
, amniotic...){kind=link}

Chorioamnionitis Symptoms Management Chorioamnionitis is an infection and inflammation of the fetal membranes (chorion and amnion), amniotic fluid, and sometimes the placenta. It usually develops during labor (clinical chorioamnionitis or intraamniotic infection) but may also be identified after delivery on placental pathology (histologic chorioamnionitis). The word chorioamnionitis comes from the Greek words “chorion” and “amnion” (fetal membranes) and “-itis,” meaning inflammation. The condition can be acute or chronic, with acute infection being the typical clinical presentation. If left untreated, the condition can cause significant maternal and neonatal morbidity and mortality. Prompt diagnosis and antibiotic therapy reduce complications for both mother and infant. Chorioamnionitis is reported in around 2–5% of term deliveries and up to 40–70% of preterm deliveries, especially in association with preterm premature rupture of membranes (PPROM).
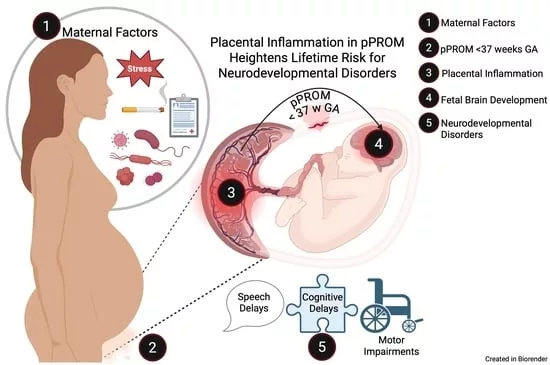
Graphical abstract of Chorioamnionitis. Image Courtesy: Placental Inflammation in Preterm Premature Rupture of Membranes and Risk of Neurodevelopmental Disorders by Cervantes et al, 2025,doi.org/10.3390/cells14130965, available via: https://www.mdpi.com/2073-4409/14/13/965, CC BY 4.0.
Causes of Chorioamnionitis: Chorioamnionitis Symptoms Management
Maternal chorioamnionitis develops when the protective mechanisms of the urogenital tract or uterus fail during pregnancy, allowing microbes to enter the amniotic cavity. It is most often an ascending bacterial infection from the vagina or cervix, but viral and fungal pathogens can also be responsible. The inflammation in utero is strongly linked with preterm birth, neonatal sepsis, retinopathy, cerebral white matter damage, and other neurodevelopmental abnormalities.
The most common bacterial agents that can cause chorioamnionitis include:
- Group B Streptococcus (GBS)
- Ureaplasma
- Mycoplasma hominis
- Gardnerella vaginalis
- Bacteroides
- Escherichia coli
Other less common pathogens include:
- Candida spp.
- Trichomonas vaginalis
Risk Factors of the Chorioamnionitis
The common risk factors for this condition include:
Rupture of Fetal Membrane:
The chorioamniotic membrane is a physical and biochemical barrier that produces antimicrobial peptides and houses innate immune cells. Premature rupture of membranes (PROM or PPROM) allows ascending microbial invasion.
Prolonged Labor:
Uterine contraction during labor increases the risk of microbial invasion in the amniotic cavity. Uterine contractions exert a suction-like effect. The vaginal fluid ascends into the uterine cavity. The longer the duration of labor after membrane rupture, the higher the infection risk.
Multiple Digital Vaginal Examinations:
Each examination increases the risk of introducing bacteria into the uterine cavity. Limiting unnecessary exams after membrane rupture reduces infection risk.
Other risk factors include: internal fetal monitoring, nulliparity, meconium-stained amniotic fluid, and sexually transmitted infections.
Pathophysiology & Histopathology
Chorioamnionitis is typically an ascending infection from the lower genital tract that reaches the amniotic cavity. Less commonly, it may occur via hematogenous spread (e.g., with Listeria infection). Histopathological findings show acute inflammatory infiltrates of neutrophils in the membranes, placenta, and umbilical cord (funisitis). The amniotic fluid may appear cloudy, purulent, or sometimes clear despite infection.

The pathogenesis and associated inflammatory cascade of chorioamnionitis.Image Courtesy: Chorioamnionitis: An Update on Diagnostic Evaluation by Carter et al, 2023,doi.org/10.3390/biomedicines11112922, available via: https://www.mdpi.com/2227-9059/11/11/2922, CC BY 4.0.
Signs & Symptoms of Chorioamnionitis
The clinical signs and symptoms of chorioamnionitis include:
- Intrapartum Fever: According to the National Institute of Child and Human Development report, maternal fever is defined as a temperature of at least 39.0 °C or a temperature between 38.0 °C and 37.9 °C without another clear source.
- Maternal leukocytosis in the absence of corticosteroids
- Fetal tachycardia (>160 bpm baseline)
- Significant maternal tachycardia
- Purulent or foul-smelling amniotic fluid or vaginal discharge
- Uterine tenderness
Diagnosis of Chorioamnionitis
Chorioamnionitis is primarily a clinical diagnosis, made on the basis of maternal signs and symptoms. However, laboratory tests and histopathology play an important role in supporting the diagnosis, ruling out mimicking conditions, and identifying infection severity.
History & Physical Examination:
The pregnant woman may appear ill, febrile, and sometimes toxic, with diaphoresis, tachycardia, and uterine tenderness. On examination, the uterus, vagina, and abdomen are carefully assessed. Most women with chorioamnionitis have ruptured membranes, but infection can occasionally occur even with intact membranes.
Important points to note in the history include:
- Maternal age
- Parity
- Gestational age
- Complications of the current pregnancy (such as premature rupture of membranes)
- Presence of meconium-stained fluid
- History or presence of sexually transmitted infections
- Recent illness
- Urinary tract infection
Diagnostic Criteria (ACOG):
According to the American College of Obstetricians and Gynecologists (ACOG), chorioamnionitis is diagnosed as follows:
- Suspected chorioamnionitis: Maternal fever ≥39°C (102.2°F) once, or 38–38.9°C (100.4–102°F) on two occasions 30 minutes apart, plus at least one of the following: maternal tachycardia, fetal tachycardia, uterine tenderness, purulent amniotic fluid, or maternal leukocytosis.
- Confirmed chorioamnionitis: Positive amniotic fluid culture or Gram stain, low glucose or elevated white blood cells in amniotic fluid, or histologic evidence of infection in the placenta or membranes.
- Isolated maternal fever: Fever without additional clinical findings still requires close monitoring and consideration of intra-amniotic infection.
Laboratory Tests:
Clinicians order blood or urine tests to check for infection or white blood cell count. A raised white blood cell count and elevated C-reactive protein (CRP) may suggest infection, although they are not specific. Vaginal cultures may identify the bacteria involved.
Amniotic fluid studies (if amniocentesis is performed) are more specific and may show:
- Low glucose levels
- High interleukin-6 (IL-6) concentrations
- Positive Gram stain or culture for microorganisms
Ultrasound may be used to check the fetus and amniotic fluid volume, but it is less specific for diagnosis.
Fetal Monitoring:
Persistent fetal tachycardia (heart rate >160 beats per minute) can be an early sign of intrauterine infection and is often used along with maternal fever to raise suspicion.
Histopathological Diagnosis:
The most definitive confirmation is made after delivery by examining the placenta and membranes. Neutrophil infiltration of the chorion and amnion is a hallmark feature. If the inflammation involves the umbilical cord, it is termed funisitis, which reflects a fetal inflammatory response. In some cases, inflammation is present without bacterial growth, known as sterile chorioamnionitis.
Differential Diagnosis
The differential diagnosis of chorioamnionitis includes:
- Urinary tract infection
- Cystitis
- Cervicitis
- Vaginitis
- Pelvic inflammatory disease
Management & Treatment of Chorioamnionitis
The management and treatment of this disease include antibiotic therapy, supportive care, and expedited delivery.
Antibiotic Therapy:
Antibiotics are the cornerstone of treatment. The recommended first-line regimen is ampicillin (2 g IV every 6 hours) combined with gentamicin (1.5 mg/kg IV every 8 hours).
In cesarean delivery, doctors recommend clindamycin (900 mg IV single dose at cord clamping) to reduce the risk of post-cesarean infections.
Other antibiotic options include:
- Carbapenems
- Cefotetan
- Cefoxitin
- Piperacillin-tazobactam
- Metronidazole
- Cefazolin
- Vancomycin
Supportive Care:
The care for mothers includes antipyretics, such as acetaminophen, for fever control. On the other hand, supportive care for the neonates includes:
- Maintenance of temperature (warmth)
- Monitoring the vitals
- Treatment of metabolic or respiratory complications
- Management of thrombocytopenia or coagulopathy
- Neonatal resuscitation, such as intubation and surfactant replacement therapy for affected neonates.
Management of Delivery:
Doctors do not delay delivery once they confirm chorioamnionitis. They usually favor vaginal delivery, since cesarean delivery increases maternal risk. They perform cesarean delivery only when obstetric or fetal indications exist. When a cesarean is necessary, they always give prophylactic antibiotics to lower the chance of postoperative infection.
Postpartum Care:
Most women recover without extended antibiotic use after delivery. If fever or infection signs persist, doctors continue antibiotics until the woman is afebrile and clinically stable.
Providers also monitor closely for complications such as endometritis, wound infection, or sepsis.
Prognosis
Chorioamnionitis is a risk factor for both neonatal and maternal sequelae. Women undergoing cesarean section or even normal deliveries can develop endometritis. Management of postpartum antibiotics can not decrease the risk of developing endometritis. However, the majority of women recover and do not require further antibiotics after delivery.
Prevention
Doctors and healthcare teams take several steps to lower the risk of chorioamnionitis during pregnancy and labor.
- They limit the number of internal vaginal examinations after the membranes rupture, since each exam increases the chance of infection.
- They start antibiotics if the membranes rupture early (preterm premature rupture of membranes) to reduce the risk of ascending infection.
- They screen pregnant women for Group B Streptococcus in the third trimester and treat carriers with intrapartum antibiotics.
- They also encourage good prenatal care, which helps identify and treat urinary tract infections, sexually transmitted infections, and other maternal risk factors early.
Effects of Chorioamnionitis on the Neonates
Chorioamnionitis has significant adverse effects on the newborn. These effects include:
- Newborns exposed to this condition have a higher risk of early-onset neonatal sepsis and pneumonia due to infection crossing to the fetus during delivery.
- It can also lead to respiratory complications such as respiratory distress syndrome.
- Gastrointestinal complications can include vomiting, diarrhea, and even seizures.
- Chorioamnionitis can often lead to preterm birth. Premature birth can be a major contributor to neonatal morbidity and mortality.
- Premature neonates face a higher risk of complications from underdeveloped organs, including necrotizing enterocolitis, intraventricular hemorrhage, impaired cerebral blood flow, and brain injury.
- Long-term outcomes can include cerebral palsy, white matter damage, developmental delays, and altered neurodevelopment.
Chorioamnionitis Versus Endometritis
Chorioamnionitis and endometritis are both infections related to the female reproductive tract. However, they occur at different times and locations with distinct clinical implications. Endometritis develops after delivery when bacteria infect the endometrial lining of the uterus. It primarily affects the mother and usually has less direct impact on the neonate. The key differences between the two medical conditions are summarized in Table 1 below.
Table 1: Difference between Chorioamnionitis and Endometritis
| Aspects | Chorioamnionitis | Endometritis |
|---|---|---|
| Time | During pregnancy | After delivery |
| Location | Infection of the fetal membrane and amniotic fluid | Infection of the endometrial lining |
| Impact on fetus | High risk of sepsis and complications | Minimal direct impact |
| Management | Supportive and antibiotic therapy, as well as delivery management. | Postpartum antibiotics and uterine evacuations in some cases. |
Final Remarks
Chorioamnionitis is a severe condition that occurs during pregnancy. In women with premature ruptured membranes, the interprofessional staff must avoid multiple digital exams. Treatment typically involves antibiotics. The fetal attack rate is low, but neonatal sepsis in patients with chorioamnionitis is a significant problem.
References
[1] Fowler JR, Simon LV: Chorioamnionitis. 2018.
[2] Maki Y, Fujisaki M, Sato Y, Sameshima H: Candida chorioamnionitis leads to preterm birth and adverse fetal‐neonatal outcome. Infectious diseases in obstetrics and gynecology. 2017, 2017:9060138.
[3] Alhomsi, S., Sawallha, L., Hakmi, M., Ibrahim, A. A., Khayoun, H., & Henna, N. (2024). Fever in Pregnancy: A Rare Case of Listeria-Induced Chorioamnionitis.Cureus,16(10), e70670. https://doi.org/10.7759/cureus.70670
[4] Kim CJ, Romero R, Chaemsaithong P, et al. “Acute chorioamnionitis and funisitis: Definition, pathologic features, and clinical significance.”American Journal of Obstetrics and Gynecology. 2015.
[5] Snyder M, Crawford P, Jamieson B: What treatment approach to intrapartum maternal fever has the best fetal outcomes? 2007.
[6] Chapman, S., & Duff, P. (1995). Incidence of Chorioamnionitis in Patients With Meconium-stained Amniotic Fluid.Infectious Diseases in Obstetrics and Gynecology,2(5), 210. https://doi.org/10.1155/S1064744995000032
[7] American College of Obstetricians and Gynecologists. (2017).Intrapartum management of intraamniotic infection: Committee Opinion No. 712.Obstetrics & Gynecology, 130(2), e95–e101. https://doi.org/10.1097/AOG.0000000000002236
[8] Clinical chorioamnionitis at term: definition, pathogenesis, microbiology, diagnosis, and treatmentJung, Eunjung et al.American Journal of Obstetrics & Gynecology, Volume 230, Issue 3, S807 – S840
[9] Conde-Agudelo A, Romero R, Jung EJ, Sánchez ÁJG: Management of clinical chorioamnionitis: an evidence-based approach. American journal of obstetrics and gynecology. 2020, 223:848-869.
[10] Conde-Agudelo A, Romero R, Jung EJ, Sánchez ÁJG: Management of clinical chorioamnionitis: an evidence-based approach. American journal of obstetrics and gynecology. 2020, 223:848-869.
[11] Shanks AL, Mehra S, Gross G, Colvin R, Harper LM, Tuuli MG: Treatment utility of postpartum antibiotics in chorioamnionitis study. American Journal of Perinatology. 2016, 33:732-737.
[12] Braun D, Bromberger P, Ho NJ, Getahun D: Low rate of perinatal sepsis in term infants of mothers with chorioamnionitis. American Journal of Perinatology. 2016, 33:143-150.
[13] Venkatesh KK, Jackson W, Hughes BL, Laughon MM, Thorp JM, Stamilio DM: Association of chorioamnionitis and its duration with neonatal morbidity and mortality. Journal of Perinatology. 2019, 39:673-682.