
{kind=link}

Prostate Enlargement BPH Prostate enlargement starts so gradually that most men do not even notice it happening. The clinical term is benign prostatic hyperplasia (BPH), benign meaning non-cancerous, and hyperplasia meaning an increase in the number of cells, causing the gland to enlarge. It is one of the most common conditions in men over 50, yet most men affected do not know what the cause of their symptoms is; it often gets mistaken for a normal part of aging.
By the age of 60, around 50% of men have BPH, and this figure jumps to a straight 90% by the age of 85.[1] But BPH is not the only cause of an enlarged prostate; conditions like prostate cancer and prostatitis (inflammation) can also cause the same, which is why self-diagnosis should be avoided, and symptoms should always be medically evaluated.
What Does the Prostate Do?: Prostate Enlargement BPH
The prostate is a walnut-sized gland, part of the male reproductive system, and its primary function is to produce seminal fluid that nourishes and transports sperm. It has two main growth phases during a man’s lifetime: the first during puberty, and the second begins in mid-adulthood (around 40–50 years of age). This second phase continues slowly for the rest of a man’s life, and it is this phase that results in BPH in many men.
What makes the size of the prostate so important is its anatomical location: it sits directly below the bladder and wraps around the urethra (the tube that transports urine). When the gland grows, it squeezes the urethra, compressing its lumen and increasing the resistance the bladder needs to work against. This is why urinary symptoms are the hallmark of BPH. Of course, any other condition that causes prostate enlargement will also present with these symptoms.

Normal male pelvic anatomy:Key structures include the urethra, which passes directly through the center of the prostate, and the seminal vesicles.
Causes Of Prostate Enlargement
There is not a single decisive cause, and in most cases, it is not caused by sexual activity, diet, or behavior. The abnormal enlargement is a consequence of age and hormonal changes that virtually every man undergoes to some degree.
The reason for this growth is purely hormonal. As men age, testosterone levels in the body gradually drop, but at the same time, another hormone, dihydrotestosterone (DHT), is produced more and continues to accumulate in prostatic tissue. DHT is a stronger androgenic hormone than testosterone and is converted from testosterone by the enzyme 5-alpha reductase. When it accumulates in the prostatic tissue, it stimulates cell proliferation within the tissue.[2]
At the same time as testosterone declines, there is a relative increase in oestrogen, which sensitises prostate tissue to the growth-promoting effects of DHT.
Risk Factors
There are several factors that make a person more susceptible to BPH, for example:
- Age is the strongest factor; BPH is rare before the age of 40
- Family history in first-degree relatives significantly increases risk
- Abdominal obesity is associated with higher estrogen levels and insulin resistance, both of which influence prostate growth
- Type 2 diabetes and metabolic syndrome are also associated with a higher risk and more severe symptoms.[3]
- Lifestyle habits also play a role; physically active men have consistently lower rates of symptomatic BPH than men with a sedentary lifestyle
- Erectile dysfunction and BPH frequently coexist, often sharing pathophysiology and overlapping risk factors
Symptoms of Enlarged Prostate
The symptoms of BPH are of two types: those caused by the blockage itself, and those caused by changes in the bladder because of that blockage. It is important to note that the severity of symptoms does not always match the extent of the enlargement. Also, the symptoms develop so gradually in the beginning that many men live with them for several years before seeking help.
Even when they notice the symptoms, they might ignore them because they are embarrassed or because they assume it is normal aging.
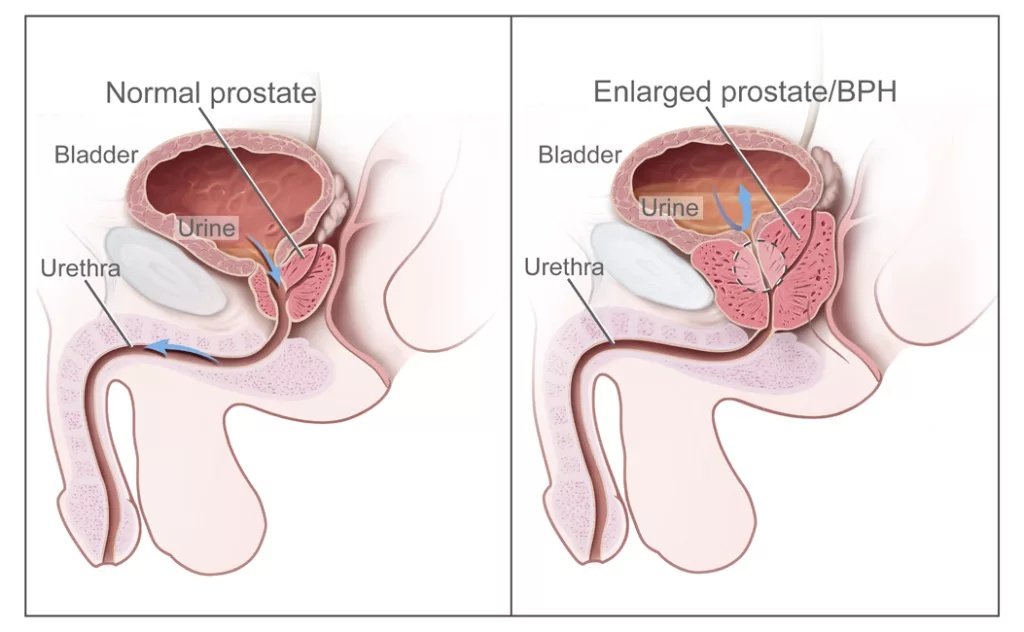
Obstructive symptoms of an enlarged prostate: A normal prostate (left) allows urine to flow freely through the urethra. In BPH (right), the enlarged gland compresses the urethra, increasing resistance and causing urinary symptoms. (Image Courtesy: National Cancer Institute, viaWikimedia Commons, Public domain)
Obstructive symptoms
These are voiding symptoms caused directly by urethral compression:
- A weak or slow urine stream is often the first noticed symptom
- Hesitancy, difficulty initiating urination despite the urge
- Intermittent stream (stopping and starting)
- Sensation of incomplete bladder emptying (post-void residual urine)[4]
- Terminal dribbling, i.e., the stream ends slowly rather than cleanly
Irritative Symptoms
These are symptoms caused by bladder changes because of outlet obstruction. Structurally, when the bladder has to work against increasing resistance to empty itself, its wall thickens and becomes overactive. These symptoms often have a psychological impact on the patients, and this is usually when they reach out to a medical professional.
- Nocturia, which is waking up at night to urinate. This is one of the most reported symptoms and one that understandably affects the quality of life.[5]
- Increased urinary frequency during the day
- A sudden, strong, difficult-to-defer urge to urinate, instead of the usual gradual urge
- Urge incontinence, i.e., leaking urine before reaching the bathroom[6]
To assess the severity of symptoms in a patient, we use a 7-item self-reported questionnaire, called the IPSS (International Prostate Symptom Score). A score of 0-7 points indicates mild disease, 8-19 is moderate, and 20-35 is severe disease.[7]
Complications of Untreated or Advanced BPH
Even though the condition is benign and the symptoms themselves might not seem that severe, BPH is not a disease that can be ignored. Doctors warn of several long-term complications that may develop if left untreated:
- Acute urinary retention: a sudden, complete inability to urinate; this is a medical emergency that requires catheterization
- Recurrent urinary tract infections because incomplete bladder emptying creates a reservoir for bacterial growth
- Bladder stones because of stagnant residual urine
- Chronic overwork of the bladder results in detrusor muscle dysfunction[8]
- Hydronephrosis: In severe cases, the backflow affects the kidneys

Clinical complications arising from chronic, untreated Benign Prostatic Hyperplasia. Persistent obstruction of the prostatic urethra leads to urinary stasis and residual volume, increasing the risk of recurrent Urinary Tract Infections (UTIs) and the formation of bladder stones. In advanced cases, the back-pressure can extend to the upper urinary tract, causing hydronephrosis (dilation of the kidneys) and potential long-term renal impairment.
How is an Enlarged Prostate Diagnosed?
Diagnosis of prostate enlargement and ruling out other conditions to diagnose BPH is not a very complex procedure; the assessment is straightforward, and most of it happens in a GP clinic.
History:
First step is the medical history of the patient: symptoms, their duration, frequency, and what impact they have on the patient’s quality of life. The IPSS then gives it a standardized score.
Digital Rectal Examination:
This is the part of the examination that patients dread, but it’s a simple, short procedure where the clinician inserts a gloved finger rectally to feel the prostate for size, shape, and consistency. The main goal is not just the size but the texture, which might raise concern for malignancy.
Urine Tests:
A urine analysis as well as culture is done to exclude an infection or the presence of blood in the urine.
Prostate-specific Antigen:
PSA is produced by prostate cells and is elevated in all relevant conditions like BPH, prostatitis, and prostate cancer, so an elevated PSA is not a diagnosis in itself, but suggests that further investigation might be needed.
There isn’t a definite cutoff, but a PSA >4.0 ng/mL is often the threshold for further testing. A very high PSA level (>10 ng/mL) or a rapid increase (PSA velocity) is more suggestive of cancer.[9] Another distinction can be made by looking at the ratio of free-to-total PSA; a higher percentage of free PSA is more indicative of BPH than prostate cancer.
Bladder Ultrasound:
A bladder ultrasound is the best way to measure post-void residual urine volume, if any.
Uroflowmetry:
If a more precise urine flow measure is needed, the uroflowmetry is a flow-measuring device in which the patient urinates. It produces an objective measure of flow rate and pattern. Generally, a peak flow rate below 10ml/second suggests there is a significant obstruction to urine outflow.
These investigations are enough to assess an uncomplicated prostate enlargement; if complications or advanced disease are suspected, cystoscopy or renal function tests may be needed.
Enlarged Prostate Treatment
The treatment of an enlarged prostate is not a one-size-fits-all; it has to be targeted to a patient based on how severe the symptoms are, whether complications are present, and what the patient’s priorities are. Mild, manageable symptoms may not need medication at all; lifestyle changes alone can make enough of a difference.
Overall, there is a wider range of treatment options than most people realise. Treatment may range from simple monitoring to medication or surgery.
Monitoring for Mild Symptoms
When the disease is in the early stages, and the symptoms do not significantly affect the quality of life, active monitoring might be enough, but the severity needs to be reassessed annually. Along with monitoring, lifestyle modifications may be needed:
- To reduce nocturia, fluid intake should be reduced in the evening
- Intake of caffeine and alcohol should be limited, as both can irritate the bladder and increase urgency
- Developing a habit of double voiding, i.e, urinating once, waiting a moment, then trying again in an attempt to improve bladder emptying
- Avoiding medications that worsen symptoms, like antihistamines, decongestants, even some antidepressants
Medications for Moderate to Severe Symptoms
For moderate to severe symptoms where lifestyle modifications aren’t enough, there are several drugs that can be prescribed.
- Alpha-blockers like tamsulosin can improve urine flow by relaxing smooth muscles in the prostate and bladder neck, within days to weeks.[10] However, they do not shrink the gland and have side effects, most notably, dizziness and retrograde ejaculation. This is where the semen from the prostate goes backward into the bladder instead of emerging from the penis during climax; it is caused by the bladder neck failing to close.
- 5-alpha reductase inhibitors (5-ARIs) like finasteride are the drugs of choice in men who have significantly enlarged prostates. They shrink the gland over 3-6 months by blocking the conversion of testosterone to DHT. Side effects include reduced libido and erectile dysfunction, so patients need to be counselled beforehand.[11]
- Since alpha-blockers and 5-ARIs are separately effective in their own domains, a combination of both works best for men with larger prostates and more severe symptoms
- Anticholinergics / beta-3 agonists (mirabegron) are prescribed for men whose symptoms are predominantly more irritative (urgency, frequency, nocturia) rather than obstructive. They target bladder overactivity, rather than the prostate itself.
- PDE5 inhibitors such as tadalafil are useful in men who also have erectile dysfunction as they address both simultaneously.
Surgical Options for Severe Symptoms
In cases where the symptoms are too severe for medications or there are complications, minimally invasive procedures and surgery are indicated.
- The historical gold standard is still TURP (transurethral resection of the prostate). A scope is inserted into the urethra, and prostatic tissue is removed. The procedure is minimally invasive in that no external incision is involved. TURP is a highly effective procedure with proven efficacy, but risks sometimes include retrograde ejaculation, erectile dysfunction, or incontinence.
- Laser therapies are increasingly replacing TURP as the non-invasive treatment of choice, and are more effective for large prostates.[12]
- Another option is Urolift in men with moderately enlarged prostates who want to avoid retrograde ejaculation. It involves inserting small implants to pull enlarged prostate lobes away from the urethra without removing tissue.
- Another option for men looking for a minimally invasive procedure is Rezum: an office-based procedure where water vapors (steam) are inserted into the prostatic tissue to shrink it. The vapours kill the excess prostate tissue, after which the body naturally absorbs the dead cells.
- A more invasive option is an open or robotic prostatectomy. It is reserved for very large prostates where minimally invasive endoscopic approaches are not feasible.

UroLift procedure: Small implants are delivered through the prostatic urethra under cystoscopic guidance (C–D). Once secured, the implants retract and hold the obstructing lobes away from the urethral lumen (E–F), restoring urine flow without removing prostate tissue (G). (Image Courtesy: Roehrborn, C.G., Chin, P.T. & Woo, H.H. The UroLift implant: mechanism behind rapid and durable relief from prostatic obstruction. Prostate Cancer Prostatic Dis 25, 79–85 (2022). Available fromNature, licensed under CC by 4.0)
Final Words
Prostate health is something that is rarely discussed openly, but with how prevalent prostate enlargement is in men of old age, patient education and public awareness are very important. So many men choose to live with the symptoms of an enlarged prostate out of embarrassment. But this delay is what turns a manageable condition into a complicated one that has a significant psychological impact.
It is important to spread awareness that BPH is not cancer; it is a common, well-understood condition with a wide range of effective treatments available, most of them minimally invasive. If symptoms go from simple urgency to a sudden complete inability to urinate or there is blood in the urine, it means a same-day emergency assessment is needed.
References
[1] Siqueira M. H. B. (2025). Risk factors for benign prostatic hyperplasia: a comprehensive review. Revista da Associacao Medica Brasileira (1992), 71(6), e20250343.
[2] Swerdloff, R. S., Dudley, R. E., Page, S. T., Wang, C., & Salameh, W. A. (2017). Dihydrotestosterone: Biochemistry, Physiology, and Clinical Implications of Elevated Blood Levels. Endocrine reviews, 38(3), 220–254.
[3] Ngai, H. Y., Yuen, K. S., Ng, C. M., Cheng, C. H., & Chu, S. P. (2017). Metabolic syndrome and benign prostatic hyperplasia: An update. Asian journal of urology, 4(3), 164–173.
[4] Ballstaedt L, Leslie SW, Woodbury B. Bladder Post Void Residual Volume. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539839/
[5] Jin, M. H., & Moon, duG. (2008). Practical management of nocturia in urology. Indian journal of urology : IJU : journal of the Urological Society of India, 24(3), 289–294.
[6] Miller, S. W., & Miller, M. S. (2011). Urological disorders in men: urinary incontinence and benign prostatic hyperplasia. Journal of pharmacy practice, 24(4), 374–385.
[7] Ahmed, A. ., Khan, M. S., Ahmed, S. N., Imran Farid, M. ., Inam, Q. A. ., & Ahmad, I. . (2025). International Prostate Symptom Score (IPSS) Correlation with Sonographic Prostate Size. Journal of Neonatal Surgery, 14(31S), 939–943.
[8] Komninos, C., & Mitsogiannis, I. (2014). Obstruction-induced alterations within the urinary bladder and their role in the pathophysiology of lower urinary tract symptomatology. Canadian Urological Association journal = Journal de l’Association des urologues du Canada, 8(7-8), E524–E530.
[9] Vickers, A. J., Wolters, T., Savage, C. J., Cronin, A. M., O’Brien, M. F., Pettersson, K., Roobol, M. J., Aus, G., Scardino, P. T., Hugosson, J., Schröder, F. H., & Lilja, H. (2009). Prostate-specific antigen velocity for early detection of prostate cancer: result from a large, representative, population-based cohort. European urology, 56(5), 753–760.
[10] Lepor H. (2007). Alpha blockers for the treatment of benign prostatic hyperplasia. Reviews in urology, 9(4), 181–190.
[11] Chislett, B., Chen, D., Perera, M. L., Chung, E., Bolton, D., & Qu, L. G. (2023). 5-alpha reductase inhibitors use in prostatic disease and beyond. Translational andrology and urology, 12(3), 487–496.
[12] Shvero, A., Calio, B., Humphreys, M. R., & Das, A. K. (2021). HoLEP: the new gold standard for surgical treatment of benign prostatic hyperplasia. The Canadian journal of urology, 28(S2), 6–10.