
{kind=link}

Inguinal hernia surgery is one of the most commonly performed general surgical procedures worldwide and aims to reinforce a weakened area of the abdominal wall to relieve symptoms and prevent complications. The most common type of hernia, which occurs in both males and females, is the inguinal hernia, which is the protrusion of abdominal contents through the inguinal canal due to a pre-existing weakness.
The gold standard approach to the repair of these hernias and prevention of severe complications is surgery. As many as 800,000 inguinal hernia repair surgeries are done in the United States alone each year, and about 20 million are done in the world.
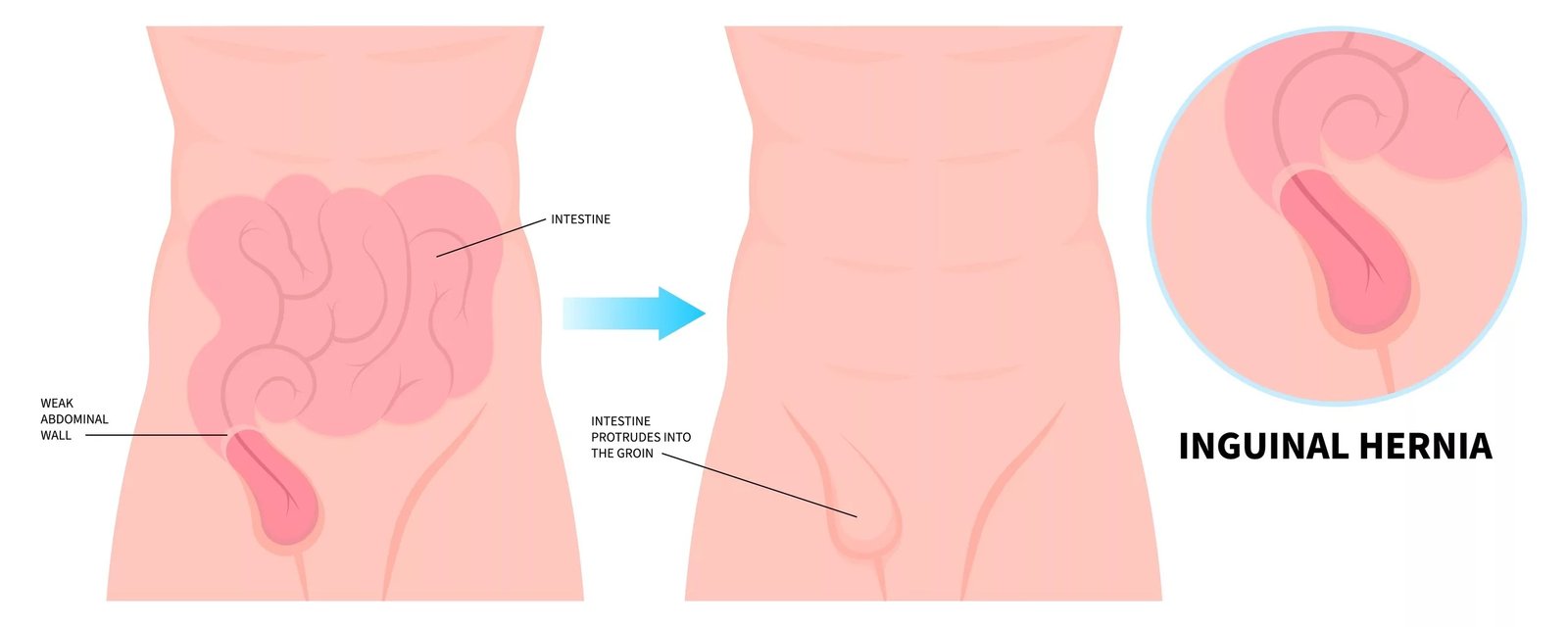
Formation of an inguinal hernia
What is Inguinal Hernia Surgery?
Inguinal hernia surgery is a process that aims at repairing the weak point or gap in the abdominal wall through which intestine or other tissue is protruding. The inguinal canal is an area in the lower abdominal wall that is close to the pubic bone. When organs herniate through this weakened part, there is a bulge that patients would experience in the groin, which is often accompanied by pain or discomfort.
There is a marked sex difference in lifetime risk: approximately 27% of men and 3% of women develop an inguinal hernia during their lifetime. This disparity exists because, in males, the descent of the testes through the inguinal canal during fetal development leaves a potential area of weakness in the abdominal wall.
Types of Inguinal Hernia Surgery
Knowledge of the various methods of surgery allows patients and doctors to decide on the best method of treatment. Inguinal hernia surgery is of the following types: open repair, laparoscopic surgery, and robotic surgery. All the methods have their own strengths and deliberations.
Open Hernia Repair
In open surgery, the incision is made in the groin region. The surgeon is then able to push the protruding tissue back into place and strengthen the weakening muscle wall by inserting synthetic mesh. This conventional method may be conducted under local, regional, or general anesthesia.
The most commonly used open technique is the Lichtenstein tension-free mesh repair, which is associated with low recurrence rates. Patients who are unable to withstand general anesthesia or who experience hernias following several laparoscopic surgeries or those with large inguinoscrotal hernias are also likely to be offered open surgery.
Laparoscopic (Minimally Invasive) Repair
Laparoscopic surgery involves the use of multiple small incisions as opposed to a single large cut. The surgeon uses special tools and a small camera called a laparoscope. Laparoscopy has two major techniques:
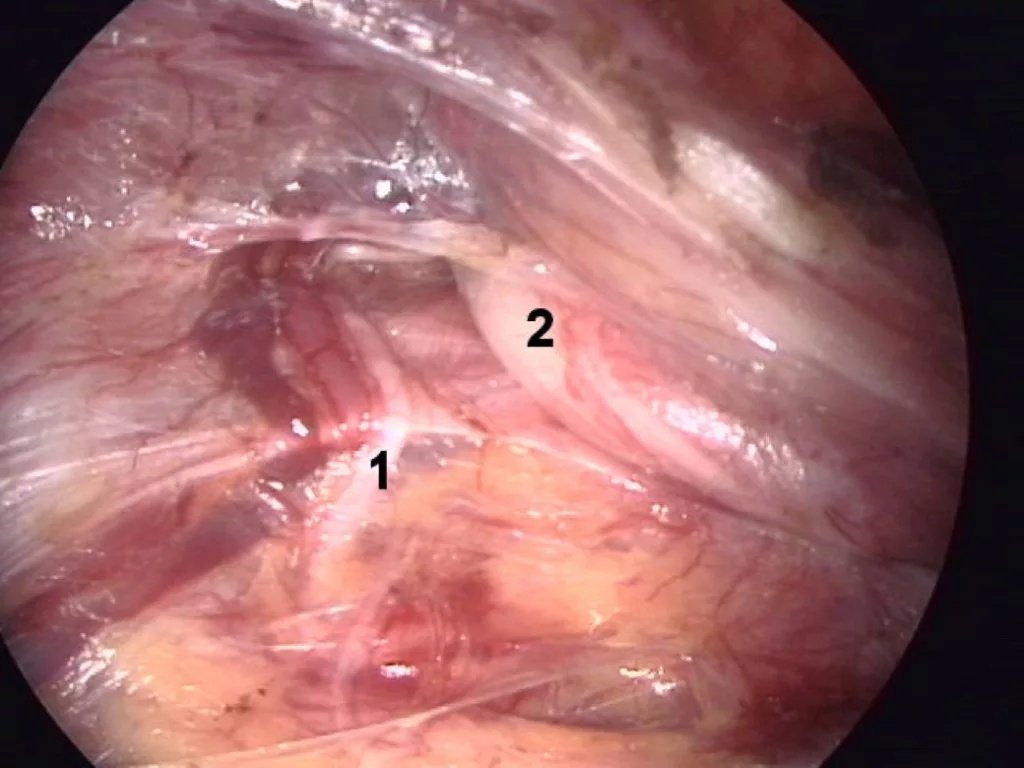
Intraoperative view during total extraperitoneal (TEP) inguinal hernia repair showing (1) the genital ramus of the genitofemoral nerve and (2) preperitoneal lipoma with the spermatic cord.Credit: Anpol42,CC BY-SA 3.0, Wikimedia Commons
- Totally Extraperitoneal (TEP) Repair: The procedure is performed entirely in the preperitoneal space without entering the abdominal cavity.
- Transabdominal Preperitoneal or TAPP: The surgeon enters the peritoneal cavity, places mesh in the preperitoneal space, and then closes the peritoneal flap.
Laparoscopic repair will usually lead to reduced postoperative pain, shorter scars, quicker recovery, and a lower risk of chronic groin pain compared with open repair. It is especially useful in patients with bilateral hernias, hernias recurring after open repair, or groin hernias.
Robotic Hernia Repair
The latest method of hernia repair is robotic surgery. It employs the robotic tools that are controlled by the surgeon with improved accuracy and 3-D imaging. Although robotic surgery has the same advantages as laparoscopic repair, it is generally more costly. Recent research demonstrates similar results to conventional laparoscopic procedures, and some surgeons report improved dexterity in complex cases, but clear superiority over laparoscopy has not been definitively established.
Double Inguinal Hernia Surgery
In case hernias are formed on both sides of the groin at the same time, they are known as bilateral or double inguinal hernia. These are in the range of 8 to 30 percent of all inguinal hernias. Interestingly, when a patient has a hernia on one side, it has a 25% probability of having an occult hernia on the other side.
The two hernias may be normally fixed together in one operation. In the case of a double inguinal hernia, laparoscopic surgery is a preferred method of surgery since the surgeon can operate on both sides with the same small incisions and therefore inflict less trauma and recovery time. Bilateral hernia repair during a single operation is equivalent to unilateral repair and less expensive than performing two separate surgeries.
Inguinal Hernia Surgery Recovery Time
The number of days to get back to normal after the operation depends on the type of surgery, the health of the patient in general, and whether the hernia was unilateral or bilateral.
Recovery Timeline
The following is an approximate recovery time of an inguinal hernia surgery:
| Time Period | What to Expect |
|---|---|
| First 24-48 Hours | Fatigue and dizziness from anesthesia. Pain in the incision site of a mild-moderate intensity. Begin gentle walking at home. Most patients go home the same day. |
| Week 1 | Light daily activities and short walks are recommended. Return to desk work may be possible for some patients, particularly after laparoscopic repair, but strenuous activity should be avoided. |
| Weeks 2-3 | Gradual increase in daily activity. Driving is permitted if the patient is not taking narcotic pain medication. Light exercise, such as walking or stationary cycling may be resumed if comfortable. |
| Weeks 4-6 | Most patients may return to physically demanding work and begin light resistance training, depending on the surgeon’s advice and surgical approach. |
| 2-3 Months | Full recovery for most patients. Go back to all normal exercises, such as running and jumping. |
| 6 Months | Residualdiscomfort or swelling may persist in some patients, but full functional recovery is expected. |
Important note. Laparoscopic surgery normally enables quicker recovery than open surgery. Minimally invasive techniques have the tendency to release patients back to normal activities approximately 8 days earlier.
Pain Following Inguinal Hernia Surgery
A certain level of post-surgery inguinal hernia pain is quite normal. With an idea of what is to be expected, patients would be able to differentiate between normal healing pain and possible complications.
Acute Postoperative Pain
Patients have different degrees of discomfort at the incision within the first few days after surgery. The pain typically peaks at days 2-3 with the full wearing out of local anesthesia. This is normal. After laparoscopic surgery, shoulder or chest discomfort may occur due to carbon dioxide insufflation and usually resolves within 24–48 hours.
Pain management involves a combination of opioids immediately after surgery, followed by short-term use of acetaminophen or NSAIDs. Ice packs used in intervals of 10-20 minutes within the first 3 days may greatly help to alleviate swelling and discomfort.
Chronic Pain After Hernia Surgery
Although the majority of patients recover without a long-term problem, chronic pain occurs in about 10-16 percent of hernia surgery patients. Pain lasting longer than 6 months after the operation is considered chronic post-herniorrhaphy pain (also called inguinodynia). The causes of chronic pain include:
- Nerve injury, entrapment, or compression during surgery.
- Nerves are trapped between the sutures or torn by fixation devices, such as tacks.
- Mesh-related problems include the shrinkage of the mesh and the trapping of nerves.
- Permanent inflammation of the mesh.
The patients report about the chronic pain as burning, stabbing, sharp, or electric. In men, it may spread to the testicle. Management begins with conservative treatments such as medications and nerve blocks. Surgical intervention is reserved for carefully selected cases, and success rates vary, rather than being universally curative.
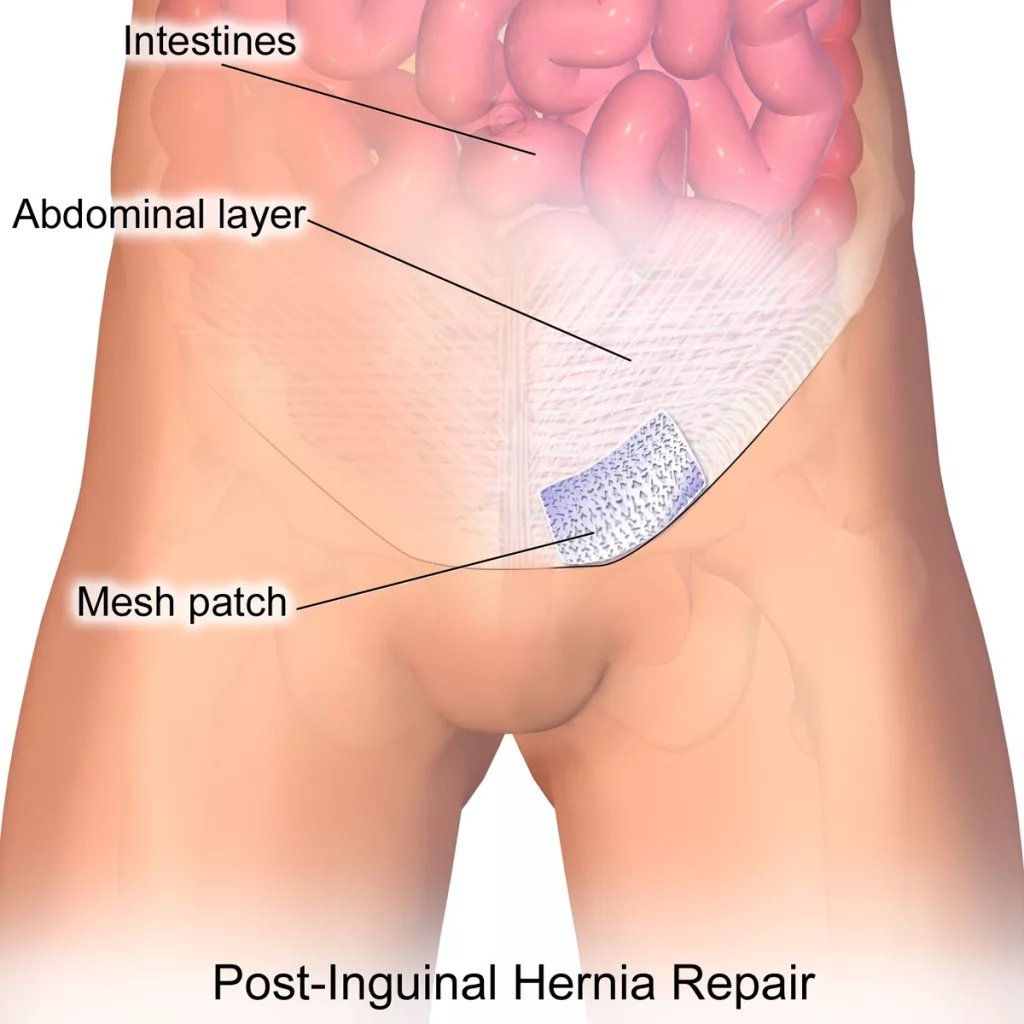
Illustration showing an inguinal hernia patch used to reinforce the abdominal wall during hernia repair.Credit: BruceBlaus,CC BY-SA 4.0, Wikimedia Commons (File: Inguinal Hernia Patch.png)
Studies indicate that laparoscopic repairs are always associated with low rates of chronic pain as compared to open repairs; this is a major factor to be considered during the selection of a surgical method.
Exercise After Inguinal Hernia Surgery
Exercise is a key component of recovery, although it depends on the time and intensity. Exercising too soon after inguinal hernia surgery may cause complications such as hernia recurrence, whereas excessive inactivity may slow the process of healing and may predispose an individual to blood clotting.
Safe Exercise Progression
Immediately post-surgery (Day 1-3), frequent 5-10 minute walks are better to enhance circulation, avoid blood clots, and facilitate digestion. Walking also aids in pushing gas in the intestines and lessening the bloating.
Week 1: Progressively increase the time and the distance of walking. There is an opportunity to walk outside at your own speed. You can do light stretching.
During Weeks 2-4: Low-impact activities may be introduced if pain-free, while heavy lifting and core-intensive exercises should be avoided.
Weeks 4-6: Revert to moderate-intensity training such as brisk walking, and taking of elliptical machine, and cycling. Minimal weight resistance training of light intensity. Golf and other low-impact sports.
2-3 Months: Progressively resume pre-surgery condition. Begin with small weights and go on increasing. Heavy resistance training and high-impact sports should generally be delayed until at least 6–8 weeks postoperatively, depending on surgeon guidance.
Exercises to Avoid in Recovery
For the next 4-6 weeks, step out of activities involving too much strain on the abdominal wall:
- Heavyweight lift (less than 10-15 pounds during the first 4 weeks)
- The sit-ups, crunches, and other core-intensive exercises
- Deadlifts, squats, and heavy compound
- Push-ups and pull-ups
- Any twisting, jerking, or sudden movements
To keep in mind: The pain is the indicator of the body that you are doing too much. When an activity is painful, then get off to rest and allow time to recover.
Do’s and Don’ts Following an Inguinal Hernia Surgery
Adherence to the following guidelines facilitates the best recovery and eliminates the chances of complications:
DO:
- Walk regularly to improve circulation and prevent blood clots.
- Make the incision clean and dry; take care of the shower in 24-48 hours.
- A diet high in fruits, vegetables, and whole grains is rich in fiber.
- Consume as much water as possible to be hydrated and avoid constipation.
- Use painkillers in accordance with the doctor’s prescriptions.
- Use ice packs at 10-20 intervals within the first 3 days.
- Wear soft clothes so that they do not press on the incision.
- Keep a pillow and use it against your incision during coughing and sneezing.
- Visit all of your follow-up appointments with your surgeon.
- Perform deep breathing exercises to avoid pneumonia.
DON’T:
- Weight lifting not more than 10-15 pounds during the first 2-4 weeks.
- Perform the intense activity or extreme exercise for at least 4-6 weeks.
- Keep absolutely still; move about a little and a good deal all day long.
- First 5-7 days, take baths or go swimming (showers are all right).
- Drive when on narcotic pain drugs.
- Smoke, since it leads to impairment of healing and an augmentation of risk.
- Strain during bowel movements.
- Disregard symptoms of complications such as fever, intense pain, and infection.
Risks and Complications of Inguinal Hernia Surgery
Although inguinal hernia surgery is usually a safe and effective procedure, knowledge of its possible complications would enable you to recognize warning signs and consult a doctor in case of an emergency.
Common Short-Term Complications
Such complications normally arise during the first few weeks of surgery:
- Infection in the incision site: The symptoms include redness, warmth, pain that is getting worse, along with swelling and drainage. Occurs in less than 1% of cases.
- Seroma: Skin fluid accumulation. The condition can resolve itself, but in some cases, drainage is necessary.
- Hematoma: Accumulation of blood at the operation site. Presents itself in the form of bruising and usually heals with time.
- Urinary retention: This occurs when one can not pass urine after surgery, especially in males. Normally acute and fades away in hours.
- Constipation: The usual one associated with anesthesia and analgesics. Avoided by using a high-fiber diet and hydration.
Long-Term Complications
- Hernia recurrence: The hernia can return after repair. Recurrence is different depending on the technique, but is usually between 1-10%. Smoking, chronic cough, obesity, and heavy lifting immediately after surgery are risk factors.
- Chronic groin pain: As described above in detail, it occurs in 10-16% of patients. May cause a great effect on the quality of life.
- Mesh-related complications: These are mesh migration, mesh erosion, or mesh infection. These dangers have been greatly minimized by the use of modern meshes.
- Testicular complications: Testicular atrophy, chronic pain, or, in some rare cases, infertility may result in men due to damage to blood vessels or nerves.
- Sexual dysfunction: The experience of pain during sex may also happen, but it is not common with the correct surgical procedure.
When to Seek Immediate Medical Attention?
Contact your surgeon immediately or go to the emergency room if you experience:
- Fever above 101°F (38.3°C)
- Severe or worsening abdominal pain
- Nausea and vomiting, which will not allow you to retain fluids
- Bright red blood bleeding bandages
- Incision that grows progressively red, swollen, or pus-draining
- Shortness of breath or chest pain
- Leg swelling
- Inability to urinate
Conclusion
Inguinal hernia repair is a relatively safe and routine operation that substantially enhances the quality of life of those who suffer it. Modern surgical procedures, such as open, laparoscopic, and robotic ones, allow surgeons to address the individual needs and situation of the patients.
The process to recover after the surgery of inguinal hernia will take time and follow-up. The majority of the patients resume normal functions in 2-3 months, and laparoscopic surgeries frequently enable a quicker patient recovery. The knowledge of what to expect at each stage of the healing process, possible complications, and post-surgery do’s and don’ts will be helpful in guaranteeing the best possible outcomes in case of inguinal hernia surgery.
Although there are some risk factors associated with surgery regarding inguinal hernias, the advantages of hernia repair are much higher than the possible risks to most patients. Even untreated hernias may have serious outcomes, including imprisonment and strangulation, so surgical treatment is necessary in the case of symptomatic hernias. You have the best opportunity of repairing and resuming regular functioning through working with an experienced surgeon and taking his or her particular suggestions into consideration.
References
[1] Burcharth J, Pedersen M, Bisgaard T, Pedersen C, Rosenberg J. Nationwide prevalence of groin hernia repair.PLoS One. 2013;8(1):e54367. doi:10.1371/journal.pone.0054367
[2] Abramson JH, Gofin J, Hopp C, Makler A, Epstein LM. The epidemiology of inguinal hernia. A survey in western Jerusalem.J Epidemiol Community Health. 1978;32(1):59-67. doi:10.1136/jech.32.1.59
[3] Lichtenstein IL, Shulman AG, Amid PK, Montllor MM. The tension-free hernioplasty. Am J Surg. 1989;157(2):188-193. doi:10.1016/0002-9610(89)90526-6
[4] Andresen K, Burcharth J, Fonnes S, et al. Transabdominal preperitoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair.Cochrane Database Syst Rev. 2024;7(7):CD004703.
[5] Qabbani A, Aboumarzouk OM, ElBakry T, Al-Ansari A, Elakkad MS. Robotic inguinal hernia repair: systematic review and meta-analysis.ANZ J Surg. 2021;91(11):2277-2287. doi:10.1111/ans.16505
[6] Amid PK, Shulman AG, Lichtenstein IL. Simultaneous repair of bilateral inguinal hernias under local anesthesia.Ann Surg. 1996;223(3):249-252. doi:10.1097/00000658-199603000-00003
[7] Simons MP, Smietanski M, Bonjer HJ, et al. International guidelines for groin hernia management.Hernia. 2018;22(1):1-165. doi:10.1007/s10029-017-1668-x
[8] Aasvang E, Kehlet H. Chronic postoperative pain: the case of inguinal herniorrhaphy.Br J Anaesth. 2005;95(1):69-76. doi:10.1093/bja/aei019
[9] Reinpold W, Nehls J, Eggert A. Risk factors of chronic pain after inguinal hernia repair: a systematic review.Innov Surg Sci. 2017;2(2):61-68. doi:10.1515/iss-2017-0017
[10] Simons MP, Smietanski M, Bonjer HJ, et al. World guidelines for groin hernia management.Hernia. 2018;22(1):1-165. doi:10.1007/s10029-017-1668-x
[11] Tolver MA, Strandfelt P, Forman JL, et al. Determinants of a short convalescence after laparoscopic transabdominal preperitoneal inguinal hernia repair.Surgery. 2012;151(4):556-563. doi:10.1016/j.surg.2011.09.041
[12] Celdran-Uriarte A, Mariscal-Flores S. Surgical site infection after elective inguinal hernia repair: a cohort study.Hernia. 2013;17(2):181-186. doi:10.1007/s10029-012-0981-7
[13] Fitzgibbons RJ Jr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial.JAMA. 2006;295(3):285-292. doi:10.1001/jama.295.3.285
[14] Klosterhalfen B, Junge K, Klinge U. The lightweight and large porous mesh concept for hernia repair.Expert Rev Med Devices. 2005;2(1):103-117. doi:10.1586/17434440.2.1.103
For more information about Inguinal hernia surgery, refer to the latest medical literature.