
{kind=link}

Evans Syndrome Symptoms Evans Syndrome is a rare autoimmune condition defined by the simultaneous or sequential occurrence of two or more autoimmune cytopenias, most commonly autoimmune hemolytic anemia (AIHA) and immune thrombocytopenia (ITP), and sometimes autoimmune neutropenia.[1] This combination of disorders is unusual and is more difficult to treat than other isolated autoimmune blood diseases. It is a lifelong condition, as a patient can have periods of remission and relapse.[2]
Why is it considered a Rare Autoimmune Disorder?: Evans Syndrome Symptoms
Evans Syndrome is an extremely rare disease. As per the medical literature, there is an estimated incidence of about 1–2 cases per million person-years and a prevalence in some cohorts up to ~20 per million.[3] It is therefore uncommon but probably under-recognized. Unlike other autoimmune illnesses, including rheumatoid arthritis or lupus, Evans Syndrome doesn’t have a single set of features and is therefore complex.[4]
Most patients consult one doctor and then another, only to be told that they do not know what is wrong with them. As there is not much research on it, it is commonly called the “orphan disease.” The medical community should give it attention for a better future.
The Historical Background
Evans Syndrome has been named after Dr. Robert Evans, who identified in 1951, the first patients who had both autoimmune hemolytic anemia and immune thrombocytopenia. Before this observation, doctors considered these blood disorders as separate, unrelated conditions.[5]
Types of Evans Syndrome
Clinically, doctors often distinguish it into primary (idiopathic) and secondary forms:
- Primary Evans Syndrome: Occurs on its own, without being linked to another disease. Its exact cause is unknown, but it is thought to be related to immune system dysregulation.
- Secondary Evans Syndrome: Develops in association with another condition such as systemic lupus erythematosus (SLE), autoimmune lymphoproliferative syndrome (ALPS), or common variable immunodeficiency (CVID). This form often has more severe complications and influences treatment choices.
What causes Evans syndrome?
Autoimmunity:
In Evans Syndrome, an immune reaction is erroneously directed against one’s own blood cells by autoantibodies. This causes them to be destroyed prematurely, causing anemia, low platelet levels, or a low number of white blood cells.[6]
Genetic & Environmental Factors:
Some genetic mutations related to immune dysregulation are predictive of this syndrome. Families with a history of autoimmune disorders may be at higher risk of bringing up children with autoimmune tendencies.
Environmental factors like viral infections, chronic inflammation, and exposure to some drugs can also act as triggers. For example, infections like Epstein-Barr virus (EBV) or cytomegalovirus (CMV) have been reported as potential catalysts in patients with underlying immune vulnerabilities. However, these triggers simply contribute to its onset in genetically predisposed individuals.[7]
Secondary Causes Linked with Other Disorders:
Evans Syndrome may develop in patients with:
- Systemic lupus erythematosus (SLE)
- Autoimmune lymphoproliferative syndrome (ALPS)
- Common variable immunodeficiency (CVID)
The secondary form often presents with more severe complications and may require more aggressive treatment. Understanding whether Evans Syndrome is primary (occurring on its own) or secondary (linked to another condition) is crucial because it influences treatment decisions and prognosis.
Symptoms of Evans Syndrome
Common Symptoms:
The symptoms of Evans Syndrome are diverse because they depend on which blood cells are being destroyed at a given time.[8]
- When red blood cells are affected, patients often experience fatigue, weakness, dizziness, and shortness of breath due to anemia. Pale skin and jaundice (yellowing of the skin or eyes) are also common indicators.
- When platelets are under attack, easy bruising, nosebleeds, gum bleeding, and prolonged bleeding from minor cuts may occur. Some patients may develop small red or purple spots on the skin (petechiae), which are caused by bleeding under the skin.
- In cases where white blood cells are reduced, patients may become more vulnerable to infections. Recurring fevers, chronic illnesses, and difficulty recovering from common infections are frequent red flags. Because Evans Syndrome involves fluctuating cycles of relapse and remission, symptoms may appear suddenly, disappear for weeks or months, and then return without warning.
How Symptoms Differ Between Children and Adults?
Children with Evans Syndrome often present more severe cases than adults. They may experience sudden, dramatic drops in blood cell counts, leading to emergency hospital visits. Pediatric patients also have a higher likelihood of being associated with other immune disorders, such as ALPS.
On the other hand, adults usually develop this disease more slowly, sometimes taking years before a proper diagnosis is made. Adults also face a high risk of complications, such as organ damage from repeated episodes of anemia or side effects from long-term steroid use.
The relapses are still frequent in both age groups, but have been addressed well by some treatments, such as immunoglobulins or rituximab.
What Complications arise from the Syndrome?
Life-threatening complications are a result of the involvement of multiple blood cells. E.g;[9]
- Severe anemia can lead to heart failure in extreme cases.
- Low platelet counts increase the risk of internal bleeding that can be the cause of dangerous brain hemorrhages.
- Neutropenia leaves the body defenseless against infections, which can rapidly increase the mortality rate.
Another reason for the complications comes from the treatments themselves. Long-term use of steroids or immunosuppressive drugs can weaken the body, making it more susceptible to infections, bone loss, and hormonal imbalances.[10]
How is Evans Syndrome Diagnosed?
Routine blood tests show abnormalities in the count that are significant in diagnosis.[11]

illustration of the Coombs test
- Complete blood counts (CBC) often show anemia, thrombocytopenia, or neutropenia.
- A more specific test is the direct antiglobulin test (DAT or Coombs test), which confirms whether antibodies are attacking red blood cells.
- Bone marrow biopsies are performed to rule out other causes of low blood cell counts, such as leukemia or aplastic anemia.
- Additional immunological tests are used to check for autoantibodies that indicate immune system dysfunction.
To sum it up, diagnosis is clinical plus laboratory: CBC demonstrating cytopenias, a positive direct antiglobulin (Coombs) test in AIHA, and exclusion of other causes (e.g., marrow failure, leukemia). Bone marrow biopsy and immunologic testing are used when needed to exclude alternative diagnoses or find an associated immune dysregulation.
Because symptoms overlap with many other conditions, diagnosis is often delayed or missed entirely. It is usually only after repeated relapses and abnormal test results that doctors confidently diagnose Evans Syndrome.
Differential Diagnosis from Other Autoimmune Disorders
Evans Syndrome is often misdiagnosed due to similar symptoms with several autoimmune and hematological disorders. These conditions include:
- Idiopathic thrombocytopenic purpura (ITP)
- Autoimmune hemolytic anemia (AIHA)
- Systemic lupus erythematosus (SLE)
- Even certain cancers must first be excluded
- Specific conditions like HELLP, when occurring during pregnancy
It is a long process that may require weeks or even months and leave the patients frustrated. The Evans Syndrome diagnosis is such a big issue that even expert hematologists have to critically observe the lab results and history before making a conclusion.[12]
Challenges in Early Detection:
One of the difficulties in the diagnosis of Evans Syndrome is its overall inconsistency. The number of blood cells can vary significantly within a short period. Some patients spend years with vague symptoms, such as fatigue and bruises, before an accurate diagnosis is made. In contrast, others have severe complications when they are diagnosed for the first time.[13]
Treatment Approaches for Evans Syndrome
Managing Evans Syndrome is challenging because the disease tends to relapse and often requires more than one type of therapy. Treatments aim to control the immune system, improve blood counts, and reduce complications.
First-Line Treatments: Steroids & Immunoglobulins
- The first line of treatment is corticosteroids, such as prednisone. The steroids reduce the production of those harmful autoantibodies that destroy blood cells. This is done by suppressing the immune system. At the start of treatment, most patients have a good response with improved blood counts and relief from fatigue, bleeding, and other symptoms. But with the long-term use of steroids, the effectiveness often declines, and comes with side effects like weight gain, high blood pressure, osteoporosis, and increased risk of infections.
- Another first-line treatment is intravenous immunoglobulin (IVIG). This therapy works by increasing the healthy antibodies in your body, which interfere with the destructive autoantibodies. IVIG is more effective in acute cases when patients need rapid improvement, such as before surgery or during a severe relapse. The drawback is that its benefits are short-lived, often lasting only a few weeks, and repeated infusions may be required.
First-line treatments are not a permanent solution. The combination of steroids and IVIG can provide only immediate relief. Patients who relapse frequently or fail to respond need stronger, second-line therapies.[14]
Second-Line Therapies: Rituximab & Immunosuppressants
When first-line treatments are not enough, doctors turn to second-line options like rituximab, a monoclonal antibody therapy.[15]
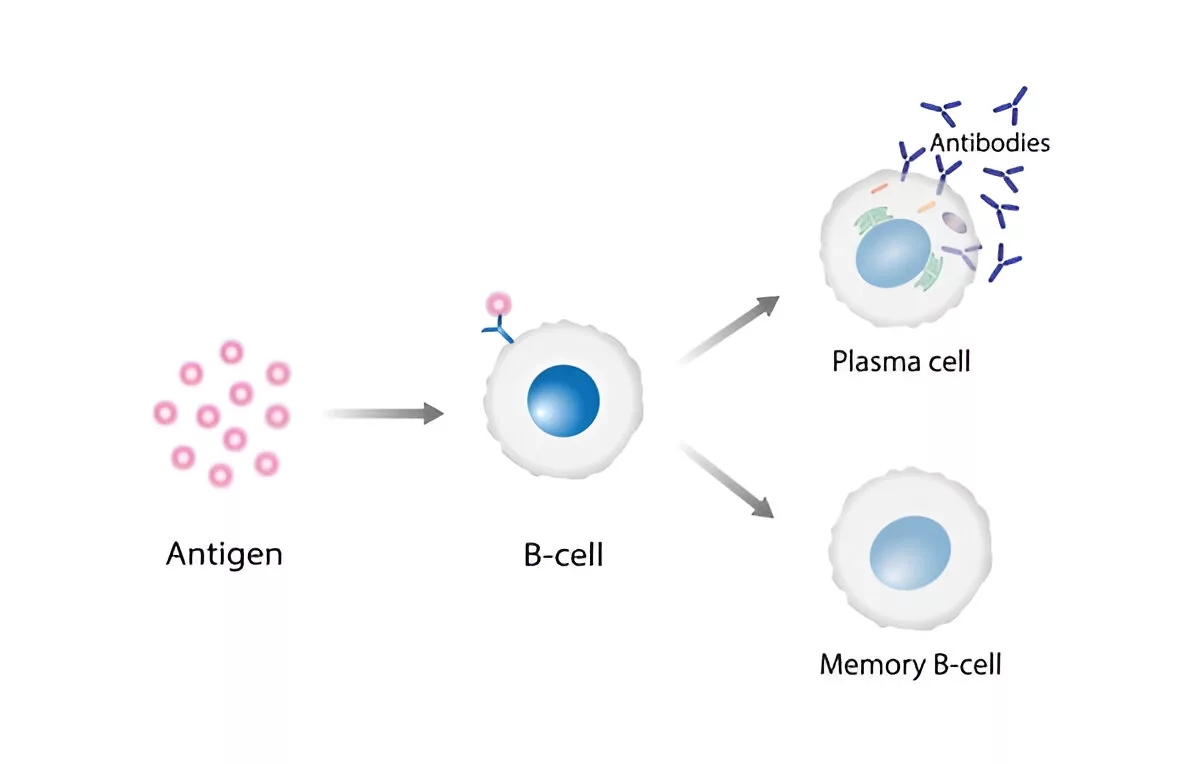
B cells’ pathway to produce antibodies
- Rituximab targets B cells, which are immune cells responsible for producing antibodies that can be harmful. By destroying these B cells, rituximab can help achieve longer periods of remission. Some patients experience remarkable improvement after rituximab, but others relapse after months or years, highlighting the unpredictable nature of Evans Syndrome.
- Immunosuppressive drugs are also used, such as azathioprine, cyclosporine, and mycophenolate mofetil.
These medications act on the overall activity of the immune system, reducing attacks on blood cells. However, because they suppress immunity broadly, patients become more vulnerable to infections. Doctors must carefully balance the benefits of controlling Evans Syndrome against the risks of leaving the body defenseless.
- Another second-line strategy is splenectomy (removal of the spleen). Since the spleen is one of the main organs that destroys antibody-coated blood cells, removing it can help some patients. However, this approach is less common today because it doesn’t work for everyone and may increase the risk of infections later in life.
Bone Marrow Transplant & Emerging Therapies:
For severe, treatment-resistant cases, hematopoietic stem cell transplantation (also known as a bone marrow transplant) may be considered. This aggressive treatment essentially resets the immune system by replacing diseased bone marrow with healthy donor cells. While potentially curative, it carries significant risks, including rejection, graft-versus-host disease, and life-threatening infections. Because of these risks, it is reserved for patients who have exhausted other treatment options.[16]
Although there is no universal cure, the growing number of treatment options is a sign of progress. With continued research, patients may eventually benefit from therapies that provide long-term remission with fewer side effects.
Evans Syndrome vs ITP
Since ITP (Immune Thrombocytopenia) is one of the hallmark conditions in Evans Syndrome, people often confuse the two. While they share similarities, there are important differences:
| Feature | ITP | Evans Syndrome |
|---|---|---|
| Definition | Autoimmune destruction of platelets only | Autoimmune destruction of plateletsandred blood cells (± neutrophils) |
| Symptoms | Bruising, bleeding, petechiae | Combination of bleeding (ITP) + anemia (AIHA) ± infections (AIN) |
| Severity | Usually less severe, though it can be serious | More severe due to multiple cytopenias |
| Prognosis | Many patients achieve remission with treatment | Higher relapse rate, more complications, poorer prognosis |
| Management | Steroids, IVIG, rituximab | Requires broader immunosuppression, often multi-drug therapy |
In short, all patients with Evans Syndrome have ITP, but not all patients with ITP have Evans Syndrome.
Living with Evans Syndrome
How do I take care of myself while living with Evans syndrome?
Life with Evans Syndrome can be unpredictable. Relapses are common, and patients may need long-term medications, frequent blood tests, and hospital visits. Emotional and psychological support is also crucial, as living with a rare chronic illness can be stressful.[17]
Lifestyle tips for patients include:
- Regular monitoring of blood counts
- Avoiding medications that increase bleeding risk (e.g., aspirin without doctor approval)
- Prompt treatment of infections
- A healthy diet and rest to manage fatigue
- Support groups for coping with the challenges of a rare disease
Prognosis & Long-Term Outlook
Life Expectancy with Evans Syndrome:
Evans syndrome does not always shorten life expectancy. Many individuals have only mild or episodic symptoms. With medical advances, life expectancy has risen, but extreme anemia, hemorrhages, and infections are significant concerns for mortality. Children are likely to have a more severe course, whereas adults have gradual development with complications over a long time.[18]
When Evans syndrome occurs with another chronic illness (secondary Evans syndrome), overall life expectancy may be influenced by that underlying condition, as it may carry its own risks and potential complications.
Relapse & Remission Cycles:
Evans Syndrome usually presents a relapsing-remitting pattern, which means the patient becomes stable at a time, then relapses unexpectedly. This cycle may be quite challenging emotionally, so it is important to have the right strategy for treatment and for monitoring regularly in the future.[19]
Factors Influencing Prognosis:
The following factors affect the prognosis:
- Age at the time of diagnosis
- Response to treatment
- Other health problems
Secondary Evans Syndrome and resistance to initial treatment can result in more complex outcomes, but routine observation and care help in enhancing long-term outcomes.
Advances in Research and Future Perspectives
Latest Clinical Trials and Studies:
Current research into Evans Syndrome is expanding, and there is an active clinical trial program into biologics that target immune pathways, CTLA-4, and PD-1 inhibitors. Combination with other treatments is also being studied with rituximab, and lower-dose chemotherapy with stem cell transplantation is under investigation to achieve better outcomes.
Potential for Personalized Medicine:
Personalized medicine is emerging as a significant development in Evans Syndrome. To achieve better efficacy and to reduce side effects, doctors give treatments that cover both the genetic composition and the immune system of an individual. Genetic testing is very useful in the best possible treatment, especially for complex or resistant cases.[20]
The Role of Genetic Research:
Genetic studies are providing insights into why some individuals develop Evans Syndrome and identifying the changes responsible for defective regulation of the immune system. These studies also involve specific therapies and preventive opportunities for family members at risk, allowing early treatment interventions.[21]
Conclusion
This syndrome is a very rare autoimmune disease of blood cells resulting in conditions such as anemia, bleeding, and infections. Although its etiology is unknown, it is believed to be a result of genetic factors, an immune dysregulation, and environmental factors.
Treatment involves a combination of medical treatment and lifestyle alteration, emotional support, and constant monitoring. There is no permanent cure; however, improvements in research, including personalized medicine and genetically-based therapies, can give hope of a better future.
Patients and families must stay educated, develop effective support networks, and advocate for better research to handle the challenges of this syndrome.
References
[1] Audia S, Grienay N, Mounier M, Michel M, Bonnotte B. Evans’ Syndrome: From Diagnosis to Treatment. J Clin Med. 2020 Nov 27;9(12):3851. doi: 10.3390/jcm9123851. PMID: 33260979; PMCID: PMC7759819.
[2] Bussel JB.Evans Syndrome. National Organization for Rare Disorders (NORD). 2021.
[3] Hansen DL, Möller S, Andersen K, Gaist D, Frederiksen H. Evans syndrome in adults – incidence, prevalence, and survival in a nationwide cohort. Am J Hematol. 2019 Oct;94(10):1081-1090. doi: 10.1002/ajh.25574. Epub 2019 Aug 9. PMID: 31292991.
[4] Bussel JB.Evans Syndrome. NORD. 2021.
[5] Evans RS, Takahashi K, Duane RT, Payne R, Liu C.Primary thrombocytopenic purpura and acquired hemolytic anemia; evidence for a common etiology. AMA Arch Intern Med. 1951;87(1):48–65.
[6] Jaime-Pérez JC, Aguilar-Calderón PE, Salazar-Cavazos L, Gómez-Almaguer D.Evans syndrome: Clinical perspectives, biological insights and treatment modalities. J Blood Med. 2018;9:171–184.
[7] Teachey DT, Seif AE.Primary autoimmune cytopenias and Evans syndrome: pathophysiology and treatment. Hematology Am Soc Hematol Educ Program. 2010;2010:354–361.
[8] Jaime-Pérez JC, et al.Evans syndrome: Clinical perspectives, biological insights and treatment modalities. J Blood Med. 2018;9:171–184.
[9] Mathew P, Chen G, Wang W.Evans syndrome: results of a national survey. J Pediatr Hematol Oncol. 1997;19(5):433–437.
[10] Michel M, Chanet V, Dechartres A, et al.The spectrum of Evans syndrome in adults: new insight into the disease based on the analysis of 68 cases. Blood. 2009;114(15):3167–3172.
[11] Aladjidi N, Fernandes H, Leblanc T, et al.Evans syndrome in children: long-term outcome in a prospective French national observational cohort. Front Pediatr. 2015;3:79.
[12] Lee S, Kim YJ.Evans syndrome: clinical features and treatment outcomes. Korean J Hematol. 2011;46(4):252–258.
[13] StatPearls Publishing.Evans Syndrome. NCBI Bookshelf. 2023.
[14] Jaime-Pérez JC, et al.Evans syndrome: Clinical perspectives, biological insights and treatment modalities. J Blood Med. 2018;9:171–184.
[15] .Norton A, Roberts I.Management of Evans syndrome. Br J Haematol. 2006;132(2):125–137.
[16] .Teachey DT, Seif AE.Primary autoimmune cytopenias and Evans syndrome: pathophysiology and treatment. Hematology Am Soc Hematol Educ Program. 2010;2010:354–361.
[17] .Mathew P, Chen G, Wang W.Evans syndrome: results of a national survey. J Pediatr Hematol Oncol. 1997;19(5):433–437.
[18] .Aladjidi N, et al.Evans syndrome in children: long-term outcome in a prospective French national observational cohort. Front Pediatr. 2015;3:79.
[19] Michel M, et al.The spectrum of Evans syndrome in adults: new insight into the disease based on the analysis of 68 cases. Blood. 2009;114(15):3167–3172.
[20] Jaime-Pérez JC, et al.Evans syndrome: Clinical perspectives, biological insights and treatment modalities. J Blood Med. 2018;9:171–184.
[21] Teachey DT, Seif AE.Primary autoimmune cytopenias and Evans syndrome: pathophysiology and treatment. Hematology Am Soc Hematol Educ Program. 2010;2010:354–361.