
{kind=link}

Miliary Tuberculosis TB Miliary TB is a severe form of tuberculosis characterized by a distinctive pattern of tiny, millet–seed–like lesions scattered throughout the lungs and widespread dissemination to multiple organs. The term ‘Miliary’ comes from a Latin word ‘miliarus’, meaning millet seed. The condition is caused by the bacterium Mycobacterium tuberculosis and results primarily from hematogenous (blood-borne) spread.
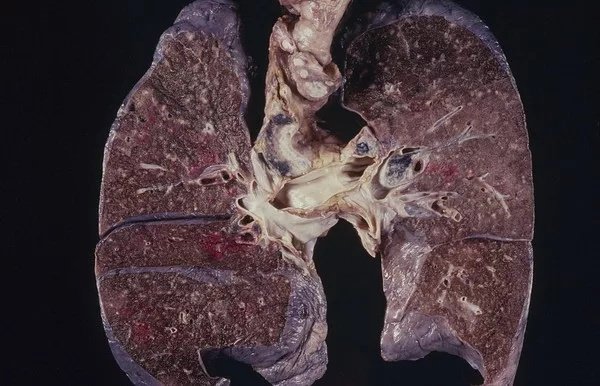
A lung CT scan showing diffusely scattered multiple tiny nodules in bilateral lung fields, suggesting miliary tuberculosis. The image is sourced fromFlickrand is under a CC BY 2.0 licence.
It is a severe form of TB that can be fatal. It ranges from non-specific symptoms to a serious medical emergency. In addition to the lungs, organs such as the liver, spleen, kidneys, bone marrow, and central nervous system may also be affected.
What Causes Miliary TB?: Miliary Tuberculosis TB
Miliary tuberculosis is a form of tuberculosis that is the result of Mycobacterium tuberculosis travelling to extrapulmonary organs, such as the liver, spleen, and kidneys. Although it is well understood that the bacteria spread from the pulmonary system to the bloodstream, the mechanism by which this occurs is not fully known yet, but there are two proposed mechanisms, which are as follows:
1. Hematogenous Spread:
One proposed mechanism is that tuberculous infection in the lungs results in erosion of the epithelial layer of alveolar cells and the spread of infection into a pulmonary vein. Once the bacteria reach the left side of the heart and enter the systemic circulation, they may multiply and infect extrapulmonary organs. Once infected, the cell-mediated immune response is activated. The infected sites become surrounded by macrophages, which form a granuloma, giving the typical appearance of miliary tuberculosis.
2. Lymphatic Spread:
Alternatively, the bacteria may invade alveolar lining cells and spread to regional lymph nodes. The organisms then drain into systemic veins and reach the right side of the heart. From there, they may seed or re-seed the lungs and other organs, producing the classical diffuse “miliary” pattern.
Risk Factors for Miliary Tuberculosis
Risk factors include close contact with TB patients, overcrowded or unsanitary living conditions, malnutrition, HIV infection, malignancy, chronic kidney disease, diabetes, and prolonged immunosuppressive therapy.
Symptoms of Miliary TB
The signs and symptoms of miliary TB range from non-specific to specific, varying from person to person. These symptoms include:
Non-specific symptoms
Patients with miliary tuberculosis often experience non-specific signs, such as coughing and enlarged lymph nodes. Miliary tuberculosis can also present with hepatomegaly (enlarged liver in 40% of cases), spleenomegaly (enlarged spleen in 5% of cases), pancreatitis(inflammation of the pancreas in <5% of cases), and multiple organ dysfunction with adrenal insufficiency (adrenal glands do not produce enough steroid hormones to regulate organ function). Stool may also be diarrheal in nature and appearance.
Specific Symptoms
The specific symptoms include fever, hypercalcemia, choroidal tubercles, cutaneous lesions, and tuberculosis meningitis (TBM), which are described as follows:
Fever
Many patients experience prolonged fever lasting several weeks, typically characterized by an evening rise in temperature rather than morning spikes.
Hypercalcemia
Hypercalcemia has been reported in a subset of patients with tuberculosis, including miliary TB. It is thought that hypercalcemia occurs as a response to increased macrophage activity in the body. The hormone, 1,25-dihydroxycholecalciferol (also referred to as calcitriol, which is the active form of vitamin D), improves the ability of macrophages to kill bacteria; however, higher levels of calcitriol lead to higher calcium levels, and thus hypercalcemia in some cases. Although recognized, hypercalcemia is an associated metabolic abnormality rather than a defining diagnostic feature.
Choroidal Tubercles
Choroidal tubercles, which are bilateral, pale, gray-white, or yellowish lesions usually less than one-quarter of the size of the optic disk and are located within 2 cm of the optic nerve, typically indicate miliary tuberculosis in children. These lesions may occur in one eye or both; the number of lesions varies between patients. Choroidal tubercles may serve as important symptoms of miliary tuberculosis, since their presence can often confirm a suspected diagnosis.
Cutaneous Lesions
Cutaneous lesions may offer a valuable clue to the diagnosis of miliary TB. Skin involvement in the form of erythematous macules and papules has also been described.
Tuberculosis Meningitis
Approximately 10–30% of adults and 20–40% of children with miliary TB develop tuberculosis meningitis (TBM) due to hematogenous spread of mycobacteria to the meninges. Symptoms often develop gradually, beginning with low-grade fever, malaise, headache, and poor appetite, and progressing to neck stiffness, vomiting, photophobia, seizures, altered mental status, focal neurological deficits, or paralysis.
How is Miliary TB Diagnosed?
Even in the endemic area, the diagnosis of miliary TB can be difficult, as the clinical symptoms are nonspecific, the chest radiographs do not always reveal the classical miliary changes, and atypical presentations are commonly encountered, but the following diagnostic approach is recommended:
Four-Point Diagnostic Criteria
The following criteria have been proposed for the diagnosis of miliary TB:
- Clinical presentation consistent with the diagnosis of TB–like pyrexia with evening rise of temperature, night sweats, anorexia, and weight loss of greater than 6 weeks in duration with response to antitubercular therapy
- Typical miliary pattern on chest radiograph
- Bilateral, diffuse reticulonodular lung lesions on a background of miliary shadows demonstrable either on chest radiograph or HRCT scan
- Microbiological or histopathological evidence of TB
Other Diagnostic Tests
Along with the above-mentioned criteria for diagnosing miliary TB, some other tests are done, which are as follows:
Laboratory and Microbiological Tests
Microbiological and histopathological examination of bone marrow, liver, peripheral lymph node, and transbronchial lung biopsy specimens have all been used to confirm the diagnosis of miliary TB, with varying results.
Hyponatremia may occur due to SIADH and may suggest associated TB meningitis. Hypercalcemia has also been described in miliary TB, but it is uncommon.
Culture and Sensitivity Tests
Culture remains the gold standard for the laboratory confirmation of TB. The culture-based diagnosis of TB is recommended in the International Standards of Tuberculosis Care.
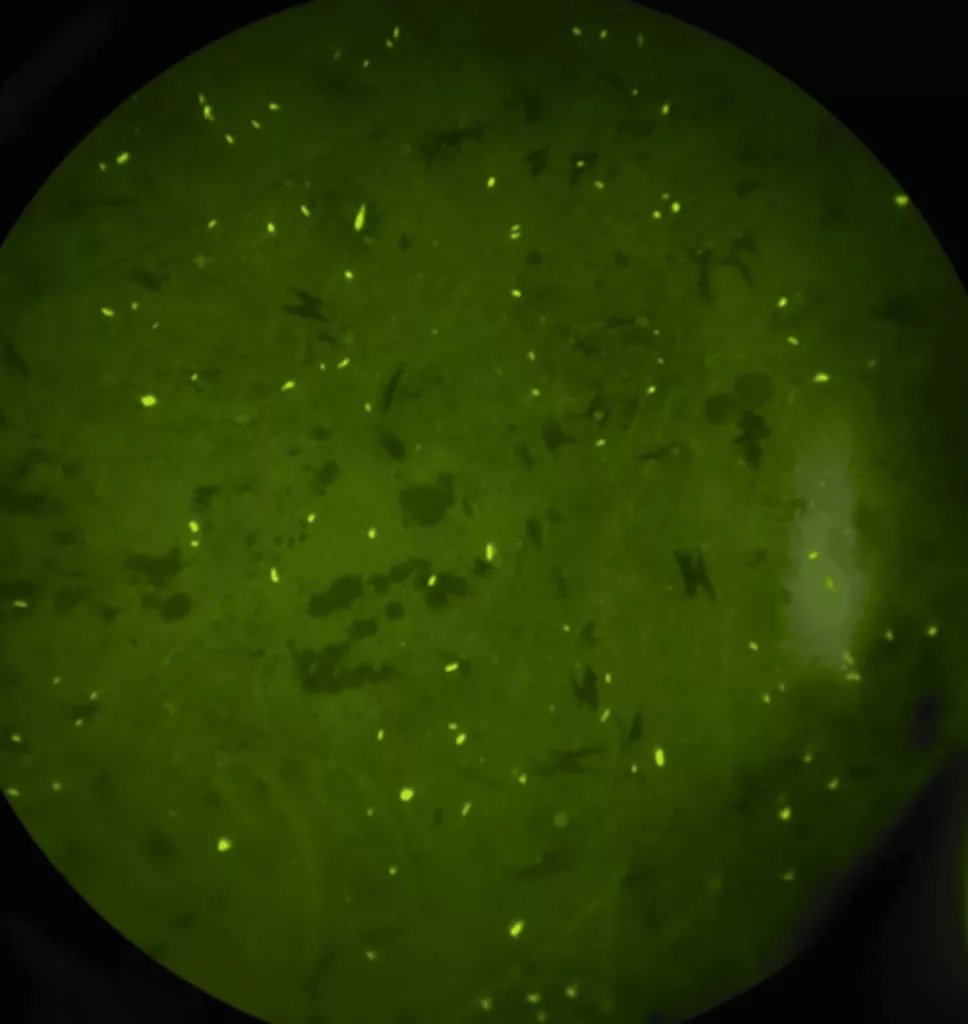
Fluorescent microscopy showing multiple acid-fast bacilli. The image is sourced fromCureusand is under CC BY License.
Tuberculin skin test
Tuberculin test positivity suggests infection, but it does not distinguish between latent TB infection and active disease. Although a positive TST signifies a possible diagnosis of miliary TB, a negative test does not exclude it.
Interferon Gamma Release Assays (IGRA)
Currently, two commercial interferon-γ release assays (IGRAs) are approved but do not differentiate latent TB infection from active TB disease and are not significantly superior to TST, albeit they have the ability to identify latent TB infection in HIV-infected individuals.
Imaging Studies
Miliary pattern on the chest radiograph is often the first clue suggestive of miliary TB. Several other imaging modalities, such as ultrasonography, CT, MRI, and positron-emission tomography (PET), help to assess the extent of organ involvement and are also useful in evaluating response to treatment.
Chest radiograph
The radiographic hallmark of miliary TB is the miliary pattern on chest radiograph of size <2mm. In about 10% of cases, the nodules may be greater than 3 mm in diameter.
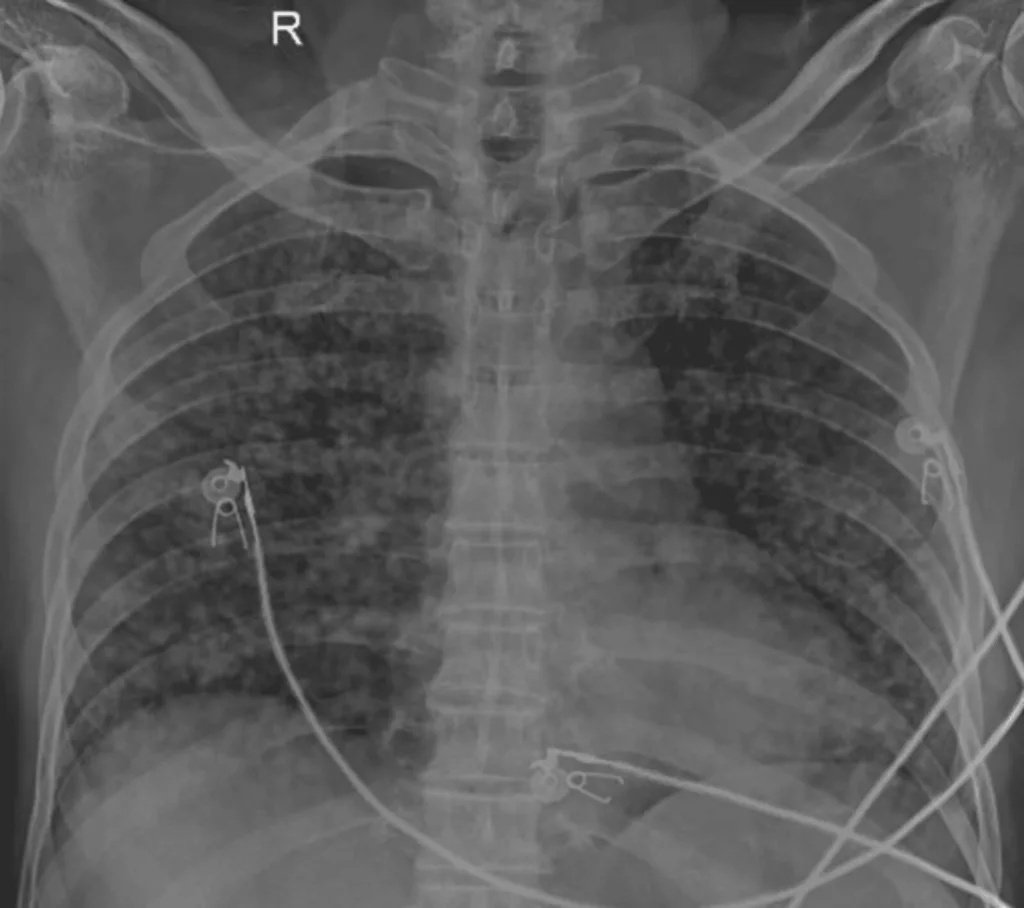
Chest radiograph showing diffusely scattered multiple tiny nodules in bilateral lung fields, suggesting miliary tuberculosis. Image credit: Mishra G V, Luharia A, Khandelwal S, et al. (September 28, 2024). Imaging of Pulmonary Miliary Tuberculosis With Multiple Intracranial Tuberculomas, sourced fromCureusunder CC BY License.
Ultrasonography
In patients with miliary TB, ultrasonography is a useful tool in detecting associated lesions, such as loculated ascites, focal hepatic and splenic lesions, intra-abdominal lymphadenopathy, and cold abscess.
Computed tomography and magnetic resonance imaging
In comparison with the pre-CT era, HRCT scans have considerably improved the antemortem diagnosis of miliary TB and may demonstrate miliary disease before it becomes radiographically apparent, e.g., Abdominal CT is useful in identifying lesions in the liver, spleen, mesentery, peritoneum, and intra-abdominal lymphadenopathy, and also detects cold abscesses.
Positron Emission Tomography
PET-CT using the radiopharmaceutical 18F-FDG has the potential to play a role in assessing the activity of various infectious lesions, including TB. The PET-CT is suitable for defining the extent of disease at the time of the evaluation of known or suspected TB cases. It can also determine the activity of lesions, guide biopsy from active sites, detect occult distant foci, and evaluate response to therapy.
Bronchoscopy
Fiberoptic bronchoscopy, bronchoalveolar lavage (BAL), bronchoscopic aspirate, brushings, washings, and transbronchial lung biopsy are useful in confirming the diagnosis of miliary TB.
Laparoscopy
When associated abdominal involvement is present, laparoscopy provides an opportunity to visualize the lesion and facilitates biopsy from the liver, peritoneum, omentum, and mesenteric lymph nodes for diagnostic confirmation.
Treatment of Miliary TB
Untreated miliary TB is almost uniformly fatal within one year. Prompt initiation of anti-tubercular therapy (ATT) is essential. . Delay in diagnosis often leads to late institution of specific treatment and significantly contributes to mortality. Current guidelines favor daily treatment regimens over intermittent therapy, especially in disseminated disease.
Guideline Recommendations
WHO Guidelines:
According to the WHO guidelines,patients are categorized as “new patients” or “previously treated patients.” Miliary TB is classified as pulmonary TB because there are lesions in the lungs. New patients with miliary TB receive six months of daily ATT for uncomplicated cases, with extended treatment (9–12 months) advised when TB meningitis or skeletal involvement is present.
CDC, ATS, IDSA, and NICE:
In the absence of associated meningeal involvement, the American Thoracic Society (ATS), the Centers for Disease Control and Prevention (CDC), the Infectious Disease Society of America, and the National Institute for Health and Clinical Excellence (NICE) TB guidelines suggest 6 months of treatment (2-month intensive phase with isoniazid, rifampicin, pyrazinamide, and ethambutol or streptomycin, followed by a 4-month continuation phase with isoniazid and rifampicin) to be adequate in miliary TB.
The NICE TB guidelines suggest that all patients with disseminated (including miliary) TB should be tested for CNS involvement by CT or MRI of the brain and/or lumbar puncture for those without CNS symptoms and signs. They recommend starting ATT even if initial liver functions are abnormal and careful monitoring during follow-up. Appropriate modification of drug treatment should be done if the patient’s liver function deteriorates significantly on ATT. Patients with miliary TB get treated under national TB control programs, with the Directly Observed Treatment, Short-course (DOTS) using short-course, intermittent, thrice-weekly treatment in low-resource countries.
AAP Guidelines
The American Academy of Pediatrics (AAP)recommends 9 months of therapy, extended to at least 12 months when TB meningitis is present.
Patients with HIV/Tuberculosis Coinfection
The WHO recommends that all patients with suspected or confirmed military TB should be tested for HIV status. In HIV-infected individuals, antiretroviral therapy should be initiated within 2–8 weeks of starting ATT, except in TB meningitis, where ART initiation is delayed to reduce the risk of IRIS.
Guideline for Children with HIV/TB Coinfection
In cases of HIV/MTB coinfected children, the CDC recommends 12 months’ ATT, including HREZ for 2 months followed by HR for 10 months ( where H= Isoniazid, R= Rifampicin, E= Ethambutol, and Z= Pyrazinamide in the drug regimen).
Guideline for Children Already Receiving ART:
For children already receiving antiretroviral treatment (ART) in whom TB is diagnosed, the ART regimen should be reviewed and optimized for treating HIV/TB coinfection and to minimize potential toxicities and drug–drug interactions. Treatment of miliary TB in patients coinfected with HIV requires careful consideration of drug–drug interactions between antituberculosis and antiretroviral drugs.
Prognosis of Miliary TB:
Miliary TB is more common in the older age group, in immunocompromised individuals, and it can be fatal if left undiagnosed, untreated, or if there is extensive organ involvement. The mortality related to miliary TB is about 15%–20% in children and 25%–30% in adults.
Miliary Tuberculosis Complications
Miliary TB, a severe form of tuberculosis, can lead to life-threatening complications in multiple organs, including the brain, heart, and abdomen. It can also cause serious systemic and immune-related disorders. Some of them are as follows:
Common Complications:
- Central Nervous System (CNS): Tuberculous Meningitis, brain abscesses, tuberculomas, seizures, paralysis (paraparesis/quadriparesis), vision loss, altered mental status.
- Cardiovascular System: Myocarditis, Pericarditis, congestive heart failure, endocarditis (native/prosthetic valves), mycotic aneurysms, pacemaker infections, sudden cardiac death.
- Respiratory System: Acute Respiratory Distress Syndrome (ARDS), pneumothorax, pneumomediastinum, empyema.
- Abdominal: Hepatic (liver) involvement (jaundice, enlarged liver/spleen), intestinal obstruction, peritonitis (ascites).
- Hematologic/Systemic: Disseminated Intravascular Coagulation (DIC), bone marrow suppression, multi-organ failure, Systemic Amyloidosis (organ deposits).
- Immune-Related: Immune Reconstitution Inflammatory Syndrome (IRIS), often in HIV patients, causing worsening symptoms.
Uncommon Clinical Manifestations and Complications in Miliary Tuberculosis:
- Cryptic miliary tuberculosis
- Pyrexia of unknown origin
- Shock
- Acute Respiratory Distress Syndrome (ARDS)
- Air leak syndrome (pneumothorax, pneumomediastinum)
- Myelopthisic anemia
- Immune hemolytic anemia
- Thyrotoxicosis
- Cholestatic jaundice
- Pericarditis with or without pericardial effusion
Miliary TB vs Pulmonary TB
What is Pulmonary TB?
Pulmonary TBis a contagious bacterial disease that commonly affects the lungs, but it can also affect other areas of the body, such as the spine, brain, or kidneys. It can be inactive, known as latent TB, or active. Pulmonary TB is the most common type of TB, and it can be differentiated from miliary TB as follows:
| Feature | Miliary Tuberculosis | Pulmonary Tuberculosis |
|---|---|---|
| Definition | Disseminated form of TB due to hematogenous spread ofMycobacterium tuberculosis | Localized TB infection primarily affecting the lungs |
| Pathogenesis | Widespread blood-borne dissemination from a primary focus | Airborne infection with local lung involvement |
| Distribution | Multisystem involvement (lungs, liver, spleen, bone marrow, meninges, etc.) | Mainly confined to lung parenchyma |
| Radiological appearance | Numerous tiny (1–2 mm) nodules uniformly distributed – “millet seed” appearance on chest X-ray | Patchy consolidation, cavitation, fibrosis, or nodular lesions |
| Common symptoms | High-grade fever, weight loss, night sweats, anorexia, generalized weakness | Hemoptysis, bronchiectasis, pneumothorax |
| Respiratory symptoms | Often mild or absent | Prominent |
| Physical findings | Hepatosplenomegaly, lymphadenopathy may be present | Crepitations, bronchial breathing, signs of lung consolidation |
| Sputum smear | Often negative | Frequently positive |
| Severity | Severe, potentially life-threatening | Variable; usually less severe than miliary TB |
| Complications | TB meningitis, adrenal insufficiency, ARDS | Hemoptysis, bronchiectasis, pneumothorax |
| Commonly seen in | Crepitations, bronchial breathing, and signs of lung consolidation | All age groups |
| Prognosis | Poor if untreated | Good with timely treatment |
Conclusion
Miliary tuberculosis is a severe and potentially life-threatening manifestation of Mycobacterium tuberculosis infection that results from widespread hematogenous (mainly) dissemination. Its varied and often nonspecific clinical presentation makes early diagnosis challenging, leading to delays in treatment and increased morbidity and mortality. A high index of suspicion, especially in vulnerable populations such as children, the elderly, and immunocompromised individuals, is essential. Timely use of appropriate imaging, microbiological investigations, and prompt initiation of anti-tubercular therapy are critical for improving outcomes. Strengthening awareness among clinicians, along with robust public health measures for tuberculosis control, remains vital in reducing the burden and fatal complications of miliary tuberculosis.
References
[1] Krishnan, Nitya; Robertson, Brian D.; Thwaites, Guy (November 2010). “The mechanisms and consequences of the extra-pulmonary dissemination of Mycobacterium tuberculosis”. Tuberculosis. 90 (6): 361–366. doi:10.1016/j.tube.2010.08.005. PMID 20829117.
[2] Sharma, Surendra Kumar; Mohan, Alladi; Sharma, Anju; Mitra, Dipendra Kumar (July 2005). “Miliary tuberculosis: new insights into an old disease”. The Lancet Infectious Diseases. 5 (7): 415–430. doi:10.1016/S1473-3099(05)70163-8. PMID 15978528.
[3] Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; & Mitchell, Richard N. (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. pp. 516–522 ISBN 978-1-4160-2973-1
[4] Al Jumaah, Suliman (2012). “Tuberculosis”. In Elzouki, Abdelaziz Y.; Harfi, Harb A.; Nazer, Hisham M.; Stapleton, F. Bruder; Oh, William; Whitley, Richard J. (eds.). Textbook of Clinical Pediatrics. Berlin, Heidelberg: Springer Berlin Heidelberg. pp. 1053–1059. doi:10.1007/978-3-642-02202-9_95. ISBN 978-3-642-02201-2.
[5] Krishnan, Nitya; Robertson, Brian D.; Thwaites, Guy (November 2010). “The mechanisms and consequences of the extra-pulmonary dissemination of Mycobacterium tuberculosis”. Tuberculosis. 90 (6): 361–366. doi:10.1016/j.tube.2010.08.005. PMID 20829117.
[6] Sharma, Surendra K.; Mohan, Alladi; Sharma, Abhishek (May 2012). “Challenges in the diagnosis & treatment of miliary tuberculosis”. The Indian Journal of Medical Research. 135 (5): 703–730. ISSN 0971-5916. PMC 3401706. PMID 22771605.
[7] Ko, Y-C.; Lee, C-T.; Cheng, Y-F.; Hung, K-H.; Kuo, C-Y.; Huang, C-C.; Chen, J-B. (2004-07-21). “Hypercalcaemia and haemophagocytic syndrome: rare concurrent presentations of disseminated tuberculosis in a dialysis patient: Hypercalcaemia and Haemophagocytic Syndrome”. International Journal of Clinical Practice. 58 (7): 723–725. doi:10.1111/j.1368-5031.2004.00054.x. PMID 15311732.
[8] Soofi, A., Malik, A., Khan, J., & Muzzafer, S. (2004). Severe Hypercalcemia in Tuberculosis. J Pak Med Assoc, 54(4), 213–215.
[9] Rodin, Frank H.; Dickey, Lloyd B. (June 1928). “Tubercle of the Choroid in Miliary Tuberculosis: Case Report”. California and Western Medicine. 28 (6): 807–809. ISSN 0093-4038. PMC 1655892. PMID 18740728.
[10] Sahn, Steven A.; Neff, Thomas A. (April 1974). “Miliary tuberculosis”. The American Journal of Medicine. 56 (4): 495–505. doi:10.1016/0002-9343(74)90482-3. PMID 4206484.
[11] Divinagracia R, Harris HW. Miliary tuberculosis. In: Schlossberg D, editor. Tuberculosis and Nontuberculous Mycobacterial Infection. Philadelphia: WB Saunders; 1999. pp. 271–284.
[12] Donald, P; Schaaf, H; Schoeman, J (April 2005). “Tuberculous meningitis and miliary tuberculosis: the Rich focus revisited”. Journal of Infection. 50 (3): 193–195. doi:10.1016/j.jinf.2004.02.010. PMID 15780412.
[13] 35.Sharma SK, Mohan A, Pande JN, Prasad KL, Gupta AK, Khilnani GC. Clinical profile, laboratory characteristics and outcome in miliary tuberculosis. QJM. 1995;88:29–37. [PubMed] [Google Scholar][Ref list]
[14] Al-Jahdali H, Al-Zahrani K, Amene P, et al. Clinical aspects of miliary tuberculosis in Saudi adults. Int J Tuberc Lung Dis. 2000;4:252–255. [PubMed] [Google Scholar]
[15] Hopewell PC, Pai M, Maher D, Uplekar M, Raviglione MC. International standards for tuberculosis care. Lancet Infect Dis. 2006;6:710–725. doi: 10.1016/S1473-3099(06)70628-4.
[16] Cattamanchi A, Smith R, Steingart KR, et al. Interferon-gamma release assays for the diagnosis of latent tuberculosis infection in HIV-infected individuals: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2011;56:230–238. doi: 10.1097/QAI.0b013e31820b07ab.
[17] Daikos GL, Uttamchandani RB, Tuda C, et al. Disseminated miliary tuberculosis of the skin in patients with AIDS: report of four cases. Clin Infect Dis. 1998;27:205–208. doi: 10.1086/514608.
[18] Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res. 2004;120:316–353.
[19] Ichiya Y, Kuwabara Y, Sasaki M, et al. FDG-PET in infectious lesions: the detection and assessment of lesion activity. Ann Nucl Med. 1996;10:185–191. doi: 10.1007/BF03165391.
[20] Ibrarullah M, Mohan A, Sarkari A, Srinivas M, Mishra A, Sundar TS. 2002. Abdominal tuberculosis: diagnosis by laparoscopy and colonoscopy.Trop Gastroenterol23:150–153.
[21] Sahn SA, Neff TA. Miliary tuberculosis. Am J Med. 1974;56:495–505. doi: 10.1016/0002-9343(74)90482-3. [DOI] [PubMed] [Google Scholar]
[22] Divinagracia R, Harris HW. Miliary tuberculosis. In: Schlossberg D, editor. Tuberculosis and Nontuberculous Mycobacterial Infection. Philadelphia: WB Saunders; 1999. pp. 271–284. [Google Scholar]
[23] World Health Organization. Treatment of Tuberculosis: Guidelines for National Programmes. 3rd ed. Geneva: WHO; 2003.
[24] Blumberg HM, Burman WJ, Chaisson RE, et al. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003;167:603–662. doi: 10.1164/rccm.167.4.603
[25] National Institute for Health and Clinical Excellence, National Collaborating Centre for Chronic Conditions. Management of non-respiratory tuberculosis. Tuberculosis: Clinical Diagnosis and Management of Tuberculosis, and Measures for Its Prevention and Control. London: Royal College of Physicians; 2006. pp. 63–76.
[26] World Health Organization. Treatment of Tuberculosis: Guidelines for National Programmes. 3rd ed. Geneva: WHO; 2003.
[27] American Academy of Pediatrics Committee on Infectious Diseases: Chemotherapy for tuberculosis in infants and children. Pediatrics. 1992;89:161–165. No authors listed.
[28] World Health Organization. Rapid Advice: Antiretroviral Therapy for HIV Infection in Adults and Adolescents. Geneva: WHO; 2009.
[29] Pozniak AL, Coyne KM, Miller RF, et al. BHIVA treatment guidelines for (TB)/HIV infection 2005. HIV Med. 2011;12:517–524.
[30] Hussey G, Chisholm T, Kibel M. Miliary tuberculosis in children: a review of 94 cases. Pediatr Infect Dis J. 1991;10:832–836. doi: 10.1097/00006454-199111000-00008. [DOI] [PubMed] [Google Scholar][Ref list]
[31] Slavin RE, Walsh TJ, Pollack AD. Late generalized tuberculosis: a clinical pathologic analysis and comparison of 100 cases in the preantibiotic and antibiotic eras. Medicine (Baltimore) 1980;59:352–366. [PubMed] [Google Scholar][Ref list]
[1335] .Sharma SK, Mohan A, Pande JN, Prasad KL, Gupta AK, Khilnani GC. Clinical profile, laboratory characteristics and outcome in miliary tuberculosis. QJM. 1995;88:29–37. [PubMed] [Google Scholar][Ref list]