticum
- Ocular involvement
- Secondary bacterial sepsis
- HSV viremia
- Rarely, herpes simplex encephalitis
- Scarring
Before antiviral therapy was available, mortality was significant; however, with early treatment, mortality is now very low.
Conclusion
Herpetic eczema is an infection caused by the herpes simplex virus, which is potentially severe and which infects the skin of a person with atopic dermatitis or other inflammatory diseases. This disorder is related to painful blisters that appear abruptly, so-called punched-out erosions, and systemic manifestations.
Whereas eczema herpeticum is contagious and is transmitted by direct contact, the connection of dermatitis herpeticum and stages of eczema herpeticum makes it possible to intervene in time. The evolution of the primitive vesicles to the healing erosions normally develops in a predictable pattern during 2-6 weeks when treated properly.
Atopic dermatitis is interrelated with eczema herpeticum. Eczema is most effectively prevented by good control, including good management of the skin and taking medications. The patients with atopic dermatitis need to be informed on how to avoid getting in contact with active herpes infections that are active and the early warning signs.
Systemic antiviral agents such as acyclovir or valacyclovir are very effective in the treatment of eczema herpeticum and must be taken early. However, postponement of the treatment can result in critical complications, including eye damage, secondary infections by bacteria, and, in rare cases, the involvement of the systemic organs.
References
[1] Traidl S, Roesner L, Zeitvogel J, Werfel T. Eczema herpeticum in atopic dermatitis. Allergy. 2021;76(10):3017-3027. doi: 10.1111/all.14853
[2] Hoss DM, Baddour LM. Psoriasis herpeticum: three cases of Kaposi’s varicelliform eruption in psoriasis. J Am Acad Dermatol. 2005;52(6):1009-1011. doi: 10.1016/j.jaad.2005.01.032
[3] Faye O, Petit A, Barbarot S. Atopic dermatitis: A global health perspective. J Eur Acad Dermatol Venereol. 2024;38(1):12-24. doi: 10.1111/jdv.19723
[4] Wollenberg A, Zoch C, Wetzel S, Plewig G, Przybilla B. Predisposing factors and clinical features of eczema herpeticum: a retrospective analysis of 100 cases. J Am Acad Dermatol. 2003;49(2):198-205. doi: 10.1067/mjd.2003.451
[5] Wollenberg A, Wetzel S, Burgdorf WH, Haas J. Viral infections in atopic dermatitis: pathogenic aspects and clinical management. J Allergy Clin Immunol. 2003;112(4):667-674. doi: 10.1016/s0091-6749(03)01638-0
[6] Skrek SV, Timoshchuk EA, Sidikov AA, Zaslavsky DV, Megna M. Kaposi varicelliform eruption induced by methotrexate in an adult atopic dermatitis patient. Dermatol Ther. 2019;32(2):e12826. doi: 10.1111/dth.12826
[7] Beck LA, Boguniewicz M, Hata T, et al. Phenotype of atopic dermatitis subjects with a history of eczema herpeticum. J Allergy Clin Immunol. 2009;124(2):260-269. doi: 10.1016/j.jaci.2009.05.020
[8] Chen TM, George S, Woodruff CA, Hsu S. Clinical manifestations of varicella-zoster virus infection. Dermatol Clin. 2002;20(2):267-282. doi: 10.1016/s0733-8635(01)00020-6
[9] Aronson PL, Yan AC, Mittal MK, Mohamad Z, Shah SS. Delayed acyclovir and outcomes of children hospitalized with eczema herpeticum. Pediatrics. 2011;128(6):1161-1167. doi: 10.1542/peds.2011-0565
[10] Akamatsu M, Kawamura Y, Miura H, et al. Systemic herpes simplex virus infection in a child with eczema herpeticum. Pediatr Dermatol. 2023;40(3):582-583. doi: 10.1111/pde.15253
[11] Aronson PL, Aoki DS, Yan AC. Hospital care for children with eczema herpeticum. Pediatr Dermatol. 2013;30(4):454-458. doi: 10.1111/pde.12094
[12] Liao CC, Cheng SH, Fang YH, Hsieh CT. Eczema herpeticum in an immunocompetent man. Diagn Microbiol Infect Dis. 2024;110(1):116304. doi: 10.1016/j.diagmicrobio.2024.116304