
{kind=link}

Psoriasis Eczema differences Psoriasis and Eczema (also called Atopic Dermatitis) are very similar in appearance to an untrained eye. However, to medical professionals, there are critical differences between the two. While their symptoms overlap, their underlying pathophysiology, and thus, the long-term management strategies are very different.
Both conditions are chronic and involve the immune system, but in different ways. Psoriasis is the result of an autoimmune overactivity in cell turnover, while eczema results from a damaged skin barrier. Approximately 3% of the global population lives with psoriasis, while eczema is significantly more common, up to 10-20% in children and 3-10% in adults.
This difference in underlying cause means that the cost of misdiagnosis is quite high. If the thin, cracked skin of an eczema flare is treated with psoriasis topicals, the skin can actually atrophy. Similarly, if psoriasis isn’t diagnosed and treated, it can develop into psoriatic arthritis.
Pathophysiology of Psoriasis vs Eczema: Psoriasis Eczema differences
The primary difference between psoriasis and eczema lies at the cellular level:
Psoriasis is an immune-mediated inflammatory disease driven by T-cell dysregulation. The immune system mistakenly attacks healthy skin cells, forcing them to mature in 3 to 5 days instead of the standard 28-day cycle. These cells cannot shed fast enough, leading to the characteristic buildup of dead tissue.
Eczema is often a structural defect involving the filaggrin protein. The skin lacks the ceramides that hold the cells together. This creates a leaky barrier that loses moisture, a process we call transepidermal water loss. This makes the skin vulnerable to allergens and irritants, and these trigger inflammation.
[Image: Clinical photo of atopic dermatitis on the palms and soles, showing red, scaly skin with deep, painful cracks and fissures.]
(a) Palmar and (b) Plantar Eczema. Diffuse erythema, dryness, and painful fissuring. Unlike the well-defined “punched-out” plaques of psoriasis, AD on the hands and feet typically presents with ill-defined borders and a higher frequency of vesiculation (blistering) during acute flares. (Image Courtesy: Kapur, S., Watson, W. & Carr, S. Atopic dermatitis. Allergy Asthma Clin Immunol 14 (Suppl 2), 52 (2018). Available fromSpringerand licensed under CC by 4.0)
Genetic and Environmental Triggers
Neither of these conditions is caused by infections. Though their mechanisms are different, both are rooted in the “Two-Hit” hypothesis of genetics and environment. What this means is that a genetic predisposition to develop either condition is present in a person, and the actual manifestation is brought about when there is exposure to an environmental trigger.
- Psoriasis Triggers: Stress, skin injuries (Koebner phenomenon), medications (like Beta-blockers or Lithium), and streptococcal throat infections.
- Eczema Triggers: Harsh soaps, detergents, animal dander, cold and dry weather, and some food allergens.
Clinical Diagnostic Markers for Psoriasis and Eczema
| Feature | Psoriasis | Eczema (Atopic Dermatitis) |
|---|---|---|
| Primary Sensation | Itching (pruritus), often astinging or burningfeeling | Intense, ‘mad’itchingthat doesn’t let you sleep |
| Appearance | Thick, well-defined,silvery scales onred bases | Poorly defined, red, scaly patches that mayooze |
| Common Sites | Extensor surfaces(Elbows, knees, scalp, and lower back) | Flexor surfaces (Inner elbows, behind knees, neck, and face) |
| Onset | Typically starts in early adulthood (ages 15 to 35) | Often begins in infancy or early childhood |
| Clinical Signs | Auspitz Sign: Pinpoint bleeding when scales are removed | Lichenification (skin thickening) due to constant scratching4Guttman-Yassky, E., Katoh, N., J Cork, M., Jagdeo, J., F Alexis, A., Chen, Z., A Levit, N., & B Rossi, A. (2025). Dupilumab Treatment Improves Lichenification in Atopic Dermatitis in Different Age and Racial Groups. Journal of drugs in dermatology : JDD, 24(2), 167–173. |

Classic Psoriasis Vulgaris (Plaque Psoriasis): Well-circumscribed, erythematous plaques and characteristic silvery scales on the extensor surfaces of the limbs and trunk. These thick, dry lesions are the primary diagnostic indicators for plaque-type disease. (Image Courtesy: Rendon, A., & Schäkel, K. (2019). Psoriasis Pathogenesis and Treatment. International Journal of Molecular Sciences, 20(6), 1475. Available fromMDPIand licensed under CC by 4.0)
Is Psoriasis Contagious?
It’s true that many skin conditions are contagious, but that’s not all of them. This is actually one of the most persistent and damaging myths in dermatology. And as if the visible nature of these conditions isn’t isolating enough, the mental toll this myth takes on a person makes it even more of a social stigma.
In case of both psoriasis and eczema, no, they aren’t contagious. Psoriasis is an internal autoimmune process; it cannot be spread through touch, clothing, or swimming pools. The same is true for eczema. There is zero risk of transmission to others.
Clinical Management and Treatment
Because these are chronic conditions, we don’t speak of a cure, but rather a clearance. For the inflammation part, the baseline management is pretty much the same. Systemic management is where the protocols differ.
First-Line Anti-Inflammatory Care:
These form the baseline for both conditions, focusing on reducing surface-level inflammation and maintaining the skin’s structural integrity, before we can move on to the underlying cause.
Daily Skincare:
When you live with a chronic skin condition, your daily routine is your first line of defense. The goal is to repair the skin barrier and minimize triggers.
In this case, the most efficient is the ‘soak and seal’ method: It involves applying a thick, fragrance-free emollient within three minutes of taking a lukewarm (never hot) bath or shower. This traps the water in the skin before it evaporates.

The ‘Soak and Seal’ protocol for barrier maintenance. This process arrests Transepidermal Water Loss (TEWL) and provides an artificial barrier against external irritants.
Topical Treatments:
- Topical Corticosteroids are the first-line for both. They suppress localized immune responses.
- Steroid-sparing agents like Calcineurin Inhibitors (Tacrolimus) are best for sensitive areas like the face or skin folds, where steroids might thin the skin in both eczema and psoriasis patients.
Phototherapy (NB-UVB):
Phototherapy uses specific light wavelengths to slow cell turnover and suppress overactive T-cells. Under medical supervision, exposing the skin to specific wavelengths of ultraviolet (UV) light can be a miracle for patients with widespread flares of either condition.
Psoriasis Specific Treatment:
The goal of psoriasis treatment is to slow down the rapid cell turnover and reduce the thickness of the scaling. If you don’t remove the scale, the medicine can’t reach the target.
- Keratolytics (Salicylic Acid): These lift and dissolve the thick silvery scales so other topicals can penetrate the skin.
- Vitamin D Analogues (Calcipotriene): These slow down the rapid production of skin cells.
- Biologics: For moderate-to-severe cases, we use protein-based drugs that are IL-17 and IL-23 inhibitors. These block the specific cytokines responsible for both the skin plaques and underlying joint destruction (arthritis), without suppressing the entire immune system. With these precision drugs, we are now seeing an incredible 90% skin clearance in over 75% of patients, a rate that was unheard of 15 years ago.
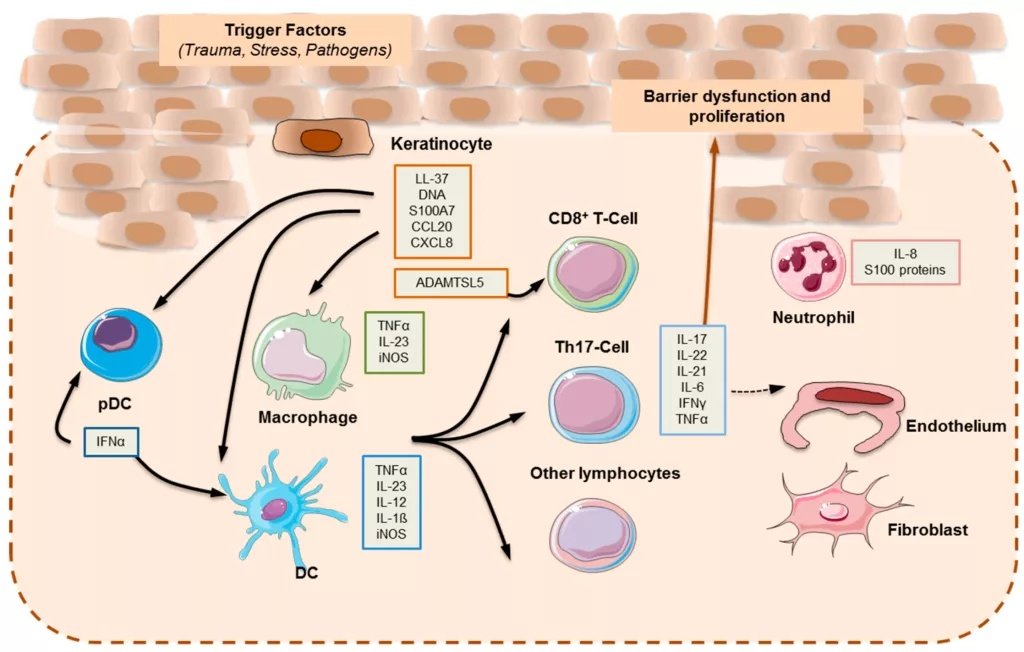
Pathogenetic Targets of Modern Biologics. This cytokine cascade (IL-23/Th17 axis) drives keratinocyte hyperproliferation. Biologic therapies, specifically IL-17 and IL-23 inhibitors, function by neutralizing these exact molecular checkpoints to break the inflammatory cycle. (Image Courtesy: Rendon, A., & Schäkel, K. (2019). Psoriasis Pathogenesis and Treatment. International Journal of Molecular Sciences, 20(6), 1475. Available fromMDPIand licensed under CC by 4.0)
Eczema Treatment:
Eczema management targets the leaky barrier and the mad itch-scratch cycle.
- Barrier Repair Creams: While moisturizers help both, eczema specifically requires ‘physiologic lipids’ (ceramides, cholesterol, fatty acids) to repair the defective skin barrier.
- Wet Wrap Therapy: Applying topicals followed by damp bandages provides immediate rehydration for acute flares; it provides a physical barrier against nighttime scratching.
- Antihistamines: They don’t stop the underlying cause, but provide the sedation necessary for patients to sleep through the intense itch.
- Biologics: IL-4 and IL-13 inhibitors (Dupilumab) provide systemic relief for moderate-to-severe Atopic Dermatitis by suppressing the inflammatory response.
Can Psoriasis and Eczema Be Treated Through Diet?
Of course, there is no miracle diet that can cure an autoimmune condition, but nutrition does play a significant role in systemic inflammation. There are two basics to understand here:
- Diets high in refined sugars and processed foods can increase C-Reactive Protein (a marker of inflammation) in the blood, which can exacerbate a skin flare-up.
- On the other hand, a Mediterranean-style diet rich in Omega-3 fatty acids (salmon, walnuts, flaxseeds) acts as a natural internal lubricant for the skin and helps dampen the body’s inflammatory response.
Complications of Eczema & Psoriasis
Both these dermatological conditions are systemic indicators that should signal the situation can get much worse if not caught in time.
30% of patients develop Psoriatic Arthritis. If a patient presents with skin plaques and morning joint stiffness, immediate intervention is required to prevent permanent joint destruction.
Similarly, in the case of Eczema, it is often the first stage of the atopic cycle that can be followed by asthma and allergic rhinitis.
When to Consult a Specialist?
Eczema and psoriasis cannot be self-managed even otherwise, but certain symptoms require immediate clinical intervention to prevent complications:
- If the skin becomes weepy, develops a golden-yellow crust, or feels abnormally hot and swollen, it signals a secondary infection.
- If your skin rashes are accompanied by stiff, swollen joints (especially in the morning), you may be developing Psoriatic Arthritis.
- If over-the-counter medications fail after 14 days, you need prescription-strength intervention.
Final Word
Skin is a mirror of the body’s internal health. If the skin is showing inflammation, the cause is most likely systemic. And systemic inflammation, especially one caused by autoimmune responses, requires timely clinical intervention. Whether it’s the stinging plaques of psoriasis or the intense itch of eczema, early clinical intervention is the only way to prevent permanent skin thickening and to find a regimen that restores the skin.
References
[1] Bronckers, I. M., Paller, A. S., van Geel, M. J., van de Kerkhof, P. C., & Seyger, M. M. (2015). Psoriasis in Children and Adolescents: Diagnosis, Management and Comorbidities. Paediatric drugs, 17(5), 373–384.
[2] Chovatiya, R., & Silverberg, J. I. (2019). Pathophysiology of Atopic Dermatitis and Psoriasis: Implications for Management in Children. Children (Basel, Switzerland), 6(10), 108.
[3] Gupta, J., & Margolis, D. J. (2020). Filaggrin gene mutations with special reference to atopic dermatitis. Current treatment options in allergy, 7(3), 403–413.
[4] Guttman-Yassky, E., Katoh, N., J Cork, M., Jagdeo, J., F Alexis, A., Chen, Z., A Levit, N., & B Rossi, A. (2025). Dupilumab Treatment Improves Lichenification in Atopic Dermatitis in Different Age and Racial Groups. Journal of drugs in dermatology : JDD, 24(2), 167–173.
[5] Malecic, N., & Young, H. (2016). Tacrolimus for the management of psoriasis: clinical utility and place in therapy. Psoriasis (Auckland, N.Z.), 6, 153–163.
[6] Campa, M., Mansouri, B., Warren, R., & Menter, A. (2016). A Review of Biologic Therapies Targeting IL-23 and IL-17 for Use in Moderate-to-Severe Plaque Psoriasis. Dermatology and therapy, 6(1), 1–12.
[7] Lopes, A. E. D. S. C., Araújo, L. F., Levy, R. B., Barreto, S. M., & Giatti, L. (2019). Association between consumption of ultra-processed foods and serum C-reactive protein levels: cross-sectional results from the ELSA-Brasil study. Sao Paulo medical journal = Revista paulista de medicina, 137(2), 169–176.
[8] Ocampo D, V., & Gladman, D. (2019). Psoriatic arthritis. F1000Research, 8, F1000 Faculty Rev-1665.