
{kind=link}

What is Chylothorax?: Chylothorax Comprehensive Medical
Chylothorax Comprehensive Medical Chylothorax is the accumulation of lymphatic fluid, called Chyle, in the pleural space. Chyle is usually a milky or opalescent fluid rich in triglycerides, chylomicrons, and white blood cells. However, the appearance may vary and can sometimes be serous or blood-stained, especially in fasting patients. Normally, chyle travels through the body’s largest lymphatic vessel, the thoracic duct, before emptying into the bloodstream. When the system is disrupted, chyle can leak into the chest cavity, causing severe respiratory stress and malnutrition.[1]
The condition affects both children and adults. In fact, chylothorax is the most common type of pleural effusion in newborns. It is therefore important to learn more about this complicated lymphatic disorder to be able to detect it early and treat it.
Understanding the Lymphatic System & Thoracic Duct
In the body, the thoracic duct serves as the primary highway of lymphatic vessels. It drains about 70% of the body’s lymph, including most dietary fats absorbed from the intestines. This duct begins at the cisterna chyli in the abdomen, ascends through the thoracic cavity behind the esophagus, and ends at the junction of the left internal jugular and subclavian veins.
The thoracic duct is prone to surgical trauma or injury because it is anatomically intricate. Therefore, most cases of chylothorax are a result of iatrogenic causes.
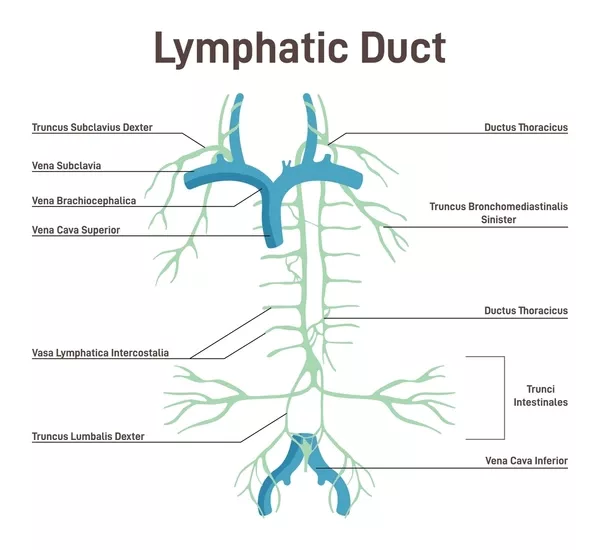
Lymphatic system.
Chylothorax Causes: From Surgical Trauma to Congenital Conditions
Primary Causes of Chylothorax:
Iatrogenic (Surgery-Related) – Most Common2 Agrawal A, Chaddha U, Kaul V, et al. Multidisciplinary Management of Chylothorax. Chest. 2022.
- Post-esophagectomy complications
- Complications of cardiovascular surgery
- Surgery of the neck and the chest.
- Development of lymphatic fistulas during an operation.
Traumatic Causes (20% of Cases)
- Chest or back injuries
- Spinal fracture-dislocations
- Blunt trauma to the thorax
- Birth trauma in neonates
Neoplastic Causes
- Lymphoma (which is the most common among malignant causes)
- Chronic lymphocytic leukemia
- Lung cancer
- Esophageal cancer
- Kaposi sarcoma
Congenital & Developmental3 Sendama W. Traumatic chylothorax: A case report and review. Respiration / Case Reports. 2015.
- Pulmonary lymphangiectasia
- RASopathies (including Noonan syndrome)
- Central conducting lymphatic anomalies
- Lymphangiomatosis
- Gorham-Stout disease
Other Medical Conditions
- Thrombosis of the Subclavian Vein
- Tuberculosis and other infections
- Sarcoidosis
- Mediastinal lymphadenopathy
- Chylous ascites
Chylothorax Symptoms: Recognizing the Warning Signs
Primary Symptoms:
The hallmark symptom of chylothorax is progressive shortness of breath (dyspnea) as accumulated chyle compresses the lungs. Patients typically experience:[2]
- Respiratory distress – difficulty breathing, especially with exertion
- Coughing- usually a dry cough
- Pressure or tightness in the chest
- Fatigue and weakness – due to compromised breathing and nutritional losses
Secondary Symptoms:
With the progression of the condition, other problems can arise:
- Weight loss and malnutrition (due to protein and fat loss)
- Deficiency of fat-soluble vitamins (A, D, E, K)
- Loss of white blood cells in the pleural fluid (Lymphopenia)
- Hypovolemia due to massive loss of fluid.
Distinguishing Features:
Unlike other pleural effusions, patients with chylothorax usually do not experience:
- Do not develop fever (chyle is non-irritating)
- Sharp pleuritic chest pain
- Develop symptoms gradually, usually within several days after injury or surgery
Chylothorax Diagnosis: Advanced Imaging & Laboratory Tests
Clinical suspicion is usually the initial step in the diagnosis, which is based on symptoms and risk factors. Upon suspicion, it is established by physical examination, radiography, and laboratory tests.[3]
Physical Examination Findings:
- On auscultation, there are decreased breath sounds on the affected side
- Dullness to percussion over the area of effusion
- Reduced chest wall movement
- Frequently, respiratory distress (tachypnea, use of accessory muscles) is evidence.
- No fever (differentiating from infectious diseases)
Chest Imaging:
- Chest X-ray showing pleural effusion
- CT chest or ultrasound to assess the extent and cause
- MRI or lymphangiography for complex or bilateral cases

James Heilman, MD – Bilateral chylothorax seen on a thoracic MRI, licensed under Creative Commons Attribution- 4.0 International (CC BY-SA 4.0).
Definitive Laboratory Diagnosis:
Thoracentesis & Pleural Fluid Analysis
The gold standard for chylothorax diagnosis involves comprehensive pleural fluid analysis:[4]
The pleural fluid analysis shows:
- Milky or opalescent fluid appearance
- Triglyceride levels >110 mg/dL strongly suggest chylothorax
- Triglycerides <50 mg/dL make it unlikely; values between 50–110 mg/dL require testing for chylomicrons
- Presence of chylomicrons confirms the diagnosis
- Lymphocyte predominance (>80%)
- Protein levels >3.0 g/dL (exudative pattern)
- LDH usually normal or low despite high protein
- Absence of malignant cells helps rule out neoplastic causes
Advanced Lymphatic Imaging
Dynamic Contrast MR Lymphangiography (DCMRL) is a recent method of identifying the location of the lymphatic leakage, classifying the leakage pattern, and directing the interventions.[5] This technique uses three injection approaches:[6]
- Intranodal injection (inguinal lymph nodes)
- Intrahepatic (liver)
- Intramesenteric (mesentery)
Pyothorax vs Chylothorax: Key Differences
| Feature | Chylothorax | Pyothorax |
|---|---|---|
| Fluid Appearance | Milky white, opalescent | Purulent, cloudy, foul-smelling |
| Composition | Chyle (triglycerides, chylomicrons) | Infected pleural fluid with bacteria |
| pH | Usually normal | Acidic (<7.30) |
| Glucose | Normal to elevated | Low (<60 mg/dL) |
| Symptoms | Gradual dyspnea, no fever | Fever, chest pain, systemic illness |
| Treatment | Dietary/surgical intervention | Antibiotics and drainage |
| Urgency | Progressive but not immediately life-threatening | Medical emergency requiring immediate drainage |
Chylothorax Treatment: From Conservative to Surgical Approaches
Treatment strategies for chylothorax follow a stepwise approach based on the underlying cause, severity, and patient response.
Conservative Management (First-Line Treatment):
Conservative management may be effective in a good number of patients, particularly in traumatic chylothorax, where it is successful in about half of patients. Nevertheless, it is not as effective in cases that are not trauma-related. Initial therapy includes reducing chyle flow and improving nutrition.[7]
Dietary Interventions
- Medium-chain fatty acid diet: These are not stored as the regular fats but are directly transported into your bloodstream by the portal circulation, by-passing the lymphatic system.[8]
- Total parenteral nutrition (TPN): Indicated when chyle output exceeds 1–1.5 L/day in adults or when oral intake fails to reduce drainage.[9]
- Fat-soluble vitamin supplementation: Prevents nutritional deficiencies
Pharmacological Support
- Octreotide: It decreases the flow of the lymphatics and the amount of chyle.[10]
- Somatostatin is a similar drug to octreotide.
- Diuretics: They may help reduce overall effusion volume, but are not curative.
Symptomatic Relief
Doctors can relieve the situation immediately by:
- Thoracentesis: It is a procedure using a needle to extract the fluid.
- Chest tube drainage: Short-term solution for large or rapidly accumulating effusions.
- Continuous monitoring for electrolyte, protein, and fluid losses.

Thoracentesis. Thoracocentesis is an invasive medical procedure to remove fluid or air from the pleural space for diagnostic or therapeutic purposes.
Surgical Treatment Option:
Surgery is not the initial option, but it should be considered when the conservative treatment is not working.
Video-Assisted Thoracoscopic Surgery (VATS)
VATS has become a favorite type of surgery in most cases due to being the least invasive surgery.[11]
Thoracic Duct Ligation
The surgeon makes three small incisions to reach the chest and tie the thoracic duct. Success rates are impressive, ranging between 85-95% of traumatic causes, and the majority of patients are discharged within a 3-5 day period.[12] Usually performed through VATS or open thoracotomy, depending on the site of the leak.
Percutaneous Thoracic Duct Embolization
In recent years, percutaneous thoracic interventions have become valuable alternatives to open thoracic surgery. These image-guided procedures involve inserting fine needles or catheters through the chest wall to directly access lymphatic structures or the thoracic duct.
They are especially useful for patients who are poor candidates for major surgery or when the exact site of chyle leakage has been localized through dynamic contrast MR lymphangiography (DCMRL).
Common percutaneous procedures include:
- Percutaneous thoracic duct embolization (TDE): A catheter is advanced into the lymphatic system (often via the groin), and the leaking duct is sealed using coils, glue, or embolic agents. This has become the treatment of choice in many specialized centers due to its high success rate and low complication risk.
- Percutaneous thoracic duct disruption: Used when embolization is not feasible, this involves targeted needle puncture of the thoracic duct to reduce lymphatic flow.
- Percutaneous drainage: Guided by ultrasound or CT, it helps relieve fluid pressure in recurrent effusions.
Compared to open thoracotomy, these procedures are less invasive, require shorter hospitalization, and have lower postoperative morbidity. However, they require specialized expertise and imaging facilities, and may not be suitable if the duct anatomy is severely distorted or the leak site cannot be accessed.
Pleurodesis Procedures
Pleurodesis is the procedure that forms adhesions between the lung and the chest wall to avoid the accumulation of fluid. It is used when surgical correction is not feasible. It has two major approaches:
- In Chemical Pleurodesis, Talc (4-6g), doxycycline (500mg), or, sometimes, bleomycin are all used in chemical pleurodesis to form these adhesions.[13]
- Mechanical Pleurodesis may be done intraoperatively. Recurrence prevention is effective in more than 90 percent of cases, yet it permanently wards off the pleural space.
Open Surgical Approaches
In some cases, the conventional open surgeries are required, such as thoracotomy, especially when VATS hasn’t worked or the chest adhesions are widespread.
Supraclavicular Approach
In cases of injuries that are high on the thoracic duct, the surgeons could reach it by an incision that is above the collar bone, where the duct joins the great veins. In this technique, attention has to be taken with respect to significant blood vessels and nerves.
Diet for Chylothorax: Nutritional Management Strategies
Diet is not merely supportive therapy in chylothorax, but is, in fact, a first-line therapy that can have a lot of influence.[14]
Phase 1: Acute Management (Days 1-14):
When TPN is Needed?
TPN is usually prescribed by physicians when:
- In adults, the daily output of chylus is more than 1.5 liters.
- Patient is ill and completely malnourished (albumin less than 2.5g/dL).
- Eating normally is not possible.
- After 5-7 days, a trial of the MCT diet has failed.
TPN Composition & Management
- Calories: 25-30 kcal/kg/day (adjust for metabolic stress)
- Protein: 1.2-1.5g/kg/day (higher if ongoing losses)
- Carbohydrates: 50-60% of total calories
- Lipids:
- Micronutrients: Standard multivitamin with emphasis on fat-soluble vitamins
Medium-Chain Triglyceride (MCT) Diet
The MCT diet takes centre stage when patients can eat:[15]
- Daily intake of total fats should not be more than 10-15g of regular (long-chain) fats.
- Use MCT oil for 60–80% of fat calories.
- This usually will last 2-4 weeks, based on its working capability.
Foods to Eat
- Lean proteins (chicken breast, fish, egg whites)
- Complex carbohydrates (rice, oats, potatoes)
- Fruits and vegetables (low-fat varieties)
- MCT-based products and supplements
Foods to Avoid
- High-fat dairy products
- Nuts and seeds
- Fried foods
- Fatty meats
- Oils and butter (except MCT oil)
- Avocado and olives
Phase 2: Transition and Recovery (Weeks 3–6):
You can begin to add normal fats when:
- There is a reduction in the output of chyle below 500ml per day for at least 48 hours.
- The fluid is growing less milky.
- Breathing is stable.
- Nutritional indicators are good.
Gradual Fat Reintroduction Protocol
This occurs in steps:
3rd Week:
Increase the amount of regular fats to 15-20g daily and still take MCT oil. Light quantities of olive oil and natural fish are fine.
4th Week:
Increase to 25-30g as the beginning to decrease MCT oil. You can put in small amounts of nuts, salmon, and restricted dairy fat.
5-6 Weeks:
Start to resume normal fat consumption (50-70g/day) with careful attention paid to the production of chyle.
Specialized Nutritional Considerations:
Managing Vitamin Needs
- Vitamin A: The usual dosage is 5,000-10,000 IU every day with monthly blood tests. After normalizing your diet, vegetables that are good natural sources of beta-carotene are obtained.[16]
- Vitamin D: Typically, 1,000 to 2,000 IU/day, more so in case of deficiency. The levels are to be checked every two months, particularly when one is not exposed to sunlight much.[17]
- Vitamin E: Besides, 400-800 IU of vitamin E is prescribed, and the level of tocopherol in serum is to be monitored. Gradually, natural sources like nuts and oils can be reintroduced.
- Lastly, vitamin K gains special significance when the intake of fats is limited for longer than two weeks, with 100-500 mcg per day as recommended. INR test and bleeding monitoring are also important, particularly in patients who have already been put on anticoagulation treatment.[18]
Essential Fatty Acid Management
The treatment of chylothorax requires strict fat intake with close attention to the essential fatty acids. The lack of omega-3s may appear in several weeks, and it may be necessary to undergo EPA/DHA supplementation under the supervision of a physician.
In the case of omega-6 deficiency, the body requires a small but critical amount of linoleic acid, which is supplied by modest vegetable oils when the diet is liberalized. Clinicians need to watch out for signs of deficiency, such as skin changes. This nutritional treatment is not only supportive but rather a first-line treatment option, which has a direct impact on the treatment.
Chylothorax Prognosis: Outcomes & Long-Term Outlook
Chylothorax prognosis depends on its cause.
The prognosis of traumatic and post-surgical patients is generally very good and usually heals within weeks, with a cure rate of almost 100 percent under proper intervention. On the same note, the results are very satisfactory in cases of pediatric patients and cases of percutaneous embolization, where the success rates are high and recovery is anticipated.
In contrast, a malignancy-related chylothorax presents a more challenging prognosis.Recurrent or chronic cases can be treated with several procedures and dietary control, and the quality of life can be maintained in most cases.[19]
Conclusion
Chylothorax is a disease of the lymphatic system, which should be properly analyzed, diagnosed, and treated. The shift from primary surgical treatment toward complex, non-surgical operations over the years has led to the enhancement of complex conditions.
In addition, the treatment outcomes have been better by using the advanced imaging technologies for diagnosis, such as Dynamic Contrast MR Lymphangiography and selective lymphatic embolization. It should, however, focus on the right pathophysiology, the correct conservative treatment, and definitive interventional or surgical treatment.
Lastly, ongoing cooperation between multidisciplinary care teams and expert lymphatic centers has become a revolution, and it provides hope to even the most difficult cases of this rare but treatable disease.
References
[1] Bhatnagar M, et al.Chylothorax: pathophysiology, diagnosis, and management. J Thorac Dis. 2024.
[2] Agrawal A, Chaddha U, Kaul V, et al.Multidisciplinary Management of Chylothorax. Chest. 2022.
[3] Sendama W.Traumatic chylothorax: A case report and review. Respiration / Case Reports. 2015.
[4] Porcel JM, et al.Clinical characteristics of chylothorax: results from the European Respiratory Journal. ERJ. 2023.
[5] Rehman KU, Sivakumar P.Non-traumatic chylothorax: diagnostic and therapeutic strategies. Breathe (Sheffield). 2022.
[6] Litvin R, et al.Nontraumatic Chylothorax: A Case Series From a Safety-Net Hospital. Ann Intern Med. 2023.
[7] Kiang SC, et al.Direct contrast-enhanced magnetic resonance lymphangiography to detect occult chylous leaks. J Vasc Venous Access. 2019.
[8] Lee CW, et al.Postoperative Chylothorax: the Use of Dynamic Enhanced MR Lymphangiography. I-MRI. 2018.
[9] Agrawal A, Chaddha U, Kaul V, et al.Multidisciplinary Management of Chylothorax. Chest. 2022.
[10] Nair SK, Petko M, Hayward MP. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg. 2007;32(2):362-369.
[11] Zabeck H, Muley T, Dienemann H, Hoffmann H. Management of chylothorax in adults: when is surgery indicated? Thorac Cardiovasc Surg. 2011;59(4):243-246.
[12] Rimensberger PC, Müller-Schenker B, Kalangos A, Beghetti M. Treatment of a persistent postoperative chylothorax with somatostatin. Ann Thorac Surg. 1998;66(1):253-254.
[13] Rehman KU, Sivakumar P.Non-traumatic chylothorax: diagnostic and therapeutic strategies. Breathe. 2022.
[14] Mohan R, Joshi M, Garg R, Ketan T. Traumatic chylothorax: management by thoracic duct ligation. J Clin Diagn Res. 2013;7(6):1162-1164.
[15] Light RW. Pleural Diseases. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2013.
[16] Bhatnagar M, et al.Chylothorax: pathophysiology, diagnosis, and management. J Thorac Dis. 2024.
[17] Valentine VG, Raffin TA. The management of chylothorax. Chest. 1992;102(2):586-591.
[18] Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington, DC: National Academy Press; 2001.
[19] Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-281.
[20] uttie JW. Vitamin K in Health and Disease. Boca Raton: CRC Press; 2009.
[21] Riley LE.Clinical approach and review of causes of a chylothorax. Respir Med. 2019.