
{kind=link}

Choroid plexus cysts are small, fluid-filled spaces seen in the fetal brain during routine ultrasound in pregnancy. They are usually benign and often resolve on their own, especially when no other abnormalities are present. However, they may sometimes be evaluated further due to their association with trisomy 18.
What are Choroid Plexus Cysts?
During the development of the fetus, the choroid plexus develops in the ventricular system of the brain. It is a network of specialised cells that plays an important role in the proper functioning of the central nervous system. It is a secretory epithelium that produces cerebrospinal fluid. Cysts can arise from the choroid plexus during fetal development. These cysts appear as bubble-like structures filled with fluid. Fetal choroid plexus cysts form as a result of the accumulation of cerebrospinal fluid in the villi of the choroid plexus. These are usually harmless and can resolve as the gestation progresses.
Ultrasound examination during pregnancy or at autopsy detects the cysts. These cysts are completely benign. However, various reports suggest a link between choroid plexus cysts and aneuploidy (a condition in which a cell contains an abnormal number of chromosomes), especially trisomy 18. In contrast, the association with trisomy 21 is weak and not considered clinically significant.
Choroid Plexus Cysts and Trisomy 18
Choroid plexus cysts are a sensitive but non-specific indication of trisomy 18, a serious genetic condition. It is also known as Edward syndrome. Normal fetuses carry two copies of chromosome number 18. However, in the presence of Edward syndrome, there are three copies of this chromosome. If a fetus carries this syndrome, organ abnormalities develop, making it difficult for the fetus to survive till birth.
Fetal choroid plexus cysts alone can not confirm the presence of trisomy 18. Fetuses with trisomy 18 also have structural abnormalities along with cysts. The first sign of trisomy 18 is the larger size of the cyst than normal. If it is 5 mm or greater, a detailed scan is performed. During this examination, special attention is given to the heart, abdominal wall, feet, and fingers. But if the size of the cyst is more than 1 cm, a confirmatory test is required. However, the size of the cyst alone is not a reliable indicator of trisomy 18, and both small and large cysts can be seen in normal fetuses.
A skilled person should perform the test to identify the features of aneuploidy. Ultrasound examination can detect some anomalies associated with trisomy 18 in fetuses. These include overlapping fingers, retardation of intrauterine growth, micrognathia, cleft lip, heart defects, rocker-bottom feet, polyhydramnios, and flexion deformities. Other features of trisomy 18 include hydronephrosis, diaphragmatic hernia, omphalocele, and oesophageal atresia.
Epidemiology
Studies suggest that fetal choroid plexus cysts are found in 0.18% to 3.6% of ultrasound examinations during pregnancy. Choroid plexus cysts are a cause for concern when associated with trisomy 18 and trisomy 21, and researchers are more concerned about trisomy 18, as the prevalence of these cysts in the general population and in fetuses with trisomy 21 is the same. Choroid plexus cysts are observed on prenatal sonography in 44-50% of pregnancies with trisomy 18; in trisomy 21 cases, they occur in only 1.4%.
Formation of Choroid Plexus Cysts
Understanding the developmental process of the choroid plexus helps explain how these cysts form.
Development of the Choroid Plexus
Histopathological development of the choroid plexus occurs in four stages.
Stage I
The first stage starts at week 7 of gestation and continues until the 9th week. At this stage of development, the choroid plexus occurs as a short stalk in the form of a club, and a neuroepithelium covers it. By the end of this first stage, minor lobulation of the stalk occurs.
Stage II
The second stage starts at the 9th week of pregnancy and ends at the 17th week. This is a period of rapid growth during which the choroid plexus becomes lobulated. Moreover, finger-like projections form and are covered by secretory epithelium.
Stage III
The third stage begins at week 17th and terminates at week 28 of gestation. Lobulation continues, and primary villi become plentiful. The surface epithelium folds into the stroma, forming tubules. The rate of tubule formation becomes equal to the rate of development of villi and lobulations. The volume of the loose stroma decreases by the end of this stage.
Stage IV
This stage begins at week 29 and continues until birth. The villi become delicate and form small branches. There is an abundance of tubules, and the connective tissue replaces the mesenchymal elements.
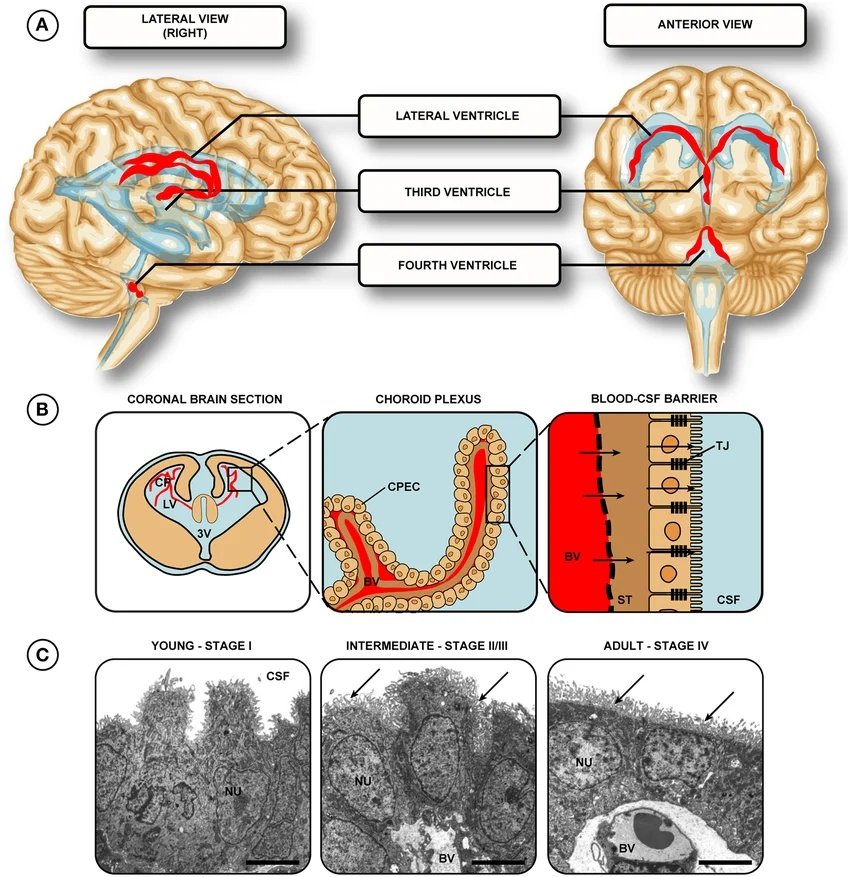
Location of choroid plexuses in the human brain. Image Courtesy: Development of the choroid plexus and blood-CSF barrier by Liddelow, 2015,10.3389/fnins.2015.00032, available via: https://www.researchgate.net/figure/Location-of-choroid-plexuses-in-the-human-brain-A-The-choroid-plexuses-are-present-in_fig1_273784823, CC BY 4.0.
Formation of the Cyst
Choroid plexus cysts are most often observed at the mid- or late-second trimester during routine screening examinations to detect abnormalities. This time period coincides with stage III of choroid plexus development. During this period of rapid growth, villous enlargement leads to cyst formation. The cerebrospinal fluid becomes trapped among the twisted villi, giving a cyst-like appearance on ultrasound. As the amount of loose stroma decreases, the regression of fluid collections may occur. Most cysts resolve spontaneously by 24–28 weeks of gestation.
Pathologic Features of Choroid Plexus Cysts
The pathologic features of choroid plexus cysts have not been widely studied. In a study involving two normal fetuses and one with trisomy 18, the appearance of these cysts was demonstrated. In each fetus, loose stromal tissue surrounded the cyst, and the cyst had no epithelial lining. These are considered pseudocysts rather than true cysts, as they lack a true epithelial lining and represent fluid trapped within the folds of the choroid plexus.
In another study, it was described that the cysts have a clear fluid surrounded by normal choroid plexus tissue.

The sagittal plane of the fetal head shows a choroid plexus cyst. Image Courtesy: Ultrasonographic soft markers of aneuploidy in second-trimester fetuses by Ali et al, 2012,10.1016/j.mefs.2012.04.007, available via: https://www.researchgate.net/figure/Sagittal-plane-of-the-fetal-head-shows-a-choroid-plexus-cyst_fig3_235655737, CC BY 4.0.
Diagnosing Choroid Plexus Cyst
Choroid plexus cysts are often detected by chance on imaging studies, primarily during routine prenatal ultrasound, which is the standard and most important diagnostic tool. At autopsy, small cysts are commonly found. These cysts can be diagnosed using various approaches such as magnetic resonance imaging (MRI), computed tomography (CT) scan, and ultrasonography. However, on CT, the cyst wall is not generally visible. The demonstration of the cyst, which is crucial for diagnosis, can be best achieved with T1-weighted MRI or proton-density-weighted images. On serial examination, MRI can be useful for observing cyst size.
Choroid Plexus Cysts Management
In most cases, cysts in the choroid plexus are benign. But, these cysts are a cause of concern if aneuploidy is also present. During pregnancy, routine examinations are performed. Cysts can be observed at gestational weeks 17-19. If the cyst is isolated (i.e., no other structural abnormalities are present), it is considered a normal variant and typically requires no further intervention.
If the size is between 5 mm and 1 cm or more than that, further evaluation is based on the presence of additional abnormalities or abnormal prenatal screening results, rather than cyst size alone. For this purpose, a detailed scan is performed at week 20–22. In the absence of any other anomaly, no further action is required. If there are structural abnormalities in other parts of the body, it is important to find out the reason. Management in such cases involves genetic counseling and appropriate prenatal testing (such as non-invasive prenatal testing or amniocentesis), with decisions made based on overall risk assessment.
Choroid Plexus Cysts VS Choroid Plexus Tumors
The given table highlights some differences between the cysts and the tumors that form in the choroid plexus. These two mainly differ in appearance, biological behavior, vulnerable age group, epidemiology, symptoms, prognosis, and treatment.
| Feature | Choroid Plexus Cysts | Choroid Plexus Tumors |
|---|---|---|
| Definition | Commonly found in fetuses during the second trimester | Usually benign, they terminate on their own |
| Appearance | Small and circular | Appear like a cauliflower and have irregular borders |
| Epidemiology | Found in 1.8-3.6% of ultrasound examinations during pregnancy12Gupta, J. K., Farrell, T. A., Hau, C. M., Cave, M., Lilford, R. J., Irving, H. C., & Mason, G. (1995). Clinical significance of fetal choroid plexus cysts.The Lancet,346(8977), 724-729. | Account for 0.4-0.8% of all brain tumors13Zülch, K. J. (1986). The origin of brain tumors. InBrain Tumors: Their Biology and Pathology(pp. 41-84). Berlin, Heidelberg: Springer Berlin Heidelberg. |
| Age Group | Neoplasms that arise from the epithelium of the choroid plexus | Mostly observed in children |
| Biological behavior | Usually benign, terminate on their own | Can be benign or malignant and require treatment |
| Symptoms | Mostly asymptomatic | Increased pressure within the skull, irritability, headaches, vomiting14Rickert, C. H., & Paulus, W. (2001). Tumors of the choroid plexus.Microscopy research and technique,52(1), 104-111. |
| Prognosis | Excellent | Excellent for benign tumors, relatively lower for malignant tumors |
| Treatment | Usually do not require treatment | Surgery, chemotherapy, radiation therapy |
Conclusion
The choroid plexus develops in the ventricular system of the brain. It plays an important role in the proper functioning of the central nervous system. During fetal development, cysts can arise from the choroid plexus. These cysts are mostly benign and resolve on their own. However, it is also suggested that the cysts are linked to trisomy 18 or trisomy 21, but other structural abnormalities should also be considered along with choroid plexus cysts for the diagnosis of these conditions. Choroid plexus cysts are commonly found during ultrasound examination of the fetus and also at autopsy.
These cysts appear as bubble-like structures filled with fluid. Cysts can be diagnosed using MRI, CT scan, and various other approaches. However, ultrasound remains the primary diagnostic tool in clinical practice. Treatment is usually not required, but if aneuploidy is present, further action is taken. Tumors in the choroid plexus are different from cysts in terms of biological behaviour, appearance, prognosis, and treatment.
References
[1] Mihaljevic, S., Michalicova, A., Bhide, M., & Kovac, A. (2021). Pathophysiology of the choroid plexus in brain diseases.General Physiology & Biophysics,40(6).
[2] Walkinshaw, S. A. (2000). Fetal choroid plexus cysts: are we there yet?.Prenatal diagnosis,20(8), 657-662.
[3] Ostlere, S. J., Irving, H. C., & Lilford, R. J. (1990). Fetal choroid plexus cysts: a report of 100 cases.Radiology,175(3), 753-755.
[4] Ostlere, S. J., Irving, H. C., & Lilford, R. J. (1990). Fetal choroid plexus cysts: a report of 100 cases.Radiology,175(3), 753-755.
[5] Kennedy, K. A., & Carey, J. C. (1993, February). Choroid plexus cysts: significance and current management practices. InSeminars in ultrasound, CT, and MR(Vol. 14, No. 1, pp. 23-30).
[6] Gupta, J. K., Farrell, T. A., Hau, C. M., Cave, M., Lilford, R. J., Irving, H. C., & Mason, G. (1995). Clinical significance of fetal choroid plexus cysts.The Lancet,346(8977), 724-729.
[7] Kennedy, K. A., & Carey, J. C. (1993, February). Choroid plexus cysts: significance and current management practices. InSeminars in ultrasound, CT, and MR(Vol. 14, No. 1, pp. 23-30).
[8] Farhood, A. I., Morris, J. H., Bieber, F. R., Opitz, J. M., & Reynolds, J. F. (1987). Transient cysts of the fetal choroid plexus: morphology and histogenesis.American journal of medical genetics,27(4), 977-982.
[9] Gabrielli, S., Reece, E. A., Pilu, G., Perolo, A., Rizzo, N., Bovicelli, L., & Hobbins, J. C. (1989). The clinical significance of prenatally diagnosed choroid plexus cysts.American journal of obstetrics and gynecology,160(5), 1207-1210.
[10] Guermazi, A., De Kerviler, E., Zagdanski, A. M., & Frija, J. (2000). Diagnostic imaging of choroid plexus disease: pictorial review.Clinical radiology,55(7), 503-516.
[11] Ostlere, S. J., Irving, H. C., & Lilford, R. J. (1990). Fetal choroid plexus cysts: a report of 100 cases.Radiology,175(3), 753-755.
[12] Gupta, J. K., Farrell, T. A., Hau, C. M., Cave, M., Lilford, R. J., Irving, H. C., & Mason, G. (1995). Clinical significance of fetal choroid plexus cysts.The Lancet,346(8977), 724-729.
[13] Zülch, K. J. (1986). The origin of brain tumors. InBrain Tumors: Their Biology and Pathology(pp. 41-84). Berlin, Heidelberg: Springer Berlin Heidelberg.
[14] Rickert, C. H., & Paulus, W. (2001). Tumors of the choroid plexus.Microscopy research and technique,52(1), 104-111.