
{kind=link}

Pulmonary Contusion Symptoms Pulmonary bruising or pulmonary contusion is a condition of fluid/blood accumulation into the lungs (alveolar and interstitial spaces) following chest trauma, most commonly after blunt thoracic injury. It is the most prevalent lung complication that arises after chest trauma. In a study, 80.4% of individuals who suffered from blunt chest trauma developed right-sided lung contusion.
It is characterized by damage to the lung parenchyma. The condition presents with lung symptoms like shortness of breath, chest pain, and wheezing, etc. In some cases, the symptoms develop quickly after trauma (within a few hours), but in other cases, it may take days to develop. However, it should be noted that pulmonary contusion is a serious health issue that can prove to be fatal. Therefore, you must seek urgent medical evaluation after significant chest trauma.
Mechanism Of Pulmonary Contusion
Experts suggest three possible mechanisms by which a blunt force induces damage to the lung vessels. The mechanisms are as follows:
Spalling Effect:
According to this belief, the pressure wave from a trauma disrupts through the cells’ lipid membranes. This results in increased permeability of the membranes, leading to consequent leakage of fluid and blood.
Inertial Effect:
Different types of tissues (with different densities) are present in the lungs. Thus, these tissues respond differently (accelerate or decelerate at varied rates) to a pressure wave. This effect strips the lighter alveoli away from the bronchial tree (which is denser).
Implosion Effect:
The encounter of a pressure wave with air bubbles and compressed gas within the tissues creates a rebound force that overstretches and tears the tissues, leading to fluid leakage.
Staging of Pulmonary Contusion
The Lung Injury (Murray) Score is sometimes used to quantify lung damage and guide management. Although not specific to pulmonary contusion, it evaluates four variables:
- Hypoxemia (PaO₂/FiO₂ ratio)
- Atelectasis
- Lung compliance
- Positive End-Expiratory Pressure (PEEP)
Each variable is allocated a score from 0 to 4. The sum of the scores is divided by the number of examined variables. The final score interpretation is:
- 0: no injury
- 0.1-2.5: mild-to-moderate injury
- Above 2.5: severe injury, often consistent with ARDS
Pulmonary Contusion Symptoms
A pulmonary contusion is similar to a bruise on the skin, the only difference being that the blood accumulates in the lungs. Trauma-induced damage to the blood vessels causes leakage of tissue fluid and blood in the alveoli. This accumulation reduces the amount of lung surfactant, leading to alveolar edema. The ultimate result of these effects is alveolar collapse or collapse of the lung lobe (atelectasis). Suboptimal functioning of the lungs causes ventilation-perfusion mismatch and decreased lung compliance. These respiratory compromises are responsible for the majority of the symptoms.
There are multiple symptoms of pulmonary contusion. It may begin with vague symptoms like coughing or wheezing. However, the disease tends to transform into more serious complications and even death (if left untreated). Generally, symptoms of a mild injury develop gradually within the next 24-48 hours, but in severe contusions, you may start seeing breathing difficulties within hours. The most commonly reported symptoms associated with a pulmonary contusion include:
Coughing:
Increased frequency of coughing is a common presentation of respiratory disorders. Coughing is usually the initial presentation of an underlying pulmonary contusion, which the patient is unaware of. While clinical signs are not typical and are often slow to develop, doctors frequently observe coughing and breathing difficulties in several patients. In severe contusions, patients may also cough up blood, i.e, hemoptysis. This may also be accompanied by excessive production of watery mucus (which can obstruct the airways), a condition known as bronchorrhea.
Pulmonary contusion patients often present with hemoptysis.
Sometimes, coughing develops later during the progression of the disease. A 61-year-old man with a lung contusion presented to the ER with complaints of mild shortness of breath. The former smoker didn’t complain of cough initially. However, in the following days, his condition deteriorated, and his respiratory distress increased as he developed a nonproductive cough.
There have been reports of increased coughing frequency in patients with hemorrhagic pulmonary contusion secondary to blunt force trauma.
Shortness Of Breath:
A salient feature of contusion is shortness of breath. The accumulation of blood and fluid in the lungs reduces their capacity to expand and fill them with oxygen. Moreover, it impedes the normal gaseous exchange of the lungs. Both these effects lead to shortness of breath. Most patients notice just a mild issue in the beginning, which can worsen over time. Studies show that hypoxemia (low oxygen levels in blood) is detected in patients suffering from mild-to-moderate pulmonary contusions. The drop in oxygen levels worsened until intubation.
Rib fractures in severe trauma cases further aggravate symptoms. Cases with pulmonary contusion with rib fractures have a higher mortality rate. Due to the breathing difficulties, patients suffering from contusions require ventilation support and intensive care.
Acute respiratory distress syndrome (ARDS) is commonly seen in patients with lung contusions. Patients encountering ARDS develop dyspnea (shortness of breath) with shallow breathing.
Chest Pain:
Blunt thoracic trauma to the chest can inflict pain in patients. Usually, there is pain associated with breathing. This chest pain on breathing can also lead to fear of breathing and, consequently, more hypoventilation.
An 8-year-old girl presented to the ER with chest pain and worsening shortness of breath, 72 hours after sustaining blunt trauma to the chest in a car collision. Radiological findings confirmed the diagnosis of a lung contusion. However, severe pain is mostly seen in cases with rib fractures with contusion (especially in pediatric patients).
According to a study, chest pain after a blunt chest trauma is linked to serious consequences like contusion, hemothorax, pneumothorax, etc. Pain associated with these conditions predisposes the patient to respiratory failure.
Tachycardia:
You may also find an increased heart rate in a patient with a lung contusion. Lung bruises obtained from blunt chest trauma impair the normal gaseous exchange of the body, which can contribute to a compensatory increase in the beating rate. The heart tries to compensate for the reduced oxygen levels (and the respiratory distress) by beating faster.
In severe cases, you might find cardiorespiratory decompensation, which is characterized by hypotension, bradycardia, and apnea. It is a critical condition in which there is a suboptimal performance of the heart and the lungs, leading to worsening of symptoms. Cardiorespiratory decompensation requires emergency medical care.
Chest Bruising:
Lung contusion can be seen as bruising on the chest skin. The accumulation of blood can become visible soon after the injury/trauma or may take a few days to develop. In a clinical study, a 17-year-old male athlete suffered from pulmonary contusion following a rubber ball injury while playing Lacrosse. The young athlete presented to the ER with local bruising, hemoptysis, and shortness of breath.
Pulmonary Contusion Causes

Blunt force trauma sustained during a car accident contributes to pulmonary contusion.
Blunt Force Trauma:
It is the most common cause of a pulmonary contusion. When a dull object (unable to penetrate) hits you, it is called a blunt force injury/trauma. Examples of blunt force trauma include:
- Car accidents (motor vehicle accident)
- Falls
- Sports injuries (contact with the ball, etc.)
- Physical violence/assault
Reports suggest that lung injuries are one of the most common types of injuries sustained during a car accident. Impact with the steering wheel or dashboard, resulting from rapid deceleration, can contribute to lung contusion and other injuries. Among the thoracic injuries sustained by car accidents, 88.7% were lung contusions.
A significant force impact is needed to cause a lung contusion. However, in older adults, even minor chest trauma can lead to lung bruising.
Penetrating Injury:
A pulmonary contusion can also be the outcome of a penetrating injury. This type of injury is sustained from an object that can penetrate through your skin and tissues. The most common examples of penetrating injuries include:
- Gunshot wounds
- Stab wounds (from a knife or sharp objects)
- Blast fragments from explosions
- Animal bites
- Accidents with sharp tools (in industries, factories, etc)
Studies show that gunshot wounds directed at the chest can induce lung contusions in patients along with other respiratory complications (like pneumothorax). However, injury from sharp objects (like blast shrapnel) causes contusions when they are not capable of penetrating the lung tissue and damage the blood vessels of the alveoli in the lungs. This breach of pulmonary vessels leads to the accumulation of fluid and blood into the interstitial and alveolar spaces.
Pulmonary Contusion Risk Groups:
Certain people have an increased risk of falling prey to pulmonary contusion.
- Older adults are prone to falling, and even minor trauma can induce a contusion.
- Children have a greater propensity to develop lung bruises.
- Sportspersons/players involved in games that have a chance of trauma to the chest (football, etc.)
- Military personnel are at a greater risk of pulmonary contusion due to blast injuries, as was seen in World War soldiers.
Pulmonary Contusion Diagnosis
Healthcare providers take a thorough history of the patient regarding the onset of the respiratory symptoms (like chest pain, hemoptysis, and breathing difficulties). This is paired with a thorough physical examination, as it can reveal bruising. They might ask you questions about any recent trauma to the chest. However, in severe contusion cases, patients are brought in an apneic and unresponsive state. In such conditions, the top priority of the doctors is to resuscitate the patient and carry out a secondary survey after the patient has been stabilized.
Radiographic Imaging:
Chest X-Ray
Your doctor may use different imaging techniques to reach a confirmed diagnosis. The most commonly used diagnostic imaging technique for a lung contusion is chest X-rays. Clinical evidence suggests that chest X-rays are accurate in detecting blunt chest trauma. Therefore, they are the first choice of diagnostic imaging in hemodynamically stable patients. A careful analysis of the X-rays is important because signs usually don’t appear immediately after the injury. It might take 6-48 hours for the signs to appear on radiographs.
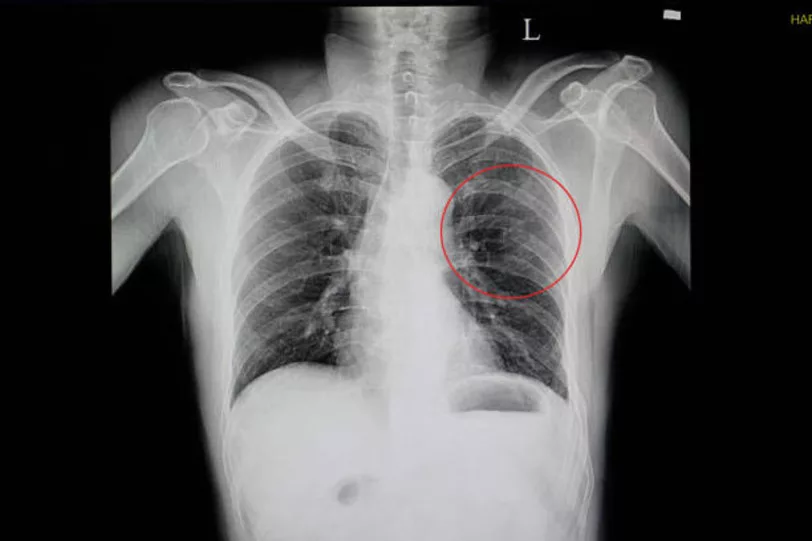
The X-ray of a patient shows pulmonary contusion with multiple rib fractures.
CT Scan
The most sensitive test in detecting a pulmonary contusion is the Computed Tomography (CT) scan. The higher resolution of a CT scan allows doctors to detect a contusion immediately after the trauma. The 3-dimensional scan of the lungs also enables health professionals to identify individuals with a high risk of ARDS.
Ultrasound
For a quick diagnosis, doctors rely on a chest ultrasound. It is a vital bedside imaging tool that helps in identifying pulmonary contusions. Doctors usually employ an ultrasound when a chest X-ray or CT scan can not be taken.
In severe contusions, doctors also advise an Electrocardiography (ECG) test to rule out cardiac contusion, which is a rapidly fatal condition.
Differential Diagnosis:
Pulmonary Contusion Vs Hemothorax
Both conditions denote accumulation of blood in the lungs and usually are outcomes of direct trauma. However, pulmonary contusion is characterized by bleeding in the alveoli, leading to impaired gaseous exchange, while hemothorax causes bleeding outside the lung (pleural space of the lungs). Symptoms are similar for a hemothorax and contusion, but unlike contusion, no hemoptysis is generally seen in a hemothorax. Doctors identify blood collection in spaces between the chest wall and the lungs in hemothorax. On the other hand, alveolar edema is present on chest X-rays in a lung contusion.
Pulmonary Contusion Treatment
Symptomatic Management:
There is no exact treatment for a pulmonary contusion. For minor cases, doctors provide supportive care only and let the body heal itself. As in most cases, symptoms develop after some time, doctors will keep you under monitoring in a hospital until they are sure of your stability. In symptomatic management, pain medications curb chest pain. Moreover, diuretics may be used in select cases to lower pulmonary capillary hydrostatic pressure and minimize fluid buildup.
Supportive Care:
Prone Positioning
Healthcare providers also use prone positioning to reduce the pressure on your diaphragm. In this technique, the patient is lying face down (on their stomach). The head is turned to the side. Clinical studies show that prone positioning can quickly correct hypoxemia and reduce atelectasis in patients with moderate-to-severe ARDS induced by pulmonary contusion. This step also potentially reduces mechanical ventilation time and the length of ICU stay. The mortality rate also reduces with prone positioning.
Mechanical Ventilation
Ventilation is essential to keep your alveoli patent and avoid physical damage to tissues, i.e., barotrauma. Non-invasive ventilation (without intubation) is effective for patients with mild-to-moderate contusion. Continuous positive airway pressure (CPAP) and Bilevel positive airway pressure (BiPAP) are effective in alleviating breathing difficulties. Invasive ventilation with mouth/neck intubation (tracheostomy) is indicated in severe cases where PAP fails.
Oxygen therapy combined with positive pressure ventilation enhances perfusion and helps redistribute fluids within the lungs, as direct drainage techniques like thoracocentesis cannot remove fluid trapped inside lung tissue.
Surgical Intervention
Surgery is generally reserved for patients with multiple rib fractures or severe chest wall instability. Stabilizing the ribs and restoring normal chest mechanics can improve lung function and reduce respiratory distress.
Pulmonary Contusion Recovery Time:
It has a mortality rate of 14-40%, depending on the severity of contusion and associated injuries. However, with good supportive care, most lung contusion patients heal within a week (5-7 days).
Pulmonary Contusion Complications
- Penumonia
- Hypoxia
- Hypercapnia (high levels of carbon dioxide in the body)
- Acute Respiratory Distress Syndrome
Final Word
A pulmonary contusion is a bruise of the lungs that causes leakage of fluid and blood into the alveoli. It is usually the outcome of blunt force trauma, like car accidents or sports injuries. It may also develop as a response to penetrating injuries like gunshot wounds and explosions. In mild cases, symptoms take around 48 hours to appear, while in severe contusions, symptoms are seen within a few hours. The disorder presents with shortness of breath (with wheeze), coughing, hemoptysis, and tachycardia.
Doctors diagnose it with physical examination, history, and radiographic imaging (X-rays, CT scans, ultrasounds). There is no exact treatment for pulmonary contusions, but healthcare professionals provide symptomatic management and supportive care, which includes analgesics, diuretics, prone positioning, oxygen therapy, and mechanical ventilation etc. Non-invasive ventilation (CPAP and BiPAP) is used in mild-to-moderate contusions, while invasive ventilation (with intubation) is the mode of choice in unconscious severe patients. Surgical intervention is opted for when there are multiple rib fractures with a contusion.
References
[1] Mardani, P., Moayedi Rad, M., Paydar, S., Amirian, A., Shahriarirad, R., Erfani, A., & Ranjbar, K. (2021). Evaluation of lung contusion, associated injuries, and outcome in a major trauma center in Shiraz, Southern Iran.Emergency medicine international,2021(1), 3789132.
[2] Rendeki, S., & Molnár, T. F. (2019). Pulmonary contusion.Journal of thoracic disease,11(Suppl 2), S141.
[3] Castrillón, A. I., Sua, L. F., Sanchez, A., & Fernández-Trujillo, L. (2024). Pulmonary Contusion—An Unusual Clinical and Radiological Presentation: Case Report.Journal of Investigative Medicine High Impact Case Reports,12, 23247096241266089.
[4] Ziebell, C., & Kravitz, L. (2018). Hemorrhagic pulmonary contusion secondary to blunt force trauma in a professional hockey player.Family Medicine and Care,1(02), 1-3.
[5] Zingg, S. W., Gomaa, D., Blakeman, T. C., Rodriquez, D., Salvator, A., Goodman, M. D., & Janowak, C. F. (2022). Oxygenation and respiratory system compliance associated with pulmonary contusion.Respiratory Care,67(9), 1100-1108.
[6] Miller, C., Stolarski, A., Ata, A., Pfaff, A., Nadendla, P., Owens, K., … & Tafen, M. (2019). Impact of blunt pulmonary contusion in polytrauma patients with rib fractures.The American Journal of Surgery,218(1), 51-55.
[7] Lee, N. H., Kim, S. H., Seo, S. H., Kim, B. J., Lee, C. S., Kim, G. H., … & Kim, J. H. (2023). Prediction of respiratory complications by quantifying lung contusion volume using chest computed tomography in patients with chest trauma.Scientific Reports,13(1), 6387.
[8] Dogrul, B. N., Kiliccalan, I., Asci, E. S., & Peker, S. C. (2020). Blunt trauma related chest wall and pulmonary injuries: An overview.Chinese journal of traumatology,23(03), 125-138.
[9] Berland, M., Oger, M., Cauchois, E., Retornaz, K., Arnoux, V., & Dubus, J. C. (2018). Pulmonary contusion after bumper car collision: case report and review of the literature.Respiratory medicine case reports,25, 293-295.
[10] Lovisari, F., Favarato, M., Giovannini, I., Giudici, R., & Fumagalli, R. (2020). Chest wall pain management after chest wall trauma.Journal of Visualized Surgery,6.
[11] Marin, E. F., Ozair, A., DeRosimo, J., Candela, J., & McDermott, M. W. (2024). Pulmonary contusion with hemoptysis from lacrosse ball strike: A case report.Heliyon,10(12).
[12] Benhamed, A., Ndiaye, A., Emond, M., Lieutaud, T., Boucher, V., Gossiome, A., … & Tazarourte, K. (2022). Road traffic accident-related thoracic trauma: Epidemiology, injury pattern, outcome, and impact on mortality—A multicenter observational study.PLoS one,17(5), e0268202.
[13] Ogbudu, S. O., Eze, N. J., Nwagboso, C. I., Echieh, C. P., Etiuma, A. U., & Bassey, O. O. (2023). Bilateral Chest Injury in A Single Gunshot Injury; Right Pleural Breach with An Open Pneumothorax and A Cavitatory Chest Wall Wound from An Ak-47.American Journal of Clinical Case Reports,1(1081), 032-033.
[14] Rollins, R., Altman, J., Diemer, K., Smith, A., Clugston, J. R., Silvestri, P., … & Chrabaszcz, S. (2025). Pulmonary Contusions in a Collegiate Football Player With Same-Game Return-to-Play.Cureus,17(2).
[15] Rendeki, S., & Molnár, T. F. (2019). Pulmonary contusion.Journal of thoracic disease,11(Suppl 2), S141.
[16] Agladioglu, K., Serinken, M., Dal, O., Beydilli, H., Eken, C., & Karcioglu, O. (2016). Chest X-rays in detecting injuries caused by blunt trauma.World journal of emergency medicine,7(1), 55.
[17] Liu, X., Liu, H., Liu, S., Zhou, W., Lan, Q., Duan, J., … & Zheng, X. (2022). Effects of prone positioning for patients with acute respiratory distress syndrome caused by pulmonary contusion: a single‐center retrospective study.Canadian Respiratory Journal,2022(1), 4579030.