
{kind=link}

Naegleria Fowleri Learn Naegleria fowleri also known as the brain-eating amoeba is a unicellular, free-living and thermophilic organism. These organisms are known to inhabit warm freshwater environments such as poorly chlorinated swimming pools, hot springs, rivers, and lakes. It grows in the environments that are conducive to its development. They are capable of living in temperatures of up to approximately 45°C therefore enable them to survive in tropical and subtropical areas in the world.[1] This amoeba is an etiological agent that causes primary amoebic meningoencephalitis (PAM).
It is a rapidly progressive central nervous system disorder. The incubation period of the disease is usually between 1 and 9 days and the disease spreads at an alarming rate.[2] PAM cannot be diagnosed clinically because its first symptoms are not specific. Despite reported cases of N. fowleri–associated PAM on nearly all continents, the actual disease incidence is underreported or underdiagnosed.
Life Cycle of N. Fowleri: Naegleria Fowleri Learn
N. fowleri has a three-stage life cycle.These are trophozoites, flagellates, and cysts.
Trophozoite Stage
The trophozoite stage is the invasive and reproductive form responsible for human infection. Trophozoites are amoeboid in shape. They measure about 10–25 micrometres in length and have pseudopodia so that they move and ingest bacteria.[3] They can produce megacolonies. The trophozoites are bacteria and fungi predators in warm water. They are capable of encasing and settling into sediments in case the water temperature reduces. As thermophilic organisms, they are most active during the warm summer when human exposure is more likely.
Flagellate Stage
Under poor nutritional conditions, the trophozoites transition into a temporary flagellate form by developing two flagella, which enable rapid movement in water.
Cyst Stage
When unfavorable conditions persist, flagellates transform into a metabolically inactive form called cysts. They are usually 7 to 12 micrometres in size. Cysts are resistant to environmental stress but are not found in human tissue.[4]
How Naegleria fowleri Enters the Body?
Trophozoites are the only stage capable of infecting humans. Infection occurs when contaminated water enters the nasal passages, mainly through freshwater exposure during swimming, diving, or nasal irrigation using nonsterile water.[5] Moreover, religious practices such as ablution (ritual nasal rinsing) using contaminated tap water have also been associated with PAM cases. In Karachi, Pakistan, clusters of PAM cases were reported in individuals who had no history of swimming or diving but regularly performed ablution with tap water that likely contained N. fowleri.[6]
Pathophysiology of N. Fowleri PAM
Human beings can only be infected by trophozoites. Infection takes place when contaminated water gets into the nasal passages primarily via freshwater contact and rinsing the nose with non sterile water. Once inhaled through the nasal cavity, they get into the brain by using the olfactory nerves, cross the cribriform plate, infect the central nervous system and settle in the brain tissues.The olfactory bulbs and the inferior frontal lobes are the typical initial locations. Herniation, hemorrhagic necrosis, cerebral edema and even death are the features of PAM. .[7]
The macrophages and neutrophils are activated as a result of an innate immune response caused by trophozoites. Their virulence is determined by several factors, including nitric oxide production, Nfa1 protein and pore-forming proteins. The Nfa1 protein facilitates the attachment of amoeba to the target cells. The specialized feeding structures of the amoeba enable them to ingest fungi and bacteria present in the environment and directly phagocytose brain cells. In addition to this, the trophozoites also cause tissue damage through the release of cytolytic molecules such as phospholipases, cysteine proteases, and other phospholipolytic enzymes. They mediate extensive necrosis, causing serious destruction of brain parenchymal tissues that cause the progressive spread of PAM.[8]
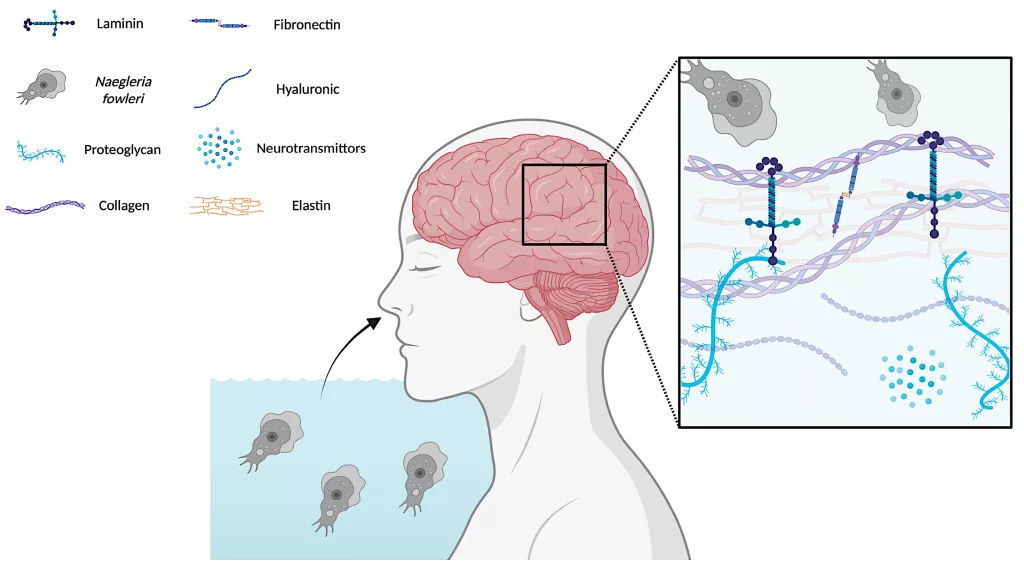
Following inhalation,Naegleria fowleritrophozoites migrate towards the brain. The parasite’s surface-binding proteins specifically recognize and attach to various structural components of the ECM. This interaction facilitates the invasion of the ECM, enabling the trophozoites to penetrate deeper into the brain tissue. Image Courtesy: Potential Inhibitors of Human–Naegleria fowleriInteractions: An In Vitro Extracellular Matrix-Based Model by Chao-Pellicer et al. 2025, doi.org/10.3390/md23080306, available via:MDPIUnder license CC BY 4.0.
Symptoms of N. fowleri Infection
The initial symptoms include:
- Headache
- Fever
- Nausea
- Vomiting
- Lethargy
- Altered mental status[9]
As the disease progresses, more severe symptoms develop, such as:
- Neck stiffness
- Confusion
- Seizures
- Photophobia
- Cranial nerve abnormalities
Notably, most cases progress rapidly, leading to coma and death within days of symptom onset.
Diagnosis of Naegleria Fowleri PAM
Diagnosis of the condition is through the following steps:
History and Physical Examination
Proper physical examination and patient history is vital in the diagnosis of PAM. Clinical manifestation of the condition is difficult to diagnose because of non-specific manifestation in the first stages which are similar to flu-like disease, viral meningitisor bacterial meningitis. The clinicians should be familiar with all the epidemiological risk factors and possible exposures. Under-detection of PAM may lead to early diagnosis and early death. Also, it is important to note that the accuracy of epidemiological history is also important in identifying the severity of the disease. Delayed recognition often results in delayed diagnosis and poor outcomes.
Laboratory Findings
The clinicians also carry out special laboratory tests on the brain tissues or cerebral spinal fluid (CSF) to make the diagnosis further. Non-specifically, however, the laboratory findings may be non-specific.
- The CSF results may commonly resemble bacterial meningitis with elevated protein levels, neutrophilic pleocytosis, and low-to-normal glucose levels.. These tests also had high CSF pressures with their recorded values going as high as 600 mm H2O in some of the patients.Hence, standard laboratory tests are not even sufficient to establish a diagnosis.[10]
- A quick method involves visualizing trophozoites directly using a wet mount. The staining methods are also used by the clinicians, including hematoxylin and eosin (H&E), periodic acid–Schiff (PAS), and Giemsa-Wright.
- PCR is the gold standard of diagnosing PAM because it has the power of detecting the N. fowleri DNA in the CSF.
- Clinicians can also perform Immunohistochemical antigen detection.[11]
- Standard bacterial cultures are usually unreliable, as the fixation process can kill the amoeba.
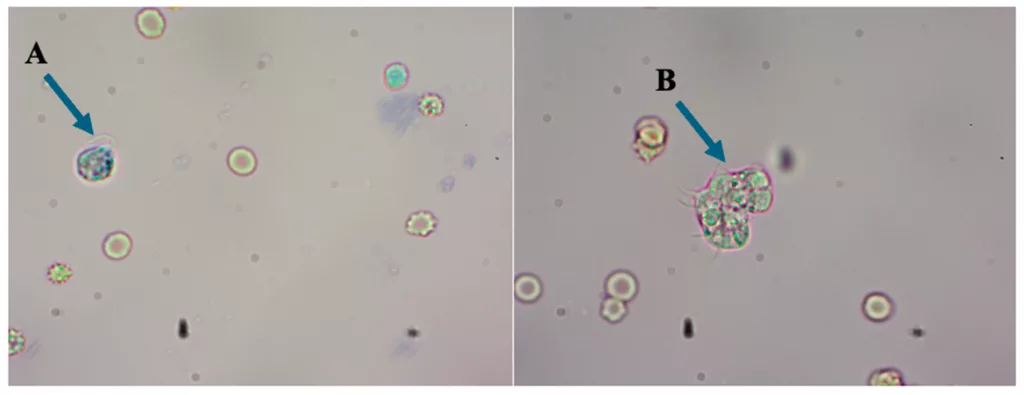
The “brain-eating” ameba in CSF were detected by direct microscopic examination under the wet preparation that showed the flagellated form (A) and the trophozoites form (B). Original magnification ×40. Image Courtesy:Naegleria fowleri:Portrait of a Cerebral Killer by Phung et al. 2025, available via:MDPI, under license CC BY 4.0.
Other Diagnostic Techniques
Magnetic resonance imaging (MRI) can reveal diffuse hemorrhages, infarctions, or contrast enhancement in affected regions of the brain as the infection advances. Its findings are often non-specific in the early stages of infection.
Brain biopsy can also provide definitive diagnosis. The histopathological examination reveals hemorrhagic meningitis. These findings show severely affected areas, such as the olfactory bulb and the base of the brain.
Advance Techniques
Advanced diagnostic techniques include:
Metagenomics Next Generation Sequencing (mNGS)
It has recently gained attention as a promising diagnostic tool for free-living amoeba. This shotgun sequencing method enables broad pathogen detection from CSF, tissue, or serum samples (without requiring large specimen volumes.[12]
Microbial Cell Free DNA Analysis
This analysis can also detect free-living amoeba. The emerging sequencing technology can have the potential to reduce diagnostic delays.
Loop-Mediated Isothermal Amplification (LAMP)
LAMP is a novel technique to amplify specific DNA regions. It is cheaper, quicker, and more sensitive, and can provide multiple amplification products at a consistent temperature. This technology can improve early detection, ultimately enhancing the patient’s outcomes.
Differential Diagnosis of N. fowleri Infection
Early symptoms of Naegleria fowleri infection, such as headache, fever, nausea, and lethargy, can resemble other serious brain infections. Correctly distinguishing PAM from these conditions is critical because delays in diagnosis can be fatal.
| Condition | Similarities with PAM | Key Differences |
|---|---|---|
| Bacterial meningitis | Fever, headache, neck stiffness, nausea | Usually slower progression; less often linked to freshwater exposure; CSF culture can identify bacteria |
| Viral meningoencephalitis (e.g., HSV, enterovirus) | Confusion, seizures, fever | Often slower onset; PCR can detect viral DNA; rare history of nasal freshwater exposure |
| Other free-living amoebae (Acanthamoeba, Balamuthia) | Headache, neurological deficits, seizures | More chronic course; less abrupt onset; infection often via skin or respiratory route rather than nasal exposure |
Management and Treatment of N. Fowleri Infection
Management and treatment options are only a few:
The recommended treatment usually involve a combination of five or six anti-fungal or antimicrobial agents. Miltefosine is the most recent addition to the regimen, and other drugs commonly include:
- Azithromycin
- Amphotericin B
- Rifampin
- Fluconazole
- Dexamethasone (adjunctive therapy to reduce cerebral edema)
Amphotericin B is the primary drug of choice due to its amebicidal activity even at low concentrations.[13] Early initiation of therapy and intensive neurocritical care are crucial for survival.
Prognosis of Naegleria Fowleri PAM
N. fowleri PAM is a rare but rapidly progressive disorder with poor prognosis even when treatment is administered. This infectious disease is associated with a mortality rate exceeding 98%.[14] Diagnosing the infection is challenging due to limited awareness among healthcare providers. This can be attributed to its initial symptoms which are similar to those of bacterial infection, viral or flue-like syndromes.
Although recovery is extremely rare, early recognition, aggressive combination therapy, and intensive neurocritical care can improve outcomes in exceptional cases. However, survivors may experience long-term neurological complications, including cranial nerve dysfunction, seizures, or cognitive impairments.[15]
Possible Complications
The infection may cause some complications and they include:
- Hemorrhagic necrosis
- Heightened intracranial pressure
- Cerebral edema
- Brain herniation
- Seizures
- Hydrocephalus
- Cranial nerve dysfunction
- Coma
How to Prevent Naegleria fowleri Infection?
To reduce the risk of infection, it is important to ensure that the water people come into contact with is safe:
- Ensure proper chlorination and regular maintenance of Swimming pools and hot tubs. Avoid swimming in pools that are poorly chlorinated or untreated.
- Avoid submerging the head or inhaling water from warm lakes, rivers, and hot springs, especially during summer when N. fowleri thrives.
- Nasal irrigation and religious practices such as ablution should use sterile, distilled, filtered, or previously boiled water.
- Regularly clean water tanks, storage containers, and plumbing systems, especially in tropical and subtropical areas where the amoeba can survive in warm water.
Final Remarks
N. fowleri is a lethal pathogen, which may lead to serious infectious diseases. Therefore, early diagnosis and immediate treatment are critical to improving patient outcomes. The infection can occur by the entrance of contaminated water in nasal passages accompanied by severe inflammation and necrosis. Because the disease progresses so quickly, clinicians must monitor affected patients closely and continuously. Furthermore, preventive measures, such as following proper water safety practices and using sterile water for nasal irrigation or ablution, are critical to reduce the risk of infection.
References
[1] Pervin, N., & Sundareshan, V. (2025). Naegleria Infection and Primary Amebic Meningoencephalitis. InStatPearls [Internet]. StatPearls Publishing.
[2] Pervin, N., & Sundareshan, V. (2025). Naegleria Infection and Primary Amebic Meningoencephalitis. InStatPearls [Internet]. StatPearls Publishing.
[3] Güémez, A., & García, E. (2021). Primary amoebic meningoencephalitis by Naegleria fowleri: pathogenesis and treatments.Biomolecules,11(9), 1320.
[4] Güémez, A., & García, E. (2021). Primary amoebic meningoencephalitis by Naegleria fowleri: pathogenesis and treatments.Biomolecules,11(9), 1320.
[5] Centers for Disease Control and Prevention (CDC. (2013). Notes from the field: primary amebic meningoencephalitis associated with ritual nasal rinsing–St. Thomas, US Virgin islands, 2012.MMWR. Morbidity and mortality weekly report,62(45), 903.
[6] Shakoor S, Beg MA, Mahmood SF, et al. Primary Amebic Meningoencephalitis Caused byNaegleria fowleri, Karachi, Pakistan.Emerg Infect Dis. 2011;17(2):258-261. doi:10.3201/eid1702.100442
[7] Gharpure, R., Bliton, J., Goodman, A., Ali, I. K. M., Yoder, J., & Cope, J. R. (2021). Epidemiology and clinical characteristics of primary amebic meningoencephalitis caused by Naegleria fowleri: a global review.Clinical Infectious Diseases,73(1), e19-e27.
[8] Marciano-Cabral, F., & Cabral, G. A. (2007). The immune response to Naegleria fowleri amebae and pathogenesis of infection.FEMS Immunology & Medical Microbiology,51(2), 243-259.
[9] Rehman, S. U., Farooq, S., Tariq, M. B., Nasir, N., Wasay, M., Masood, S., & Karim, M. (2023). Clinical manifestations and outcome of patients with primary amoebic meningoencephalitis in Pakistan. A single-center experience.Plos one,18(11), e0290394.
[10] Grace, E., Asbill, S., & Virga, K. (2015). Naegleria fowleri: pathogenesis, diagnosis, and treatment options.Antimicrobial agents and chemotherapy,59(11), 6677-6681.
[11] Visvesvara, G. S. (2010). Amebic meningoencephalitides and keratitis: challenges in diagnosis and treatment. Current Opinion in Infectious Diseases, 23(6), 590-594.
[12] Haston, J. C., & Cope, J. R. (2023). Amebic encephalitis and meningoencephalitis: an update on epidemiology, diagnostic methods, and treatment.Current opinion in infectious diseases,36(3), 186-191.
[13] Alanazi, A., Younas, S., Ejaz, H., Alruwaili, M., Alruwaili, Y., Mazhari, B. B. Z., … & Junaid, K. (2025). Advancing the understanding of Naegleria fowleri: Global epidemiology, phylogenetic analysis, and strategies to combat a deadly pathogen.Journal of Infection and Public Health, 102690.
[14] Pervin, N., & Sundareshan, V. (2025). Naegleria Infection and Primary Amebic Meningoencephalitis. InStatPearls [Internet]. StatPearls Publishing.
[15] Linam WM, Ahmed M, Cope JR, Chu C, Visvesvara GS, da Silva AJ, Qvarnstrom Y, Green J. Successful treatment of an adolescent with Naegleria fowleri primary amebic meningoencephalitis. Pediatrics. 2015 Mar;135(3):e744-8. doi: 10.1542/peds.2014-2292. Epub 2015 Feb 9. PMID: 25667249; PMCID: PMC4634363.