
 is a rare congenital lung malformation characterized by the formation of a...){kind=link}

Pulmonary Sequestration Understand Pulmonary sequestration (PS) is a rare congenital lung malformation characterized by the formation of a nonfunctional mass of lung tissue. The disease arises before birth, i.e,. during fetal life (embryonic phase of development). The dysplastic lung tissue is nonfunctional and does not communicate with other structures of the lungs. In addition to the lack of communication between the sequestrum and the tracheobronchial tree, there is a lack of normal blood supply. The blood vessels that supply blood to the sequestrum are defective (anomalous). It receives blood from the systemic circulation (most commonly the thoracic or abdominal aorta) instead of the pulmonary artery, which normally supplies the lungs..
The disorder is also known as lung or bronchopulmonary sequestration and accounts for 0.15 to 6.40% of all congenital lung malformations. It is the second most common congenital anomaly of the lungs. Pulmonary sequestrations are more common in males than females, with a ratio of approximately 4:1. Typically, doctors manage sequestrations through early surgical intervention.
Pulmonary Sequestration Types: Pulmonary Sequestration Understand
Clinicians divide pulmonary sequestration into two main types:
Intralobar Pulmonary Sequestration (IPS):
IPS contributes to 75% of all pulmonary sequestration cases. In a study, intralobar pulmonary sequestration accounted for 90.7% of PS cases, while EPS was found in only 9.3% of cases.
In this variant, the sequestrum arises within the normal lung tissue. Thus, you will find it enclosed in the visceral pleura of the normal lung. However, there is no communication between the abnormal tissue and the bronchi, making it nonfunctional. It is usually diagnosed in early childhood and receives oxygenated blood from the systemic circulation, while venous drainage occurs through the pulmonary veins. Clinical reports of a 26-year-old male patient found intralobar pulmonary sequestration receiving a blood supply from the descending thoracic aorta.
IPS commonly affects the younger population who present with repeated infections. In rare instances, intralobar sequestration can be acquired secondary to chronic inflammation, bronchial obstruction, or recurrent pneumonia, though most cases are congenital.
Extralobar Pulmonary Sequestration (EPS):
This type is less common as compared to IPS. Extralobal PS is found enclosed in its own distinct pleural covering, unlike intralobal sequestration, which shares the pleural lining with healthy lung tissue. It is usually found in the lower thoracic or upper abdominal regions. Most of the extrapulmonary sequestrations are incidental findings. As per studies, 90% of ELS cases are found in the hemithorax. An EPS also has its own separate venous drainage, i.e., delivers blood frequently into the azygos or the hemiazygos vein. The sequestration receives arterial supply from systemic vessels. The majority of extralobar sequestrations (around 73%) get their arterial supply from the descending thoracic aorta.
Pulmonary Sequestration Symptoms
Infants:
It is rarely diagnosed in infants. According to experts, the following symptoms in newborns can indicate underlying sequestration:

Excessive crying in infants can be a sign of pulmonary sequestration
Crying & Feeding Difficulties
Newborn babies with PS can present with irritation and crying due to PS. In a clinical case, a 7-month-old baby presented with excessive crying. CT scans revealed the presence of a mass in the right lower chest, which turned out to be pulmonary sequestration.
Respiratory Distress
Infants may suffer from recurrent respiratory distress due to a non-functional tissue in the lungs. This can be a contributing factor to grunting and excessive crying.
Adults:
In adults, approximately half of PS cases are asymptomatic and diagnosed during routine clinical examinations. However, when present, clinicians commonly find the following symptoms in sequestration patients:
Recurrent Pneumonia
Patients suffering from intralobar sequestration often develop pneumonia repeatedly. In a case report, a 37-year-old male presented with symptoms of cough, dyspnea, and fever on multiple occasions. After detailed analysis and histopathological reports, doctors reached the diagnosis of pulmonary sequestration.
In the vast majority of cases, doctors mistake a sequestration for a respiratory infection. Therefore, several patients receive antibiotics that do no good in improving the patient’s condition. Even in pediatric patients, PS can manifest as recurrent pneumonia. So, appropriate treatment strategies like surgical lobar resection significantly alleviate symptoms.
This is why experts advise lung specialists to never rule out pulmonary sequestration without proper testing.
Recurrent Infections
Repeated respiratory infections can puzzle clinicians. As PS is a rare disorder, most healthcare professionals do not consider it in routine practice. However, the repeated exposure of patients to lung infections can even cause long-term problems. According to one study, sequestration-induced recurrent infections can have a synergistic effect (with cigarette smoking) in the development of COPD.
Patients with dysplastic lung tissues may show symptoms due to infected sequestrations. There is evidence of secondary infections arising due to underlying PS. In one case, a 21-year-old female patient had recurrent pulmonary actinomycete infection secondary to a sequestration in the right lower lung.
Persistent Cough & Hemoptysis
Numerous patients experience a persistent cough as a consequence of pulmonary sequestration. Fever may accompany these on-and-off episodes of cough. The presence of an inactive lung mass can present with recurrent infections, cough, and hemoptysis (blood in the cough).
Back Pain
Backache is not directly linked to sequestrations, but different patients have reported it in association with the lung deformity. According to a case report, a 43-year-old man suffered from left-sided back pain along with respiratory symptoms like hemoptysis, shortness of breath, chest pain, and weight loss for 2 weeks. Radiographic analysis revealed bronchopulmonary sequestration, which was treated with a left thoracotomy. Like other studies, this study also found recurrent pneumonia, hemoptysis, and chest pain associated with PS.
In unique cases, an extralobar sequestration can impact your abdomen, too. There have been reported clinical cases of concurrent back and abdominal pain (in adult patients). So, if you experience back pain along with respiratory troubles, you must consult a pulmonologist.
Exertional Dyspnea
The dysplastic tissue can interfere with the performance of your lungs, leading to a decline in function. As a result, multiple patients with PS fall prey to exertional dyspnea, which can impact their overall quality of life. Exertional dyspnea and chronic cough can persist for long periods before being diagnosed as PS. In the majority of cases, exertional dyspnea is observed with other symptoms, but it can rarely exist as an isolated symptom for a long time.
Pulmonary Sequestration Causes
The exact mechanism of pulmonary sequestration formation is not known, but experts believe that it is the result of an extra lung bud during prenatal development. In normal embryonic life, a lung bud (respiratory diverticulum) forms from the wall of the foregut. This lung bud develops into bronchial buds from which different respiratory structures form (including trachea, bronchi, and larynx, etc.).
However, in rare instances, there is the formation of an accessory bud that fails to connect with the main (normal) tracheobronchial tree. As it is disconnected from the main lung tissues, the sequestration survives by developing its own blood supply from the aorta. The disconnected lung mass is non-functional. It may or may not be encapsulated within (and connected to) the lung base, leading to the formation of intralobar or extralobar PS.
In a study, bilateral bronchopulmonary sequestration was hypothesized to originate from an extra (supernumerary) lung bud. Clinical features of the patient revealed abnormal lung tissue that formed during the intrauterine life.
Pulmonary Sequestration Diagnosis
History & Physical Examination:
The symptoms of PS are similar to different pulmonary pathologies; therefore, your healthcare provider will take a complete history of your symptoms. Recurrent pneumonia in a specific segment of the lung usually points towards this type of disorder. Doctors usually diagnose PS as an infection and advise antibiotics. However, a lack of response (or poor response) to antibiotics encourages health professionals to investigate further. So, your doctor can order radiographic imaging tests for clarity.
Radiographic Imaging:
Different imaging studies can help diagnose a pulmonary sequestration.
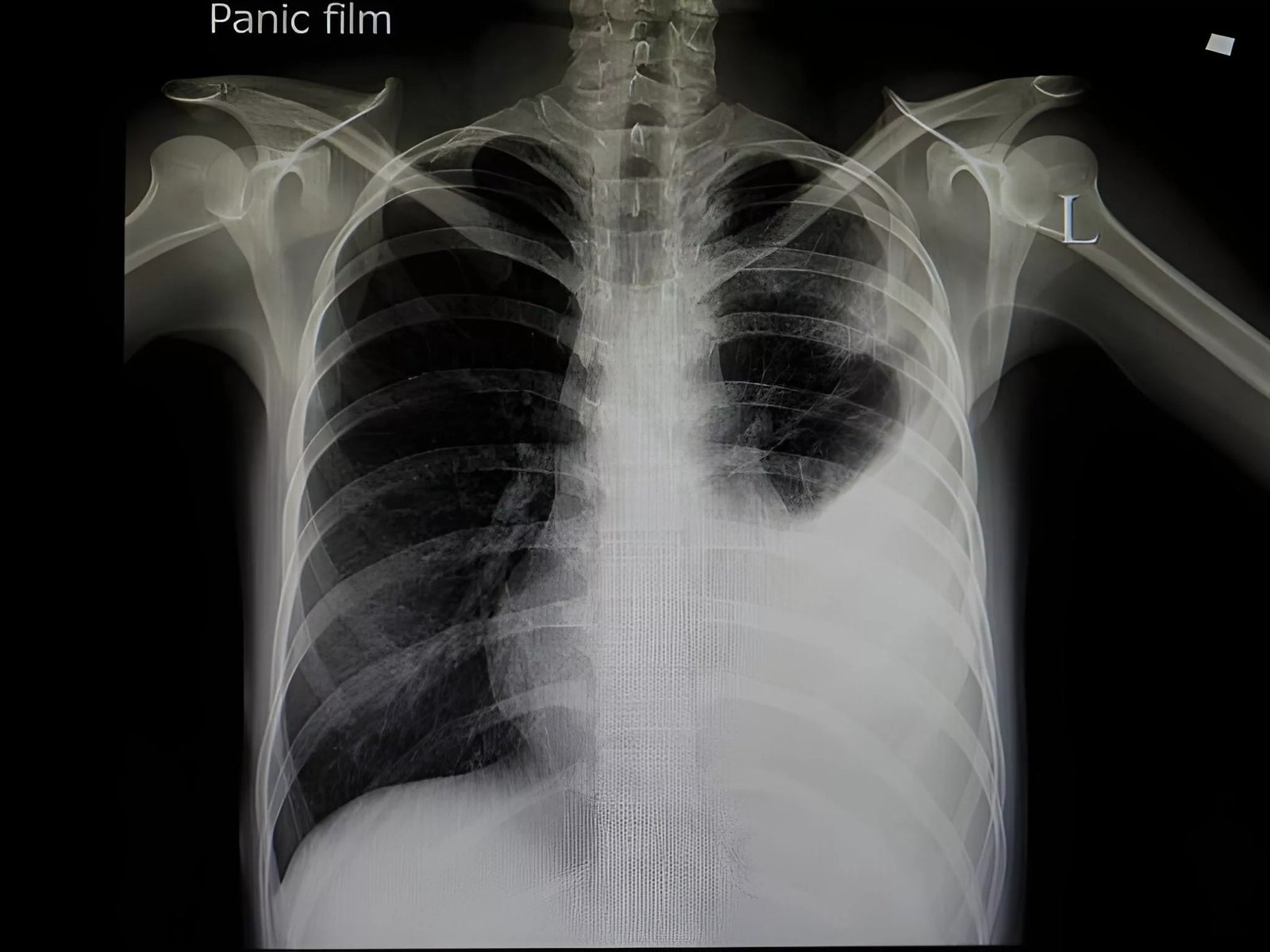
The radiograph shows pneumonia in the left lung of the patient attributed to underlying pulmonary sequestration.
Chest X-rays
Conventionally, chest X-rays have been useful in diagnosing lung pathologies. However, nowadays, doctors use more advanced imaging types such as CT scans.
CT Scans
Most diagnoses of sequestrations are incidental diagnoses on a routine computed tomography (CT) scan of the chest. A modification of the CT scan is the Computed Tomography Pulmonary Angiography (CTPA) test. In this particular test, a chest CT scan is done after injecting a special dye into the vein. This contrast dye highlights the pulmonary blood vessels, which allows diagnosis of PS. Modern studies conclude that the clinical presentations of lung sequestration are non-specific; however, CTPA plays a significant role in improving diagnostic accuracy. This is attributed to the test’s superior ability to accurately identify arteries and vessels.
Usually, doctors avoid biopsies due to the high risk of bleeding. Your healthcare provider may check your blood hormone levels (of cortisol, aldosterone) and order blood and urine tests to rule out adrenal and neurogenic tumors.
Prenatal Diagnosis:
Doctors use a Doppler ultrasound at 18-19 weeks of gestation in pregnant mothers suspected of having infants with PS. However, it isn’t a very reliable test because most of the lung masses disappear without any intervention.
Differential Diagnosis
Different diseases fall into the differential diagnosis of PS, including cystic adenomatoid malformation, bronchoectasis, pneumatoceles, and bronchogenic cysts, among others.
Pulmonary Sequestration Treatment
Infant Management:
Management of infants with intra- or extralobar pulmonary sequestration needs extensive treatment strategies. In case of large lung sequestrations, doctors provide supportive management with strategies like ventilator support and extracorporeal membrane oxygenation (ECMO). An ECMO is a type of life-support system that acts as a temporary heart-lung machine. It removes blood and returns it to the patient after adding oxygen (and removing carbon dioxide) to it.
Coil embolization is a minimally invasive procedure in which coils (made out of platinum) are used to block blood flow to the sequestrum. This blockage leads to involution of the sequestrum.
Lobectomy or segmentectomy may be necessary in large lesions or cases associated with pleural effusion.
Adult Management:
Surgery
The mainstay of lung sequestration management in adults is pulmonary lobectomy or segmentectomy. Doctors advise performing lobotomies even in asymptomatic cases to prevent progressive inflammation of the parenchyma and infection.
The illustration shows different types of lobectomies for pulmonary sequestration.
Surgeons can choose from different surgical techniques to access the lung tissues, including open thoracotomy or Video-assisted thoracoscopic procedures (VATS). Studies show that lobectomy/lobotomy is the generally adopted operative method, but techniques like wedge resection (with VATS) are safe and feasible alternatives in selected cases.
Endovascular Embolization
This very strategy reduces the blood supply to the sequestrum, leading to its necrosis, followed by fibrosis and consequent involution. Your doctor may use micro coils or embolic agents like gelatin, Amplatzer agents for this purpose. Research shows that arterial embolization is an effective therapy in sequestration treatment. It has been proven to be an effective alternative to surgery for IPS.
Pulmonary Sequestration Prognosis:
In general, extralobar sequestration has a better prognosis. Experts note that prognosis depends on factors like the presence of pulmonary hypoplasia and fetal hydrops (fluid buildup in the infant’s tissues). Only a small percentage of fetuses with large pleural effusions survive.
Complications
Timely diagnosis and treatment of PS is crucial because bronchopulmonary sequestrations are linked to multiple complications, including:
- Heart failure
- Lung cancer
- Pleural hemorrhage
{kind=link}
Wrapping Up
Pulmonary sequestration is a rare disorder involving the formation of dysplastic lung tissue during intrauterine life. Unlike the normal tracheobronchiolar tissues, this tissue (called a sequestrum) stays disconnected from the main lung tissues and has its own blood supply (from the aorta). There are two types of PS, i.e., intralobar PS, which develops within the pleura of normal lung tissue, and extralobar PS, which has its own distinct pleura.
In the vast majority of cases, the condition is asymptomatic despite being present at birth. Infants diagnosed with the disorder have serious breathing and feeding difficulties. When present, symptoms in adults include persistent unexplained cough, recurrent pneumonia, hemoptysis, repeated infections, and exertional dyspnea, etc. It arises due to the abnormal presence of a supernumerary lung bud (from the foregut) during embryonic life.
Doctors diagnose PS with radiographic imaging like chest X-rays and CT scans. CT pulmonary angiography helps accurately diagnose a sequestration by providing a detailed picture of the vessels. Health professionals provide oxygen therapy and ventilator support to serious infants with PS. In adults, the preferred mode of treatment is surgical resection, i.e., pulmonary lobotomy/lobectomy. However, endovascular embolization has also shown promising results in treating sequestrations.
References
[1] Chakraborty, R. K., Modi, P., & Sharma, S. (2023). Pulmonary sequestration. InStatPearls [Internet]. StatPearls Publishing.
[2] Ren, S., Yang, L., Xiao, Y., Tong, Z., Wang, L., & Hu, Y. (2023). Pulmonary sequestration in adult patients: a single-center retrospective study.Respiratory Research,24(1), 13.
[3] Sadasivan Nair, P., Merry, C., & White, A. (2023). Intralobar pulmonary sequestration in an adult: a case report.Journal of Cardiothoracic Surgery,18(1), 5.
[4] Liu, L., Han, P., Zhu, Y., Gong, J., Xu, Y., Wei, X., … & Wei, Q. (2012). Intra-abdominal pulmonary sequestration: a case report and literature review.Urologia Internationalis,88(1), 121-124.
[5] Li, L., Wang, Y., Sun, L., & Wang, W. (2024). A seven‐month‐old baby presenting excessive crying for pulmonary sequestration with torsion: A case report and literature review.Respirology Case Reports,12(9), e70016.
[6] Samarasinghe, L., Dharmaratna, D., Dharmaratna, K., & Inigo-Santiago, L. (2025). Recurrent Episodes of Pneumonia Leading to the Diagnosis of Pulmonary Sequestration: A Case Report.American Journal of Respiratory and Critical Care Medicine,211(Abstracts), A6762-A6762.
[7] Goswami, G., Bhatnagar, R., & Tandon, R. (2024). Recurrent Pneumonia in a Child: Identifying an Underlying Pulmonary Sequestration.Indian Pediatrics Case Reports,4(1), 36-40.
[8] Gonzalez Santiago, G. M., Fernandez, R., Mendez, O. F., Matos, E., & Torrens Olan, J. (2023). Recurrent Pneumonia: Don’t Miss a Pulmonary Sequestration. InA62. BACTERIA, FIND OUT WHAT IT MEANS TO ME(pp. A2122-A2122). American Thoracic Society.
[9] Leitner, M., Kühnle, J. L., Ecker, P., Khrystenko, T., Tränkenschuh, W., Bals, R., … & Langer, F. (2024). Untreated pulmonary sequestration with recurrent superinfection supporting COPD development in a 42 year old male patient.Multidisciplinary Respiratory Medicine,19(1), 953.
[10] Singh, R., & Duffalo, L. (2024). A Case of Infected Pulmonary Sequestration in Adulthood.Annals of Internal Medicine: Clinical Cases,3(6), e231249.
[11] Wang, Y., Ma, G., Rao, N. N., Liu, M., Liao, J., & Wang, Q. Y. (2024). Pulmonary sequestration associated with pulmonary actinomycosis: A case report and literature review.Medicine,103(40), e39981.
[12] Dang, S., & Butzko, R. (2025). A 30-Year-Old Male With Pulmonary Sequestration Presenting as a Lung Mass and Bilateral Bronchiectasis.American Journal of Respiratory and Critical Care Medicine,211(Abstracts), A7512-A7512.
[13] Petty, L., Joseph, A., & Sanchez, J. (2018). Case report: pulmonary sequestration in an adult.Radiology case reports,13(1), 21-23.
[14] Wong, B., & Culjat, R. (2018). Extralobar Pulmonary Sequestration Presenting as Abdominal Pain.Proceedings of UCLA Health,22(1).
[15] Sarkar, S., Girija, A., Shirgaonkar, R., & Mohapatra, P. R. (2024). Intralobar pulmonary sequestration.QJM: An International Journal of Medicine,117(5), 366-367.
[16] Kumar, K., Sharma, N., Rana, S., Grewal, D. S., Chaudhary, R., & Vasan, A. S. (2024). An Unusual Presentation of Pulmonary Sequestration-A Case Report.Medical Journal of Dr. DY Patil University,17(6), 1261-1263.
[17] Joseph, B., Akshaya, K. T., Nair, R. S., Raju, R. S., Mini, J., & Ravi, A. (2024). Bilateral Pulmonary Sequestration–A Rare Entity.Pulmon,26(1), 20-22.
[18] Yang, T., Wang, Z., Qiang, J., Mao, Q., Kong, S., Sun, Z., & Li, Y. (2023). Computed Tomography Imaging Features of Pulmonary Sequestration.Journal of Vascular Diseases,2(4), 367-380.
[19] Lin, Z. W., Gu, J., Xu, S. T., Ge, D., & Wang, Q. (2016). Video-assisted thoracoscopic surgery for intralobar pulmonary sequestration: Wedge resection Is feasible in limited peripheral lesions.The Thoracic and cardiovascular surgeon,64(05), 456-460.
[20] Borzelli, A., Paladini, A., Giurazza, F., Tecame, S., Giordano, F., Cavaglià, E., … & Niola, R. (2018). Successful endovascular embolization of an intralobar pulmonary sequestration.Radiology Case Reports,13(1), 125-129.
[21] Prakash, K. A., & Ramakrishnan, G. A. (2024). Intralobar pulmonary sequestration: Varied presentations and different treatment modalities.Journal of Association of Pulmonologist of Tamil Nadu,7(3), 105-107.