
{kind=link}

Pulmonary Tuberculosis Warning Pulmonary tuberculosis, historically known as the “Great White/White Plague”, is a contagious bacterial infection of the lungs that can cause serious breathing impairments and even death. Mycobacterium Tuberculosis is the causative agent of the disease. TB is also known as Pthisis and Pthisis Pulmonalis. According to the WHO, TB is a common disorder and the leading cause of death worldwide (from a single infectious agent) that caused approximately 1.3 million deaths globally in 2023. The bacteria can stay inactive in your body in a dormant form or become active and cause havoc. Doctors treat the microbial infection with a combination of antibiotics. Timely treatment can cure the infection, but if left untreated, TB can cause life-threatening pulmonary complications and death.
Types Of Pulmonary Tuberculosis: Pulmonary Tuberculosis Warning
There are different classifications of TB. However, doctors most commonly divide tuberculosis based on the activation of the bacteria. Latent TB is characterized by the entry of the bacterium into the body, but without clinical disease or symptoms, whereas active TB has evident manifestations.
Latent TB
This type is characterized by the presence of tuberculous bacteria in an inactive form. While the person has the causative agent inside the body, there are no symptoms, and thus, it is not infectious. However, it can progress to active disease if immunity weakens. Most infected individuals worldwide have latent TB infection, not active disease.
Active TB
As the name indicates, the bacteria gain entry into your body and actively multiply. This multiplication makes you sick and a source of infection for others. Only people with active pulmonary TB are contagious.
The most common site of TB is the lungs. However, it can infest other parts of the body (like the kidneys or the brain, etc.), where it is known as extrapulmonary TB.
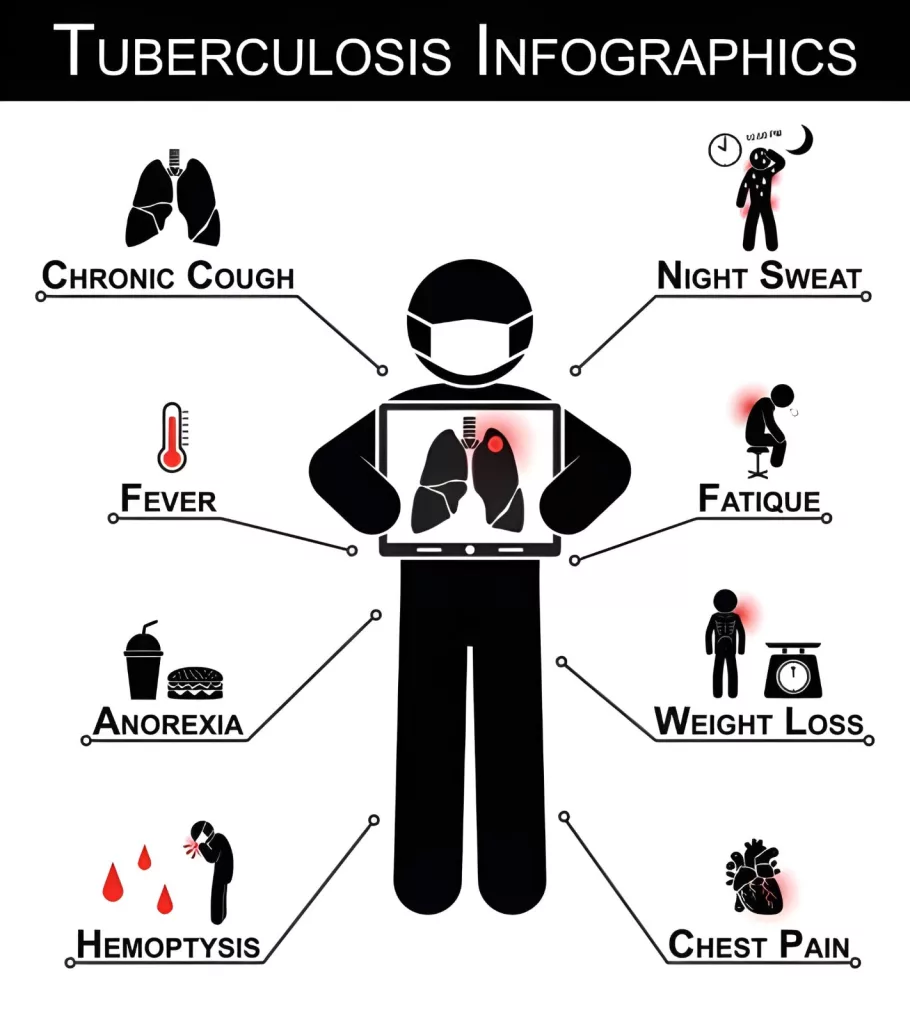
Pulmonary Tuberculosis Symptoms
Pthisis Pulmonalis is a common condition. Therefore, doctors across the globe are well aware of its symptoms. Sometimes, doctors divide symptoms into pulmonary (related to the lungs) and constitutional (extra-pulmonary) symptoms. The most common problems caused by TB include:
Pulmonary tuberculosis symptoms
Cough:
A highly prevalent symptom that directly affects the quality of life of pulmonary TB patients is a persistent cough that lasts for long periods. Generally, doctors order pulmonary tuberculosis tests if a patient presents with a cough lasting for more than 3 weeks (standard TB screening threshold). It is regarded as a prominent symptom of the disease, directly linked to its transmission. Some patients experience a productive cough (with phlegm/mucus) while others report a dry cough.
Clinicians have noted that TB patients, generally, have a unique coughing sound. However, cough sound alone cannot be used as a reliable diagnostic test. Due to the high prevalence of the disease in underdeveloped regions of India and Africa, mobile-based cough audio screening can aid in diagnosis and provision of health care.
Weightloss:
Unexplained weight loss is a salient feature of pthisis. Patients encounter unusual drops in weight, which are usually accompanied by other complications like headache, fatigue, chest pain, and generalized weakness. Weight loss was proven to be an important symptom among tuberculosis patients in tribal Indian populations. Multiple cases of TB present with chronic cough, appetite loss, and weight loss.
Hemoptysis:
A seriously concerning symptom for most patients is coughing up blood, i.e., hemoptysis. A productive cough is a common feature of the disease, in which patients discharge sputum/phlegm while coughing. However, sometimes, the coughed-up phlegm can have a tinge of blood in it. Tuberculosis is one of the leading global causes of hemoptysis.
The mycobacterium-induced erosion of the lung (bronchial) arteries is the main cause of bleeding. In rare instances, it leads to the formation of a dilated artery within the TB cavity, i.e., Rasmussen’s aneurysm. Patients may notice an evident amount of blood in their cough when these aneurysms rupture. Based on the amount of the expectorated blood, hemoptysis is categorized into:
- Mild: Less than 50 ml per 24 hours
- Moderate: 50-200 ml per 24 hours
- Severe: more than 200 ml per 24 hours
Ramussen’s aneurysm is known to cause massive hemoptysis in adult tuberculosis patients.
Chest Pain:
Chest pain is not always present. Most of the time, only a few patients report having it. Some patients experience mild-to-moderate localized musculoskeletal pain. However, others may suffer from sharp, stabbing pleuritic pain. Chest pain is oftenpleuriticwhen the pleura is involved. According to a clinical study, cough is present in about 75% of pulmonary tuberculosis patients, while chest pain is seen in just 4.5% cases.
Night Sweats:
A rather unique feature of the respiratory disorder is excessive sweating during sleep. Known as “night sweats”, this symptom is characterized by so much sweating during sleep that it might soak your nightclothes. This sweating arises even when the room is cold. Experts believe that the abrupt thermoregulation of the body (which causes sweating) is the body’s immune response to the Mycobacterium tuberculosis invasion. In a small number of cases, night sweats can accompany common symptoms like cough, weight loss, and fever. However, hemoptysis and night sweats are rarely reported symptoms.
Fatigue:
A number of patients are disturbed by the never-ending fatigue associated with TB. This feeling of lethargy and fatigue doesn’t go away with ample rest. This extra-pulmonary feature of the highly prevalent infectious disease has a serious impact on the quality of life of the patients. Moreover, research reveals that tuberculosis is clearly linked to an increased risk of chronic fatigue syndrome.
Fever And Chills:
A raised body temperature is seen in almost all bacterial infections, and Mycobacterium tuberculosis is no exception. In this case, there is mostly a consistent yet low-grade fever. A characteristic feature of the disorder is that the fever usually develops during the late afternoon and is accompanied by fatigue and malaise. Some patients report having chills along with a fever. Rarely, intrathoracic lymph node enlargement may be seen, especially in children.
Breathing Difficulty:
Pthisis of the lungs can contribute to breathing difficulties as well. Wheezing is not a typical feature unless there is airway compression or coexisting disease.
Appetite Loss:
Tuberculous infection in your body can alter your appetite. Several patients report a loss of appetite that can further contribute to weight loss.
Pulmonary Tuberculosis Causes
Mycobacterium tuberculosis infection causes pulmonary TB and other types of TB (extrapulmonary TB). The bacteria spread through the air via droplet nuclei released when a person with active pulmonary TB coughs, speaks, or sings. The mycobacterium then lodges in the lungs and causes symptoms.

Pulmonary tuberculosis is caused by Mycobacterium tuberculosis (rod-shaped bacteria).
Is Pthisis Contagious?
Yes, tuberculosis is a contagious disease and spreads from an infected individual (with an active lung infection) through their coughing, sneezing, laughing, or even singing. It is an air-borne infection, i.e., transmitted through the air. The bacteria can stay in the air for some time, so you may get infected even if the person is not in the room.
According to the latest clinical research, different factors like cough, hemoptysis, and weight loss can help in predicting the contagiousness of pulmonary tuberculosis. Latent TB is non-contagious.
Risk Factors
Clinicians have identified certain risk factors that increase your chances of getting infected with Mycobacterium tuberculosis. The risks are as follows:
Close Contact With the Infected Persons:
Residents of the Caribbean, Africa, and Asia are more prone due to the high prevalence of the disease. Moreover, increased exposure by caring for an infected person, working in a hospital/lab, adds to the risk.
Lifestyle Habits:
Illicit intravenous (injection) drug use, smoking, and alcohol abuse are identified as risk factors for pulmonary tuberculosis.
Comorbidities:
Several health conditions and comorbidities, like diabetes and a weakened immune system, increase the risk. You can have weak immunity if you are on immunosuppressants (after an organ transplant), receiving chemotherapy for cancer, or have an impaired immune system (infants/children have underdeveloped systems). Patients suffering from diseases like autoimmune disorders (rheumatoid arthritis) and HIV, hepatitis, also have weak immune systems and consequently higher chances of falling prey to TB.
Pulmonary Tuberculosis Diagnosis
Healthcare providers adopt different varieties of diagnostic tests to reach a diagnosis. Imaging tests provide useful information about the extent of damage caused by the infection, while body fluid tests reveal the nature of the causative agent.
History And Physical Examination:
Your doctor will take a complete history of the disease (onset of fever, night sweats, cough, etc). This is followed by a physical examination to check for fluid in the lungs.
Sputum Tests:
If suspected, healthcare providers can perform blood, sputum, and skin tests to confirm the diagnosis. Doctors look for the presence of the bacterium in your sputum. Microbial culture of the sputum sample is a “gold standard” in TB diagnosis. It involves growing suspected TB bacteria in a dish.
In the sputum smear microscopy, lab experts analyze your sputum sample under a microscope and identify bacteria using specific staining techniques. Smear microscopy detects acid-fast bacilli but is less sensitive than molecular tests. The Nucleic Acid Amplification (NAA) test detects nucleic acids of bacterial DNA. A PCR test (polymerase chain reaction) looks for the presence of certain germ genes.
Skin And Blood Tests:
TB skin and TB blood (IGRA) tests are able to identify whether a person has had pulmonary TB, but can not differentiate between active and latent disease. The IGRA test measures T-cell immune response (in response to Mycobacterium tuberculosis) in the blood. The tuberculin skin test (PPD test), also known as the Mantoux test, is done to check latent infection. In this specific pulmonary TB screening test, a healthcare provider injects a small amount of purified protein derivative (PPD) under the skin and checks your body’s immune response by measuring the size of the bump/induration that forms 48-72 hours after injection.
Imaging Tests:
A chest X-ray has been conventionally used to identify lung abnormalities like pulmonary pthisis. It can’t solely help diagnose the disorder and needs correlation with the clinical picture. Advanced scans like CT scans are superior to conventional chest X-rays in diagnosing TB.
Other Tests:
Your doctor may also perform minimally invasive tests like bronchoscopy to see the inside of your lungs (bronchial tissues). It involves inserting a small camera (with light) through your nose/mouth that goes into your lungs. Thoracocentesis involves taking a sample of pleural fluid for Mycobacterium detection. Lung biopsy (removal of small lung tissue) is often performed to rule out other pathologies.
Differential Diagnosis
Several lung conditions fall under the DD for pulmonary TB. Infectious conditions like bacterial pneumonia, bronchiectasis, sarcoidosis, and lung cancer can have similar presentations. However, doctors differentiate between the conditions with the help of diagnostic tests (cultures, DNA tests), personal and clinical pictures of the patients.
Pulmonary Tuberculosis Treatment
The mainstay of treatment is managing the lung infection, whether active or latent. In the vast majority of cases, doctors prescribe a combination of strong antibiotics to deal with the stubborn bacterial pathogen. You will need to take these drugs for six months. The most commonly prescribed pulmonary tuberculosis medicines include:
- Rifampin
- Isoniazid
- Pyrazinamide
- Ethambutol
This intensive phase usually lasts two months, followed by a continuation phase of four months with:
- Isoniazid
- Rifampicin
This regimen is widely regarded as the most effective and well-studied treatment approach for pulmonary TB. However, some patients may develop side effects such as liver toxicity, rash, visual disturbances (with ethambutol), and gastrointestinal upset, which require close medical monitoring.
For latent tuberculosis infection, doctors may prescribe shorter preventive regimens, such as isoniazid alone or rifamycin-based combination therapies, depending on patient risk factors and national treatment guidelines.
Note: YOU MUST COMPLETE YOUR ANTIBIOTIC COURSE, IRRESPECTIVE OF SYMPTOM ALLEVIATION/RESOLUTION. BECAUSE FAILING TO DO SO CAN LEAD TO THE DEVELOPMENT OF MULTI-DRUG RESISTANT TB!
To improve adherence, many TB control programs use Directly Observed Therapy (DOT) or other structured treatment-support strategies, where healthcare providers regularly supervise medication intake.
Patients with drug-resistant tuberculosis require specialized treatment using second-line medications under the care of experienced TB specialists, often for longer durations.
Pulmonary Tuberculosis Precautions
Pulmonary tuberculosis requires careful personal and public health precautions to prevent complications and reduce the risk of spreading the infection to others. Patients diagnosed with active TB should follow their healthcare provider’s advice closely and avoid missing doses of prescribed medications. Thus, to keep yourself safe, you can try these steps:
- Keep your medicines in a pill organizer. You can get one that has the days of the week mentioned.
- Take medicines at the same time of day to make a routine.
- Ask your friends or family to remind you of the medicine every day.
- Avoiding alcohol and smoking during treatment is strongly advised, as these habits can worsen lung damage and reduce the effectiveness of medications.
How Can You Prevent Pulmonary Tuberculosis?
The chances of acquiring an airborne disease can be minimized if you take the necessary actions. You can prevent pulmonary TB by avoiding extended contact with TB patients and covering your face with a mask when moving in TB common areas.

Pulmonary tuberculosis prevention can be achieved with a BCG vaccine.
You can get the BCG (Bacillus Calmette-Guerin) vaccine to prevent TB. The vaccine is made from weakened Mycobacterium bovis strains that are effective in protecting against severe forms of TB in children.
Wrapping Up
Pulmonary tuberculosis (TB) is a bacterial infection of the lungs caused by an airborne pathogen, i.e., Mycobacterium tuberculosis. It is a globally widespread infection that may take a latent (inactive) form in the infected individual. In the active state, symptoms of the disease include chronic coughing, hemoptysis, unexplained weight loss, night sweats, consistent low-grade fever, and fatigue etc. The disease spreads through coughing, sneezing, and laughing of an infected person. People caring for TB patients, having weak immunity, IV drug users, and residents of TB pandemic areas have a high risk of acquiring the disease.
Healthcare providers diagnose it with sputum tests (bacterial culture and PCR test, etc.), Mantoux test (skin test), and imaging tests (chest X-ray and CT scan). Doctors treat it with a long course (of six months) of a combination of strong antibiotics, i.e., rifampin, isoniazid, pyrazinamide, and ethambutol. Patients must complete the course of antibiotics, as an incomplete course can lead to the development of resistant disease (multidrug-resistant TB).
References
[1] World Health Organization. Tuberculosis [Internet]. Geneva: World Health Organization; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
[2] Turner, R. D. (2019). Cough in pulmonary tuberculosis: Existing knowledge and general insights.Pulmonary pharmacology & therapeutics,55, 89-94.
[3] Kafentzis, G. P., Tetsing, S., Brew, J., Jover, L., Galvosas, M., Chaccour, C., & Small, P. M. (2023). Predicting tuberculosis from real-world cough audio recordings and metadata.arXiv preprint arXiv:2307.04842.
[4] Thomas, B. E., Thiruvengadam, K., Vedhachalam, C., A, S., Rao, V. G., Vijayachari, P., … & Kaur, H. (2021). Prevalence of pulmonary tuberculosis among the tribal populations in India.PLoS One,16(6), e0251519.
[5] Wetscherek, M. T., Sadler, T. J., Lee, J. Y., Karia, S., & Babar, J. L. (2022). Active pulmonary tuberculosis: something old, something new, something borrowed, something blue.Insights into imaging,13(1), 3.
[6] O’Gurek, D., & Choi, H. Y. J. (2022). Hemoptysis: evaluation and management.American family physician,105(2), 144-151.
[7] Sammy, R. P., & Yap, Y. C. (2024). Rasmussen’s aneurysm: A pivotal cause of hemoptysis in pulmonary tuberculosis.Visual Journal of Emergency Medicine,37, 102149.
[8] Shebani, A., Hnish, M., Elmelliti, H., Abdussalam, A. L., & LAbdussalam, A. (2022). Massive hemoptysis in pulmonary tuberculosis from rasmussen pseudoaneurysm.Cureus,14(10).
[9] Rao, V. G., Bhat, J., Yadav, R., Muniyandi, M., Bhondeley, M. K., & Wares, D. F. (2015). Yield of pulmonary tuberculosis cases by symptoms: Findings from a community survey in Madhya Pradesh, central India.Indian Journal of Tuberculosis,62(2), 121-123.
[10] Farina, E., D’Amore, C., Lancella, L., Boccuzzi, E., Ciofi degli Atti, M. L., Reale, A., … & Raucci, U. (2022). Alert sign and symptoms for the early diagnosis of pulmonary tuberculosis: analysis of patients followed by a tertiary pediatric hospital.Italian Journal of Pediatrics,48(1), 90.
[11] Yang, T. Y., Lin, C. L., Yao, W. C., Lio, C. F., Chiang, W. P., Lin, K., … & Tsai, S. Y. (2022). How mycobacterium tuberculosis infection could lead to the increasing risks of chronic fatigue syndrome and the potential immunological effects: a population-based retrospective cohort study.Journal of Translational Medicine,20(1), 99.
[12] Unnewehr, M., Meyer-Oschatz, F., Friederichs, H., Windisch, W., & Schaaf, B. (2023). Clinical and imaging factors that can predict contagiousness of pulmonary tuberculosis.BMC Pulmonary Medicine,23(1), 328.
[13] Silva, D. R., Muñoz-Torrico, M., Duarte, R., Galvão, T., Bonini, E. H., Arbex, F. F., … & Mello, F. C. D. Q. (2018). Risk factors for tuberculosis: diabetes, smoking, alcohol use, and the use of other drugs.Jornal Brasileiro de Pneumologia,44(02), 145-152.
[14] Buonsenso, D., Pata, D., Visconti, E., Cirillo, G., Rosella, F., Pirronti, T., & Valentini, P. (2021). Chest CT Scan for the diagnosis of pediatric pulmonary TB: radiological findings and its diagnostic significance.Frontiers in Pediatrics,9, 583197.
[15] Huber, B., & Joshi, S. (2023). CNS tuberculoma in an immunocompetent patient: A case report of multi-drug hypersensitivity to RIPE therapy.IDCases,33, e01886.
[16] Goyal, V., Kadam, V., Narang, P., & Singh, V. (2017). Prevalence of drug-resistant pulmonary tuberculosis in India: systematic review and meta-analysis.BMC Public Health,17(1), 817.