
 is surgically repositioned...){kind=link}

Maxillary Osteotomy Improving Maxillary osteotomy is a type of orthognathic surgery in which the maxilla (upper jaw) is surgically repositioned to correct skeletal and dental misalignments. It is done for functional or aesthetic purposes. The procedure is commonly used to correct congenital or developmental deformities, traumatic injuries, or acquired conditions involving maxillary retrusion, protrusion, open bite, or asymmetry. Among the different techniques, the Le Fort I osteotomy is the most frequently performed approach for repositioning the maxilla.
Maxillary Osteotomy Indications: Maxillary Osteotomy Improving
There are multiple issues for which your dentist might advise you to undergo an upper jaw osteotomy. The common indications for this procedure include:
Bite Derangement:
Thousands of children and adolescents across the globe suffer from a deranged bite. Malocclusion can be attributed to dental or underlying skeletal abnormalities. Patients with skeletal anomalies need surgical interventions. Surgeons frequently perform bimaxillary osteotomy to correct skeletal anterior open bite. Modern studies demonstrate that the surgical procedure exhibits great stability in open bite cases. However, the best results are achieved when osteotomy surgery is paired with orthodontic correction. Other bite deformities that can be corrected with osteotomies include deep bites, crossbites, and underbites.
Maxillary Bone Growth Abnormalities:
Osteotomy surgeries can fix abnormal growth patterns of the maxilla. Vertical maxillary excess (VME) is a condition in which overgrowth of the maxilla bone occurs in the vertical dimension. It presents with unesthetic features, such as a long face and excessive gum display (gummy smile). Doctors frequently adopt the conventional Le Fort 1 osteotomy to correct this anatomical deformity. It also helps correct a gummy smile in patients.
However, there is a compromised upper movement of the bone. Therefore, nowadays, doctors opt for altered versions of the Le Fort 1. One such alteration, i.e., the horseshoe osteotomy, has proven to provide substantial upward movement of the maxilla in patients with long face syndrome.
Orthognathic surgery is the treatment of choice for moderate-to-severe maxillary deficiencies. Doctors pair orthodontic treatment with orthodontic treatment for superior skeletal corrections.
Occlusal Assymmetries (Horizontal Discrepancies):
In addition to vertical abnormalities, a maxillary osteotomy is also indicated for horizontal discrepancies between the maxilla and the mandible. Angle’s classification best denotes the relationship between the upper and lower jaws (occluding teeth).

The illustration shows different types of horizontal and vertical malocclusions, which can be corrected with orthognathic surgeries like maxillary osteotomy.
Class 2 Malocclusion
Class 2 represents a distoclusion where the mandible is retrusive in relation to the maxilla, which can be due to a retrusive mandible, a protusive maxilla, or a combination of both. Thus, a maxillary osteotomy can help set back the bone to improve aesthetics and function.
Class 3 Malocclusion
In class III, the mandible is protrusive, the maxilla retrusive, or a combination of both. A maxillary osteotomy can help advance the retruded upper jaw, often in combination with mandibular surgery. Surgeons have observed that osteotomies in severe class II and class III cases not only improve facial aesthetics but also enhance nasal function.
When one jaw grows out of proportion, other structures in the oral cavity follow the pattern. Therefore, in several cases, surgeons perform both mandibular and maxillary osteotomies together. In rare cases of associated macroglossia, a glossectomy may also be performed to optimize results. Studies show that the combination of Le Fort I maxillary osteotomy, mandibular sagittal split ramus osteotomy (SSRO), and glossectomy leads to significant improvements in masticatory abilities.
Professionals compared the impact of orthodontic vs surgical treatment (maxillary osteotomy) for class 3 malocclusion cases and found that the occlusal outcome for both procedures (surgical and orthodontic) is great and comparable. However, a smaller number of appointments is needed for surgical corrections.
Thus, a maxillary osteotomy is the treatment of choice in severe occlusal discrepancies involving misalignments of the upper jaw.
Midface Hypoplasia
An aesthetic indication for maxillary osteotomy is midface hypoplasia. It is a craniofacial syndrome characterized by a severe growth deficiency in the mid-face region. For moderate cases, a maxillary osteotomy can suffice. However, for severe cases (maxillary discrepancies averaging more than 15 mm), doctors combine Le Fort osteotomy (distraction surgery) with other procedures, such as mandibular osteotomy.
Sleep Apnea
Health professionals are now adopting orthognathic surgery as a treatment option for certain functional issues like obstructive sleep apnea. Modern clinicians believe that abnormal growth patterns of the dentofacial structures (nose, palate, tonsils, tongue, and jaws, etc.) contribute directly to sleep apnea. A 2024 study concluded that maxillary surgery is safe and has high efficacy in improving symptoms of obstructive sleep apnea. However, the maxillary osteotomy procedure should be performed after palatal surgery.
Studies suggest that maxillomandibular advancement has the highest success rate for obstructive sleep apnea. Sometimes, patients undergo an osteotomy to correct severe difficulties in chewing, speaking, and swallowing arising from an abnormal maxilla.
Skull Base Tumors
Gaining access to the base of the skull is a difficult surgical task. Thus, sometimes, surgeons opt for a maxillary osteotomy to access the skull base. Access osteotomy is a successful procedure in the field of oral and maxillofacial surgery. Surgeons frequently adopt procedures like Le Fort 1 osteotomy, transfacial maxillary swing, and lip-split mandibulotomy to access inaccessible tumors of the craniomaxillary region.
Maxillary Osteotomy Types
Osteotomies of the upper jaw are broadly divided into two types:
Segmental Maxillary Osteotomy:
As the name indicates, surgeons cut only a portion (segment) of the maxilla to achieve the aesthetic or functional changes required.
Anterior Segmental Oosteotomy
This mainly involves correcting the front (anterior) region of the maxilla to fix apertognathia (open bite in the front teeth). Moreover, forward advancement of the maxilla also falls under this sub-category.
Posterior Segmental Osteotomy
The surgeon accesses the posterior segment (molars region) mainly to fix open bites and issues in this area.
Combination of Anterior & Posterior Osteotomies
A horseshoe osteotomy is a combination of both anterior and posterior types. In comparison to conventional Le Fort 1 osteotomy, this type yields superior nasal esthetics after maxillary repositioning. Horseshoe osteotomy helps surgeons fix complex dentofacial deformities.
U-shaped Osteotomy
This is a variation of the horseshoe osteotomy that involves giving a U-shaped cut in the palate. The main aim of this technique is to minimize the chances of damage to the descending palatine artery (DPA), which potentially occurs during the posterior repositioning of the maxilla. It allows better mobilization and repositioning of the maxilla.
Total Maxillary Osteotomy:
These types of osteotomies allow complete movement and repositioning of the maxilla. It is further divided into:
Le Fort 1 Osteotomy
It is the most common type of maxillary osteotomy. It accurately addresses issues of protrusion and maxillary asymmetry, thereby greatly improving aesthetics. In this technique, the surgeon makes a horizontal incision below the nose and continues to cut across the maxilla. So, doctors can advance or set back the maxilla, depending on the requirements.
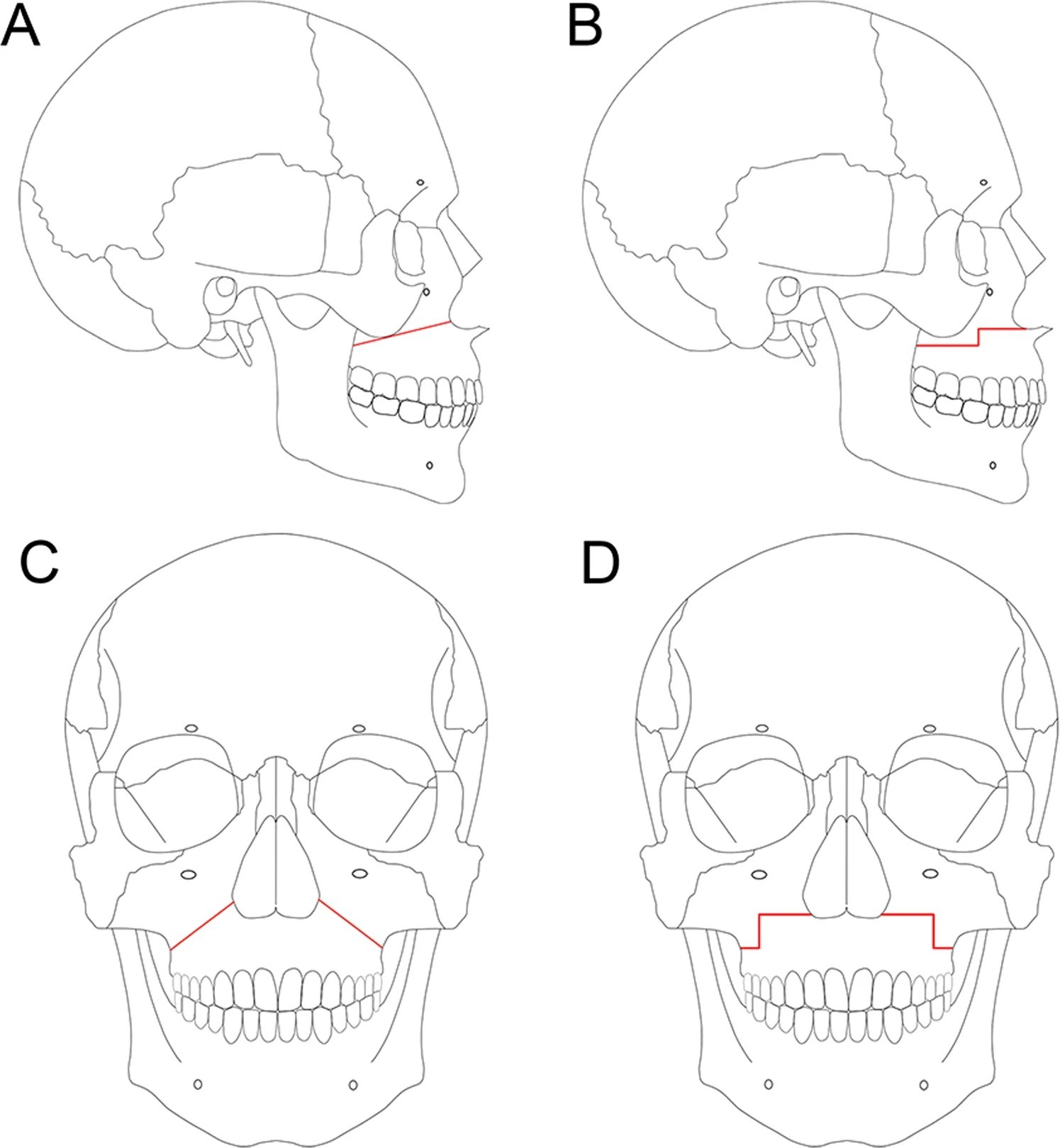
The illustration shows the Le Fort 1 osteotomy variations for different cases. By Kazuto Kurohara, Nobuyoshi Tomomatsu, Koichi Nakakuki, Naoya Arai, and Tetsuya Yoda –https://www.nature.com/articles/s41598-019-46233-5/figures/1,CC BY 4.0,Link
Le Fort 2 Osteotomy
Lesser common than type 1, this type involves a pyramidal cut that spans through the maxilla and the midface bones (including nasal bones, medial orbital walls, inferior orbital rims, orbital floor, and zygomaticomaxillary sutures). It is primarily done to correct midface hypoplasia.
Le Fort 3 Osteotomy
The most extensive type, detaching and mobilizing the entire midface as a single unit. It includes cuts through the nasal bones, zygomas, and orbital rims. Indicated for severe craniofacial syndromes (e.g., Crouzon or Apert syndrome).
Maxillomandibular osteotomies (MMO)
In a number of cases, doctors surgically alter both jaws (upper and lower) to treat discrepancies. Maxillomandibular advancement surgeries have proven to be effective in alleviating symptoms of obstructive sleep apnea.
Maxillary Osteotomy Procedure
As maxillary osteotomy falls under the category of orthognathic surgery, presurgical orthodontics is carried out in most cases. However, in several cases, orthodontists perform post-surgical orthodontic treatments to do the final root alignment and root parallelism.
Most surgeons perform a model surgery called a mock surgery before actually cutting the bone of a patient. Doctors create replica models of the patient’s jaws and then stimulate surgical movements on the model to accurately prepare for the surgery. This provides pre-operative practice to the surgeon and also helps communicate well (for demonstration) with the patients. Doctors also fabricate a splint on the new position of the reoriented maxilla. This splint helps guide the surgeon in repositioning the bone during the actual surgery. The procedure takes 1.5 to 3 hours on average to complete.
Anesthesia:
Surgeons perform a maxillary osteotomy under general anesthesia. An anesthesiologist accompanies the team of oral surgeons to administer general anesthesia.
Incision & Access:
To ensure maintenance of patient aesthetics, all the incisions are made inside the mouth. This prevents incision lines and scarring on the facial skin. After anesthesia, a surgeon makes an incision in the gum just above your upper teeth to surgically expose the maxilla.
Surgeons use a variety of specialized surgical instruments, including scalpels (for incisions), retractors (to hold soft tissues), osteotomes, rongeurs, bone files, and surgical saws to cut and reshape bone. Depending on the case, the surgeon may perform either a segmental osteotomy or a total osteotomy (e.g., Le Fort I osteotomy).
Bone Cutting and Repositioning
The surgeon cuts the bone following the pre-planned osteotomy pattern. After mobilizing the bone, the maxilla is repositioned into the new, corrected alignment.
Fixation:
To stabilize the repositioned maxilla, surgeons most commonly use titanium mini-plates and screws. These provide rigid fixation and allow for early function and healing. Once stability is confirmed, the incision site is closed with resorbable sutures, eliminating the need for suture removal.
Maxillary Osteotomy Recovery
Bone healing is generally a slow process that takes months to complete. The recovery time typically ranges between 6 and 12 weeks. However, complete healing of the bone may even take up to 6 months, depending on the patient’s overall health.
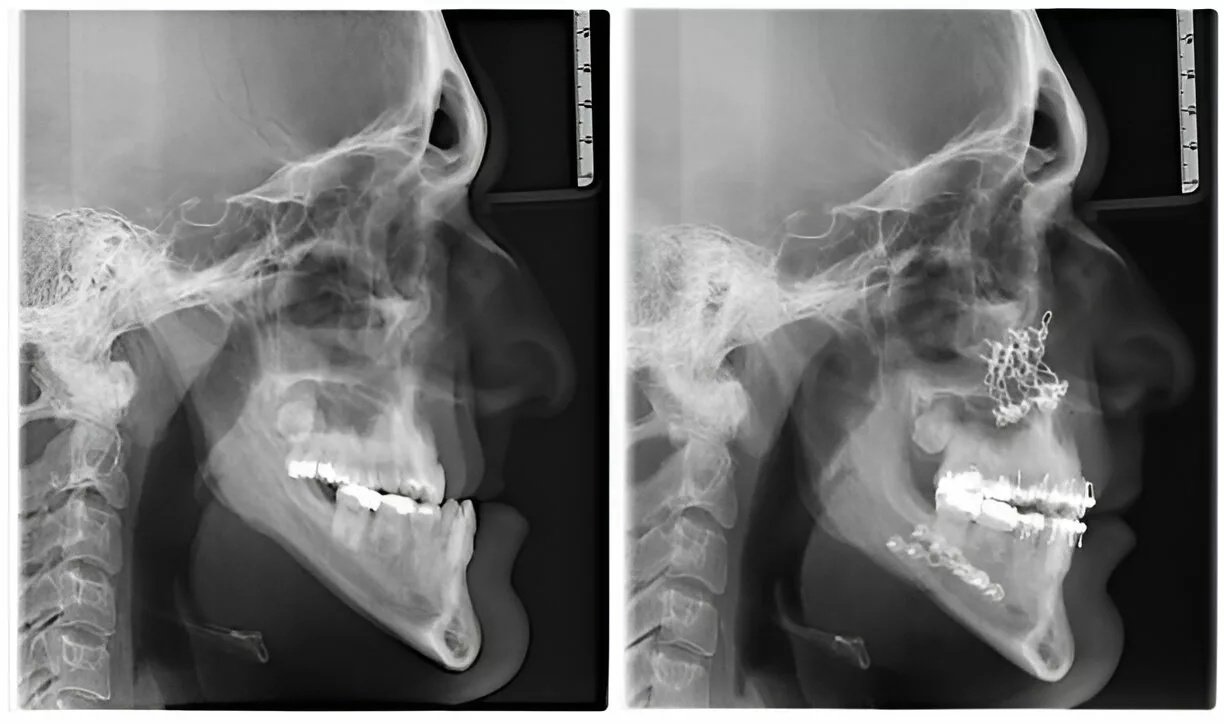
The X-ray shows pre- and post-op of a patient after combined mandibular and maxillary osteotomies.
During the first several days (or even weeks), you might feel some bruising, discomfort, and swelling. Most of the swelling goes away by the end of the first month, and by this time, patients can start noticing the changes in the appearance. The pain usually lasts for a few days.
Maxillary Osteotomy Post-Operative Care:
You can follow these steps for a quick healing:
- Apply ice to the surgical site during the first 24-48 hours after surgery to reduce post-operative swelling.
- Take over-the-counter analgesics to manage pain (which may last for several days).
- Shift to a softer diet for the initial couple of weeks to reduce strain on the jaws.
- Minimize strenuous activities for about 3 months to ensure proper, flawless fixation of the bone in the new position.
- Strictly follow your doctor’s advice and regularly take prescribed antibiotics to minimize the chances of infection.
Maxillary Osteotomy Complications
The surgical repositioning of the upper jaw involves manipulation of numerous hard and soft tissue structures. This increases the chances of post-operative complications. Although meticulous planning and careful execution minimize the chances of serious complications, there still can be some.
Mild Complications:
Issues like pain and swelling can be managed with medication and mostly resolve without intervention. However, excessive bleeding from the site indicates an underlying hemorrhage that needs immediate medical attention.
Infection after surgery is common and can be managed well with antibiotics (prophylactic management is better than treatment). Other potential complications of maxillary osteotomy include injury to the soft tissues (gums, cheeks, etc.) and hard tissues (teeth). An oroantral communication arises when there is a breach in the oral/nasal cavity linings, i.e, oral mucosa and the maxillary sinus membrane, that leads to a communication between the two cavities.
While nerve injuries are more common in mandibular osteotomies, researchers have identified that maxillary osteotomy-induced cranial nerve injuries can lead to nerve palsies. There have been cases of injury to these nerves following a bimaxillary osteotomy:
- Ⅱ (optic): Provides vision
- Ⅲ (oculomotor): Controls eye movement
- Ⅳ (trochlear): Controls eye movement
- Ⅴ (trigeminal): Provides sensations to the face and motor control for chewing
- Ⅵ (abducens): Controls eye movement
Neurosensory complications are attributed to unfavorable bone fractures during an osteotomy. Most of the time, the nerve impingement or injury is temporary and heals after some time.
Serious Complications:
Though rare, serious complications from upper jaw osteotomy include. The extent and patient’s propensity to develop complications depend upon the skill of the surgeon, the type of osteotomy performed, and the overall health of the patient.
- Permanent nerve injury (and palsy)
- Improper/incomplete bone joining (malunion or even nonunion of bone) due to unfavorable fractures
- Relapse of the jawbone to the original position
- Long-term inflammation of the maxillary sinus (sinusitis) due to debris lodgement during the surgery
- Osteonecrosis (death of bone tissues)
Wrapping Up
Maxillary osteotomy is an orthognathic surgery to correct anatomical abnormalities (vertical, horizontal) of the maxilla that cause functional and aesthetic issues. The surgical intervention is indicated in cases of vertical maxillary excess, open bite (apertognathia), malocclusion (class 2 and 3), and midface hypoplasia. An osteotomy is also done to correct obstructive sleep apnea and to access skull base tumors. Surgeons may opt for a segmental or a total maxillary osteotomy (Le Fort 1,2, or 3) along with orthodontic treatment for complete correction.
A maxillary osteotomy is performed under general anesthesia with in-mouth incisions to prevent facial skin scarring. A surgical splint guides the surgeon while he fixes the jaw in a new position using screws and metal plates. Temporary post-operative complications of a maxillary osteotomy include pain, bruising, bleeding, and nerve impingement (or damage), which can lead to palsies of cranial nerves. However, serious complications include permanent nerve damage and improper union of bones (malunion or non-union).
References
[1] Inchingolo, A. M., Patano, A., Piras, F., Ruvo, E. D., Ferrante, L., Noia, A. D., … & Dipalma, G. (2023). Orthognathic surgery and relapse: a systematic review.Bioengineering,10(9), 1071.
[2] Lone, I. M., Midlej, K., Zohud, O., Paddenberg, E., & Krohn, S. (2024). Global Map of Skeletal and Dental Malocclusion Prevalence: From Classes to Continents.J Dentistry Oral Disorders,10, 1183.
[3] Ellabban, I., Germain, S., Jenkins, G., & Paterson, A. (2023). The stability of anterior open bite closure after bimaxillary osteotomy.Journal of Maxillofacial and Oral Surgery,22(4), 893-899.
[4] Nasrun, N. E., Takeda, S., Minamida, Y., Hiraki, D., Horie, N., Nagayasu, H., & Shimo, T. (2021). Surgical procedures for correcting vertical maxillary excess: a review.International journal of surgery case reports,86, 106354.
[5] Goguet, Q., Mercier, J., Longis, J., Bonnet, R., Perrin, J. P., Corre, P., & Bertin, H. (2023). Long-term vertical stability of horseshoe osteotomy for the correction of large vertical excess of the maxilla, a retrospective assessment in 15 patients.Journal of Stomatology, Oral and Maxillofacial Surgery,124(5), 101474.
[6] Yang, J., Tang, Z., Shan, Z., & Leung, Y. Y. (2025). Maxillary Deficiency: Treatments and Applications for Adolescents.Applied Sciences,15(6), 3256.
[7] Yücel, H. C., Kozanoğlu, E., Akalin, B. E., Sütçü, A. O., Şentürk, E., & Emekli, U. (2024). The Effects of the Maxillary Movements in Angle Class 2 and 3 Malocclusion Treatment on Nose Air Flow Amount, Rate, and Resistance.Journal of Craniofacial Surgery,35(8), 2231-2235.
[8] Hotokezaka, H., Karadeniz, C., Hotokezaka, Y., Matsuo, T., & Yoshida, N. (2022). A severe skeletal Class III malocclusion treated with Le Fort I combined with sagittal split ramus osteotomy, mandibular body ostectomy and tongue reduction surgery. A case report.APOS Trends in Orthodontics,12, 221-229.
[9] Anwar, M., Benington, P. C., Gillgrass, T. J., & Ayoub, A. F. (2022). Surgery-first approach for correction of class III dentofacial deformity with Le Fort I osteotomy; is it advantageous?.British Journal of Oral and Maxillofacial Surgery,60(9), 1234-1239.
[10] Goel, P., Fahradyan, A., Wolfswinkel, E. M., Jacob, L., Yen, S. L., Urata, M. M., & Hammoudeh, J. A. (2021). Is Le Fort I distraction enough to treat severe midface hypoplasia?.Journal of Craniofacial Surgery,32(5), 1716-1720.
[11] Amadi, J. U., Plutino, F., Scozzafava, E., Delitala, F., Liberatore, G., & Brevi, B. C. (2024). Maxilla management in “phase II” skeletal surgery for obstructive sleep apnea.Journal of Cranio-Maxillofacial Surgery,52(11), 1367-1375.
[12] Walker, A., Kassir, M. F., Sama, V., Nguyen, S. A., & Abdelwahab, M. (2025). Maxillomandibular Advancement Safety and Effectiveness in Obstructive Sleep Apnea: Systematic Review and Meta‐Analysis.Otolaryngology–Head and Neck Surgery,172(4), 1142-1154.
[13] Girdhar, P., Pansotra, N., Sandhu, A. P., & Kansal, K. (2021). Access Osteotomy in the Maxillofacial Region: A Review of Literature.Baba Farid University Dental Journal,11(1), 83-90.
[14] Kitagawa, S., Habu, M., Tsurushima, H., Ohtani, T., Sakamoto, K., Yoshiga, D., … & Tominaga, K. (2023). Horseshoe osteotomy maintains the nasal cavity and function after superior repositioning.Journal of Cranio-Maxillofacial Surgery,51(12), 746-754.
[15] Shiokawa, H., Mochizuki, K., Hama, S., Miyahara, Y., Sakamoto, M., Kaneko, N., … & Moriyama, M. (2025). U-Shaped Osseous Release for Le Fort 1 Osteotomy: Potential Application to Superior Repositioning.Journal of Craniofacial Surgery,36(4), 1114-1118.
[16] Trindade, P. A. K., Nogueira, V. D. S. N., & Weber, S. A. T. (2023). Is maxillomandibular advancement an effective treatment for obstructive sleep apnea? Systematic literature review and meta-analysis.Brazilian journal of otorhinolaryngology,89, 503-510.
[17] Gaspar, C., Santos, R. B., Rodrigues, M., Zenha, H., & Costa, H. (2022). A new pattern of cranial nerve injuries caused by unfavorable fractures during Le Fort I osteotomy.Journal of Stomatology, Oral and Maxillofacial Surgery,123(4), e140-e144.