
{kind=link}

What Is Infectious Colitis?: Infectious Colitis Infection
Infectious Colitis Infection Infectious colitis is inflammation and swelling of the colon due to the invasion of harmful microorganisms into the digestive system. The colon or large intestine is the last section of your digestive tract, where water and electrolytes are absorbed, and stool is formed, before waste leaves the body. When infectious agents attack this region, an immune reaction takes place, resulting in an inflamed lining of the colon with a number of unpleasant symptoms.
Infectious colitis is a widespread digestive disorder affecting millions of individuals annually in the world. In contrast to chronic inflammatory bowel diseases (ulcerative colitis or Crohn’s disease), infectious colitis is an acute disease. This implies that it occurs abruptly and tends to disappear within days to weeks after the infection has been removed from the body.
Causes of Infectious Colitis
Knowledge of the causal factors of infectious colitis may assist you in preventing it. The condition occurs when some pathogenic microorganisms get into your digestive system, and normally, it happens as a result of contaminated food or water. Bacteria are the most frequent cause of infectious diarrhea globally, though the exact percentage varies by region and study.
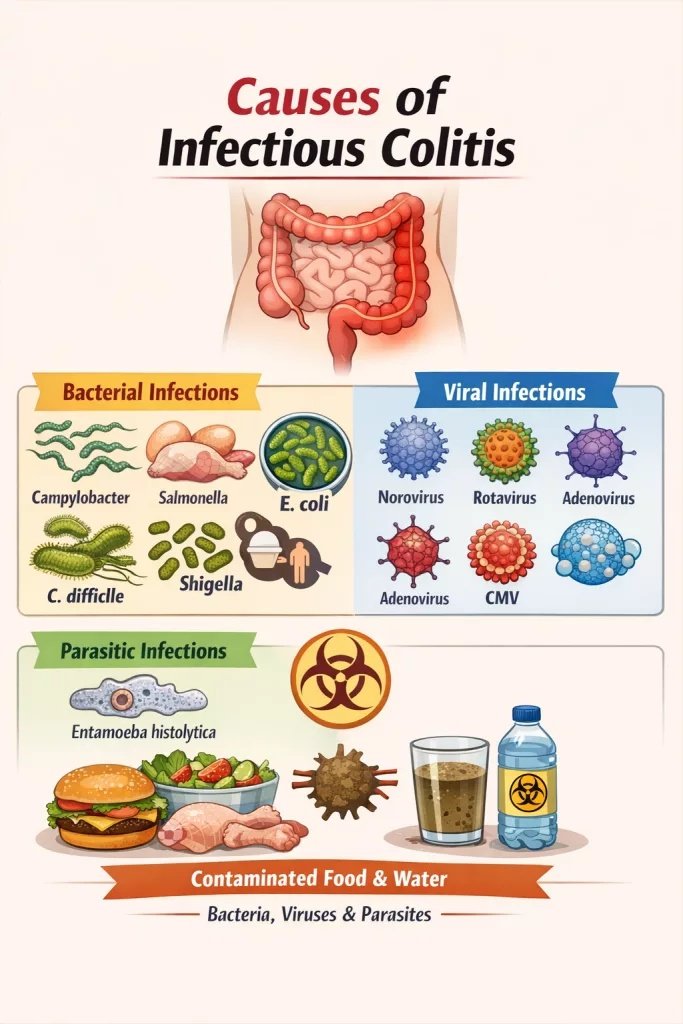
Common causes of infectious colitis include bacteria, viruses, and parasites transmitted through contaminated food or water.
Bacterial Infections
The majority of the infections are bacterial. Many types of bacteria may be the cause of this condition:
- Campylobacter jejuni has been reported to be the major bacterial cause of diarrheal disease globally, with a prevalence rate of 25-30 in 100,000 individuals. Reported incidence rates vary widely by region, and true prevalence is likely underestimated due to underreporting.The bacteria are commonly present in undercooked poultry and raw milk.
- In the United States, Salmonella infections result in about 1.2 million cases every year. These bacteria are transmitted via contaminated eggs, poultry, and produce. Individuals with disorders such as sickle cell anemia or people who consume immunosuppressive drugs are at greater risk of Salmonella infection.
- Escherichia coli (E. coli) is a bacterium that may severely make a person ill, especially the O157:H7 strain. It is a very dangerous strain that only takes 10-100 organisms to infect and is spread most often by undercooked ground beef.
- Shigella bacterium is transmitted via the fecal-oral route and has an annual incidence of about half a million in the United States, but globally has been estimated to be about 165 million cases annually.
- Clostridioides diff (C. diff) is an exception since this bacterium is a normal inhabitant of the intestines. But when antibiotics destroy the good bacteria, which usually check C. diff, it can multiply further and cause damage to the colon through the production of toxins. Recent exposure to antibiotics and hospitalization are also significant risk factors for C. diff infection.
Viral Infections
Viruses are a rare cause of infectious colitis, although in certain cases, they can cause the condition. The key offenders are:
- Norovirus
- Rotavirus
- Adenovirus
- Cytomegalovirus (CMV)
Parasitic Infections
The amoebic colitis may be caused by parasites such as Entamoeba histolytica, which may invade the colonic mucosa. These infections are more prevalent in the developing world, which is poorly sanitized, but may occur in travelers who visit the endemic world.
Sexually Transmitted Infections
Sexually transmitted diseases may also involve the rectum in some population groups, especially in men who have sex with men, and individuals with HIV infection, leading to colitis-like symptoms. These are Neisseria gonorrhoeae, Chlamydia trachomatis, herpes simplex virus, and Treponema pallidum (the cause of syphilis).
Is Infectious Colitis Contagious?
Yes, infectious colitis is contagious, but the contagiousness is determined by the organism that induces the infection. Infectious colitis is mostly transmitted by person-to-person contact, and it is therefore important to learn how it occurs.
How Does it Spread?
The main modes of transmission are:
The most widespread route is through the fecal-oral. It happens when feces that contain the infectious organism in microscopic volumes are passed to the mouth, usually by contaminated hands, food, or water.
The sources of infection include contaminated food and water. During food processing or preparation, bacteria such as Salmonella and E. coli tend to contaminate food. The infectious agents can also be transmitted by drinking untreated water in lakes, ponds, or other contaminated water sources in the municipal supplies.
Person-to-person contact is the means of spreading numerous infections, particularly in households, daycare centres, and health facilities. Touching any objects touched by an infected individual and thereafter touching your mouth is enough to infect you.
Objects and surfaces that are shared may contain infectious organisms. Doorknobs, bathroom, and utensils used by more than one person, as well as personal tools such as toothbrushes, can also be carriers of infection unless they are well cleaned.
Importantly, some individuals may continue to shed pathogens and remain contagious even after symptoms improve. That is why it is necessary to practice good hygiene during your recovery period.
Infectious Colitis Symptoms
The symptoms of infectious colitis may be different in different people and depend on what organism is the one to causes the infection. The majority of individuals acquire symptoms within hours to days of exposure to the infectious agent.
Primary Symptoms
The characteristic features of infectious colitis are:
- Diarrhea: This is generally the most apparent symptom, which may be loose and watery stool to frequent and diarrheal bowel movements. The diarrhea may contain blood, mucus, or pus.
- Pain in the abdomen and cramping: A lot of individuals complain of the lower-abdominal pains that come in waves.
- Fever: An elevated body temperature often accompanies the infection as your immune system fights the invading organisms.
- Urgency and tenesmus: You can have the feeling that you have an urgent need to pass a bowel movement that is very strong, even though there is no content in the bowel.
- Blood in the stool: In contrast to simple gastroenteritis, infectious colitis is the cause of bloody diarrhea as a result of inflammatory processes and injury of the colon mucosa.
Additional Symptoms
Others can also experience:
- Nausea and vomiting
- Loss of appetite
- Fatigue and weakness
- Symptoms of dehydration (dry mouth and reduced urination, dizziness, etc.)
- Headache
- Weight loss
When to Seek Medical Care?
You should visit a doctor in case of:
- Diarrhea for more than three days
- Abdominal pain/tenderness is severe
- Blood or pus in your stool
- High fever (above 101.5°F or 38.6°C)
- Dehydration (vital feeling of thirstiness, urine of very dark color, feeling of weakness, loss of consciousness)
The Difference Between Infectious Colitis and Gastroenteritis
The two conditions are known to result in diarrhea, stomachache, and even fever. Nevertheless, these two conditions have certain significant differences.
| Feature | Infectious Colitis | Gastroenteritis |
|---|---|---|
| Location of Inflammation | Affects only the colon (large intestine) | Affects both the stomach and intestines |
| Primary Symptoms | Bloody diarrhea, rectal pain, urgency | Watery diarrhea, nausea, vomiting |
| Blood in Stool | Common | Rare or absent |
| Nausea/Vomiting | Less common | Very common |
| Duration | Usually, 7 days to several weeks | Typically 1-3 days (some bacterial gastroenteritis cases can last longer than 3 days, if untreated) |
| Common Causes | Bacteria (47% of cases), viruses, parasites | Primarily viruses (especially norovirus) |
| Severity | Often more severe | Usually milder |
Diagnosis of Infectious Colitis
The aim of diagnosis is not merely to make sure that you have infectious colitis, but also to diagnose the particular organism that has caused it so that it can be treated properly.
Medical History and Physical Examination
Your doctor will enquire about how and when you began to have your symptoms, and what changes have taken place. They will enquire about your last travels, particularly to places with questionable sanitation, and ask about your recent diet, specifically, eating undercooked meat, unpasteurized milk items, and food from a potentially hazardous source.
The physician will also be interested in knowing about the recent antibiotic use because, in some cases, it can provoke some infections. Your health history and any conditions that impact your immunity, as well as the medications that you are taking, will be checked. Upon this discussion physical examination will be done to evaluate signs of dehydration, abdominal inspection to see tenderness, and other signs that may indicate the level of the illness.
Laboratory Tests
Stool Studies are the key to the diagnosis of infectious colitis.
- Stool culture: It is a simple test, but regrettably, stool cultures only determine the causative organism in less than half of the cases.
- Molecular tests using PCR: These are sophisticated tests that can identify bacterial, viral, and parasitic DNA faster and more precisely than conventional cultures, and the results can be given within 24 hours.
- Toxin testing: In the case of C. diff, the bacteria are not targeted; instead, the toxin that the bacteria are producing is targeted by the laboratory.
- Fecal leukocytes/lactoferrin: The markers are evidence of inflammation and may be used to differentiate between inflammatory and non-inflammatory diarrhea of colitis.
- Examination of ovum and parasites: In case of the suspicion of parasitic infection, microscopic analysis of stool can be used to determine the presence of parasites or their eggs.
Blood Tests assist in determining the extent of the infection and exclusion of complications:
- Complete blood count (CBC)
- C-reactive protein (CRP)
- Erythrocyte sedimentation rate
- Electrolytes, renal, and liver function tests.
- Albumin levels
Imaging Studies
Abdominal and pelvic CT can identify thickening of the colon wall that is a sign of inflammation and can be used to identify severe complications such as toxic megacolon or perforation. These radiographic examinations also indicate the extent and distribution of involvement of the colon and the presence of inflammation outside the colon.
Endoscopic Examination
Endoscopy is not routinely required but may be useful when the diagnosis is unclear. A direct examination of the inner lining of the colon is done by colonoscopy or flexible sigmoidoscopy, which is particularly beneficial when the stool cultures are negative or when the physician has to distinguish between infectious colitis and inflammatory bowel disease.
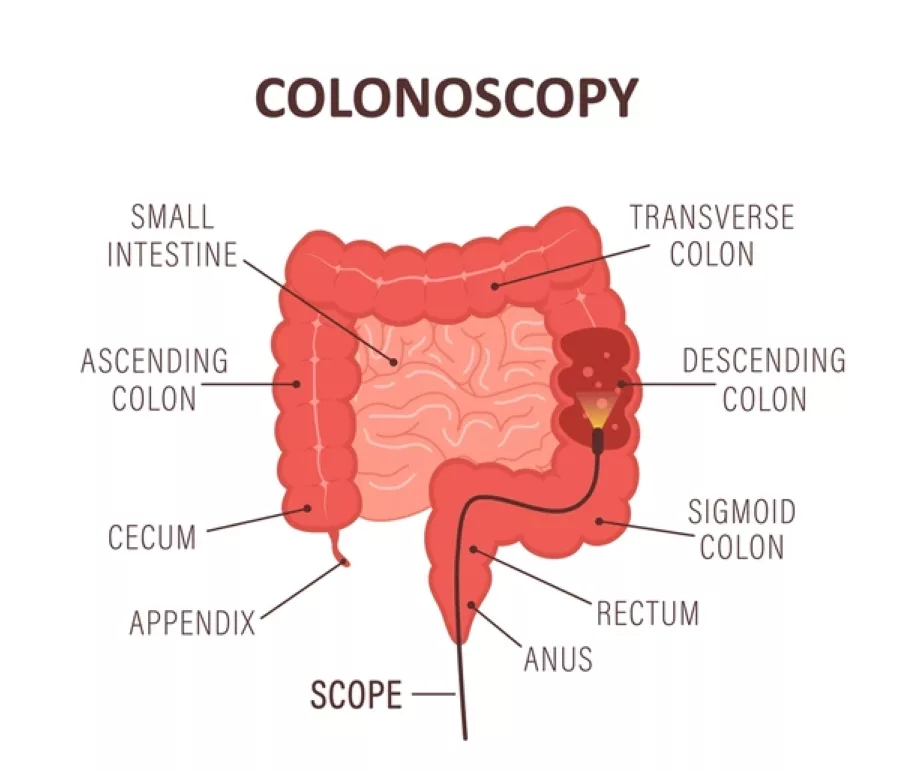
Illustration of a colonoscopy used to examine colonic inflammation and bowel changes in infectious colitis.
Another diagnostic data comes in the form of biopsies performed during a colonoscopy. Biopsy findings in infectious colitis typically show acute inflammation without chronic architectural distortion.
Treatment Approaches for Infectious Colitis
Mostly, patients of infectious colitis will resolve their disease without specific therapy, although appropriate care can greatly minimize the symptoms and help avoid complications.
Supportive Care
If you have severe diarrhea, then you need oral rehydration. Patients are advised to consume as much fluid as possible, which contains electrolytes (e.g, oral rehydration solutions, broth, sports drinks). In extreme situations when oral feeding is not tolerated, intravenous fluids can be used to keep one hydrated and electrolytes balanced.
Rest is also essential in the recovery stage. The body requires energy to combat the infection, and therefore, you should not engage in any hard work sessions, and also give yourself time to rest.
The diet should be bland and easy to digest, which may be achieved with the help of bananas, rice, applesauce, and toast (the BRAT diet). Although more recent guidelines propose to resume a normal diet gradually and in the amounts that can be tolerated.
Antimicrobial Therapy: When Antibiotics Are Required
Not every case of infectious colitis needs antibiotics, and they are even detrimental in some cases. Antimicrobial therapy depends on the organism causing and the severity of the disease.
Antibiotic therapy should be considered in infectious colitis when there is:
- Severe disease (high fever, systemic toxicity, severe abdominal pain, or dysentery)
- Immunocompromised state, advanced age, or significant comorbidities
- Confirmed or strongly suspected bacterial or parasitic pathogens known to benefit from treatment
- Healthcare-associated infections such as Clostridioides difficile.
Azithromycin or ciprofloxacin may be used for severe Campylobacter or Shigella infections, while antibiotic therapy is reserved for high-risk or severe cases of non-typhoidal Salmonella. In the case of Clostridioides difficile (C. diff) colitis, the treatment is often to stop the causative antibiotic where possible and then to administer therapy using oral vancomycin or fidaxomicin. Mild cases can be treated with metronidazole,but it is no longer recommended as first-line therapy for C. difficile, except in limited situations where preferred agents are unavailable.
The treatment of parasitic diseases such as Giardia or Entamoeba histolytica needs certain antiparasitic drugs like metronidazole or tinidazole.
It is also worth mentioning that in some cases, antibiotics are not recommended, especially in the case of enterohemorrhagic E. coli (EHEC), because it can cause the development of hemolytic uremic syndrome, one of the most severe complications.
Symptomatic Management
Symptom management can be of great use when the underlying infection is treated and can make patients feel much better. Anti-diarrheal drugs such as loperamide should also be used with caution and are not usually given in the presence of bloody diarrhea, high fever, or a possible invasive pathogen, since retarded intestinal motility may aggravate the infection.
Acetaminophen can be used to manage pain in cases of fever and cramping. But NSAIDs should be applied sparingly because sometimes, they irritate the gastrointestinal tract. Probiotics could be used to restore normal gut flora, especially following antibiotic therapy, but their use during acute infection has been contradictory.
Preventing Infectious Colitis
The prevention of infectious colitis depends mostly on good hygiene and the ability to make wise food decisions.
- The most successful preventive measure is hand hygiene. Handwashing with soap and water prior to eating, after using the washroom, and after touching raw food can greatly contribute towards lowering the risk of infections. Hand sanitizers can be used, yet soap and water are a better option against some pathogens.
- Practices of food safety are also important. When cooking meat, poultry, and eggs, do not leave them uncooked, because they are dangerous to consume. The same is the case with unpasteurized dairy products. Washing of fruits and vegetables is mandatory.
- It is important to store food properly. Perishables need to be refrigerated immediately. Different cutting boards must be used with raw meat and vegetables, and in case of doubt, discard them.
Conclusion
Infectious colitis is an unpleasant and potentially severe disorder, but it is manageable. And in most cases, it is curable through proper treatment. Being aware of the causal factors, the occurrence of the symptoms at the initial stages, and being able to know when to approach a medical practitioner may make a huge difference in your healing process. It is possible to greatly decrease your risk of developing this condition by practicing good hygiene, observing food safety measures, and taking due precautions during traveling.
Keep in mind that infectious colitis is not the same as chronic inflammatory bowel disease. It is often a transient disease that is the result of a certain infection. Most individuals can be treated and cared for to live a normal life.
References
[1] Lewis JD, Parlett LE, Jonsson Funk ML, et al. Incidence, prevalence, and racial and ethnic distribution of inflammatory bowel disease in the United States. Gastroenterology. 2023;165(5):1197–1205.e2. doi:10.1053/j.gastro.2023.07.003
[2] Kaakoush NO, Castaño-Rodríguez N, Mitchell HM, Man SM. Global epidemiology of Campylobacter infection. Clin Microbiol Rev. 2015;28(3):687-720.
[3] Rangel JM, Sparling PH, Crowe C, Griffin PM, Swerdlow DL. Epidemiology of Escherichia coli O157:H7 outbreaks, United States, 1982-2002. Emerg Infect Dis. 2005;11(4):603-609.
[4] Centers for Disease Control and Prevention.Shigella – epidemiology and risk factors. Atlanta (GA): CDC; 2023. Available from: https://www.cdc.gov/shigella/index.html
[5] Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825-834.
[6] Ramani S, Atmar RL, Estes MK. Epidemiology of human noroviruses and updates on vaccine development. Curr Opin Gastroenterol. 2014;30(1):25-33.
[7] Haque R, Huston CD, Hughes M, Houpt E, Petri WA Jr. Amebiasis. N Engl J Med. 2003;348(16):1565-1573.
[8] Thapar N, Sanderson IR. Diarrhoea in children: an interface between developing and developed countries. Lancet. 2004;363(9409):641-653.
[9] Riddle MS, DuPont HL, Connor BA. ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults. Am J Gastroenterol. 2016;111(5):602-622.
[10] Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin Infect Dis. 2017;65(12):e45-e80.
[11] Khare R, Espy MJ, Cebelinski E, et al. Comparative evaluation of two commercial multiplex panels for detection of gastrointestinal pathogens by use of clinical stool specimens. J Clin Microbiol. 2014;52(10):3667-3673.
[12] Prideaux L, De Cruz P, Ng SC, Kamm MA. Serological antibodies in inflammatory bowel disease: a systematic review. Inflamm Bowel Dis. 2012;18(7):1340-1355
[13] Nostrant TT, Kumar NB, Appelman HD. Histopathology differentiates acute self-limited colitis from ulcerative colitis. Gastroenterology. 1987;92(2):318-328.
[14] World Health Organization. The Treatment of Diarrhoea: A Manual for Physicians and Other Senior Health Workers. 4th rev. Geneva: WHO; 2005.
[15] Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31(5):431-455.
[16] Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America clinical practice guidelines for the diagnosis and management of infectious diarrhea.Clin Infect Dis. 2017;65(12):e45–80. doi:10.1093/cid/cix669.
[17] Szajewska H, Canani RB, Guarino A, et al. Probiotics for the prevention of antibiotic-associated diarrhea in children. J Pediatr Gastroenterol Nutr. 2016;62(3):495-506.
[18] Aiello AE, Coulborn RM, Perez V, Larson EL. Effect of hand hygiene on infectious disease risk in the community setting: a meta-analysis. Am J Public Health. 2008;98(8):1372-1381.