
 is a rare but progressive neurological condition in which iron is deposited on the...){kind=link}

Superficial Siderosis (SS) is a rare but progressive neurological condition in which iron is deposited on the surfaces of the brain and spinal cord due to blood leakage into the cerebrospinal fluid (CSF).
This excessive free iron starts damaging the brain, spinal cord, and cranial nerves, resulting in symptoms like hearing loss, difficulty in swallowing, unsteady gait, muscle stiffness, and overactive reflexes. For the timely diagnosis and treatment, it is important to understand the pathophysiology and differential diagnosis of superficial siderosis.
Pathophysiology: How Superficial Siderosis Occurs?
Our brain and spinal cord are protected by three layers called meninges. The space between the innermost two coverings is referred to as the subarachnoid space, in which continuous and slow bleeding causes the iron buildup.
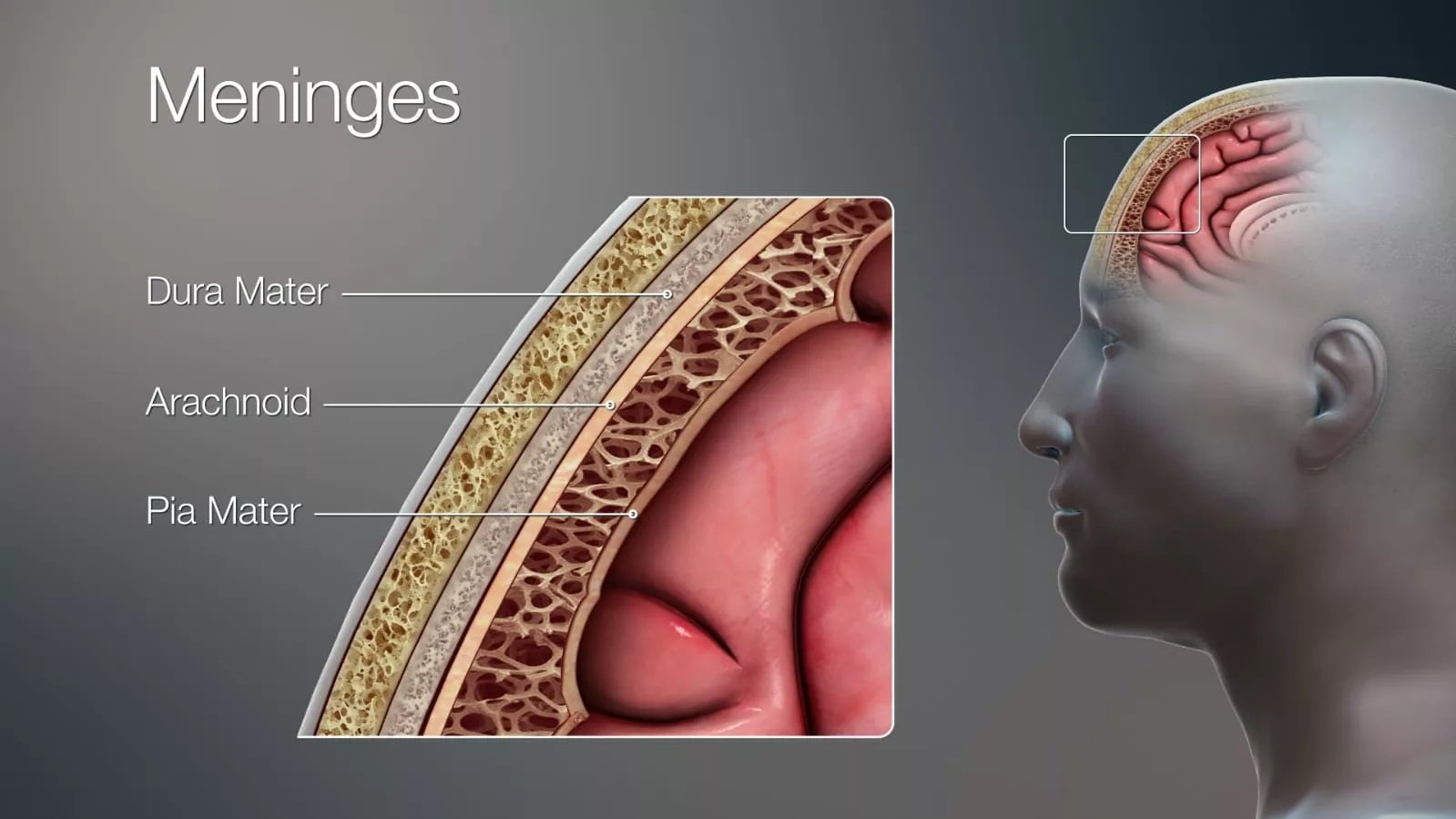
Image courtesy: 3D Medical Illustration Meninges by Ajokley, licensed under Creative Commons Attribution 4.0 International (CC BY 4.0) and Creative Commons Attribution‑ShareAlike 4.0 International (CC BY‑SA 4.0). Source: Wikimedia Commons – 3D Medical Illustration Meninges Details
Common sources of this slow bleeding into the subarachnoid space can be:
- Tumors
- Tears in the dural covering of spinal cord
- Vascular malformations (such as arteriovenous malformations or cavernous angiomas)
- Prior surgery
- Traumatic subarachnoid hemorrhage

Gross pathology of subarachnoid hemorrhage by Mikael Häggström, M.D., public domain. Source: Wikimedia Commons – Gross pathology of subarachnoid hemorrhage
Breakdown of Red Blood Cells (RBCs):
The enzymes present in the CSF in the subarachnoid space start breaking down the RBCs, extracting their iron from the cells. Normally, our brain and spinal cord clear the breakdown products of blood, but when the bleeding continues, the clearing system is overwhelmed.
- Ferritin, an iron-storing protein, becomes saturated with this excessive iron. When its storage capacity is exceeded, the excess iron precipitates and combines with proteins to form hemosiderin.
- Hemosiderin is less soluble and tends to deposit in tissues, especially along the brain and spinal cord surfaces.
These are the iron deposits that are visible on the iron-sensitive MRI sequences.
Oxidative Stress Due to Iron:
Although the hemosiderin contains the iron in the bound form, over time, free iron is released from it. This free iron speeds up the normal chemical reactions occurring in the brain to produce reactive oxygen species (ROSs).
ROSs are the main culprits that damage the lipids, proteins, and DNA, causing nerve cell death and the removal of the myelin sheath. This iron-dependent form of nerve cell death is called ferroptosis.
Why SS Affects the 8th Cranial Nerve & Cerebellum?
Clinical and imaging studies have shown that SS typically damages the 8th cranial nerve (vestibulocochlear nerve) and the cerebellum, which control balance and coordination.
- CSF Flow & Gravity: Due to gravity, CSF pools down the breakdown products of blood at the dependent parts of the brain, like the cerebellum and brainstem surfaces. That’s why these parts are affected severely.
- Cerebellum cell susceptibility: The cerebellum cells are more sensitive to iron toxicity due to their high metabolic activity and weaker antioxidant defense, which fails to clear out the ROSs.
- Long CSF exposure of the 8th cranial nerve: The 8th nerve has a long path that is bathed by CSF before it enters the ear. That long contact area increases the chance that iron will coat and damage the nerve root, which explains the early and frequent hearing loss in SS.
Patterns of Superficial Siderosis
Superficial siderosis presents with two different patterns based on where the hemosiderin deposits in the brain. The differences between these two patterns are discussed below.
| Feature | Infratentorial Superficial Siderosis (iSS) | Cortical Superficial Siderosis (cSS) |
|---|---|---|
| Main location of iron deposits | Brainstem, cerebellum, cranial nerve roots, spinal cord | Outer surface (cortex) of the brain |
| Typical cause | Chronic slow bleeding, often from spinal dural defects, trauma, or surgery | Small repeated bleeds from fragile vessels, usually due to cerebral amyloid angiopathy (CAA).5Charidimou, A., Linn, J., Vernooij, M. W., Opherk, C., Akoudad, S., Baron, J. C., Greenberg, S. M., Jäger, H. R., & Werring, D. J. (2015). Cortical superficial siderosis: detection and clinical significance in cerebral amyloid angiopathy and related conditions. Brain: a journal of neurology, 138(Pt 8), 2126–2139. https://doi.org/10.1093/brain/awv162 |
| Common age group | Middle-aged adults | Older adults (60+) |
| The most common first symptom | Progressive hearing loss in both ears | Short, repeated sensory or motor episodes |
| Other key symptoms | Imbalance, slurred speech, and muscle stiffness | Seizures, headaches, and gradual memory/thinking changes |
| Why symptoms happen | Iron damages hearing & balance nerves, cerebellum, and spinal cord tracts | Iron from surface bleeds irritates and injures the cortex |
| Progression | Slow, over the years | Episodes can start suddenly; risk of bigger brain bleeds |
| MRI clues | Dark rim along cerebellum/brainstem/spinal cord | Dark rim along the outer brain surface |
| Treatment focus | Repair bleeding source, consider iron chelation, and rehab | Control risk factors, prevent seizures, and monitor for bleeds |
How common is Superficial Siderosis?
SS is rare in the general population. Population studies using MRI have found it in only a few dozen per 100,000 people. The Mayo Clinic population study stated that 0.21% of the cases of SS occurred in individuals aged 50-69, while 1.43% of those over 69.
The cases of SS are rising day by day because of improved MRI scans. Most people are diagnosed with SS incidentally during brain scans done for another reason.
Symptoms of Superficial Siderosis
Superficial siderosis presents with diverse symptoms depending upon the part of the brain damaged by the iron toxicity. The classical triad of this condition includes progressive sensorineural hearing loss, cerebellar ataxia, and myelopathy, though not all patients present with all three.
- Progressive hearing loss: It is usually common in SS due to 8th cranial nerve damage.
- Balance & coordination problems: Iron toxicity mainly affects the cerebellum, resulting in an unsteady gait and progressive difficulty with coordination and fine movements.
- Loss of smell: Some patients experience the loss of smell because the smell-controlling region of the brain lies immediately beneath the meninges.
- Speech & Swallowing problems: Brainstem, the part of the brain that connects the spinal cord to other parts of the brain, is affected mostly by the accumulation of hemosiderin, resulting in swallowing difficulty and late-stage speech problems.
- Muscle stiffness & Overactive reflexes: When SS involves the spinal cord, it causes increased muscle tone with exaggerated reflexes.
- Bladder changes: Patients with SS may experience a sudden, strong urge to urinate, incomplete bladder emptying, difficulty starting urination, or, in some cases, urinary retention.
- Headache & Seizures: Cortical superficial siderosis, brain tissue irritation triggers the abnormal electrical activities, lowering the seizure threshold, resulting in seizures.
- Cognitive and behavioral changes: In some patients, hemosiderin buildup in cortical areas can lead to memory problems, slowed thinking, difficulty concentrating, or subtle personality changes.
- Vision problems: If iron deposition involves pathways related to vision, patients may experience double vision, blurred vision, or eye movement abnormalities.
- Chronic fatigue: Many individuals with SS report persistent fatigue, likely related to the progressive neurological decline and the brain’s reduced efficiency in processing signals.
Symptoms in SS usually appear slowly over the years iron builds up gradually.
How is Superficial Siderosis diagnosed?
Diagnosis of superficial siderosis begins with a detailed history and clinical examination. Patients often present with slowly progressive neurological symptoms, most notably the classical triad of bilateral sensorineural hearing loss, gait ataxia, and pyramidal tract involvement. Pyramidal signs may appear as muscle stiffness, exaggerated reflexes, or weakness due to dysfunction of the corticospinal tract. Careful recognition of these findings can raise clinical suspicion before imaging is performed. After the symptoms that suggest the SS, doctors usually use high-resolution MRI with blood or iron-sensitive sequences to observe carefully the characteristic superficial hemosiderin staining in the subarachnoid space
Imaging:
Standard MRIs may miss the very small coating of iron on the surfaces of the brain and spinal cord. So, healthcare professionals use specialized MRIs, like susceptibility-weighted imaging (SWI), or T2 star gradient recalled echo (T2* GRE) sequences. These MRIs even detect the very thin and dark iron stains.

The coronal (a) and parasagittal (b) T2-ponderation MRI. Image courtesy: Image by Kumar, N., licensed under Creative Commons Attribution 3.0 Unported (CC BY 3.0). Source: PMC – Superficial Siderosis: Associations and Therapeutic Implications.
Looking for the Bleeding Source:
Once the MRI confirms the iron coating on the pia mater surfaces, the next step is to find the source of bleeding.
- Doctors use the computed tomography (CT) myelography, in which the contrast dye is first injected into the CSF through lumbar puncture and is tracked. If there is any dural tear or leakage, the dye pinpoints it, helping the doctors to repair it.
- In some cases, healthcare professionals prefer a more advanced version, Dynamic CT myelography, which takes images in real time as the contrast dye moves in the subarachnoid space. It increases the chances of spotting very small leaks.
Spinal Fluid Test:
It involves the lumbar puncture or spinal tap to extract a small quantity of CSF to analyze it. Although a spinal fluid test is not always necessary, it still provides some useful clues in the diagnosis of SS.
- In some cases, CSF shows a yellowish tint (xanthochromia) indicating active bleeding.
- Further studies of CSF in the laboratory may show increased protein and hemosiderin in the CSF, confirming the superficial siderosis.
Hearing & Balance Tests:
The 8th cranial nerve damage and unsteady gait are among the earliest symptoms appearing in superficial siderosis. After appearing these symptoms, it is important to rule out the SS.
- Doctors use pure tone audiometry to measure the hearing threshold at different frequencies.
- Vestibular testing, including the video-nystagmography and rotatory chair testing, reveals the nerve functioning in the balancing of the body.
- Speech discrimination tests are also done to evaluate how well a patient understands spoken words.
These tests help monitor the disease progression and treatment response.
Differential Diagnosis of Superficial Siderosis
SS diagnosis becomes challenging sometimes for doctors because its symptoms are confusing, which overlap with many other neurological disorders.
- Neurodegenerative Disorders: They present with similar symptoms to SS, like progressive imbalance, hearing, and speech problems. However, MRI can distinguish it from SS because SS shows iron deposits on the brain’s surface.
- Motor Neuron Disease: Amyotrophic lateral sclerosis (ALS) is a disease that shows the symptoms of muscle rigidity and imbalance. But SS has characteristics iron rim appearance in a detailed MRI study.
- Cortical Vein Thrombosis (CVT): In CVT, the patients experience seizures like cSS. But MRI of CVT displays a dark, tube-like shape along the venous path, and the veins light up with contrast dye.
- Post-Surgical or Trauma-Related Iron Deposition: Treatment sites, old surgical places, tumors, or aneurysms (dilated veins) have the same appearance as SS. Even in the history of brain surgery, trauma years earlier can mislead the doctors. Specialized MRIs are useful to rule out the cause.
The summary of the diseases that mimic SS is:
| Condition | Why It Can Look Like SS | How to Tell the Difference |
|---|---|---|
| Spinocerebellar ataxia | Hearing loss, motor symptoms | No iron “black rim” on MRI |
| Motor neuron disease (ALS) | Weakness, spasticity, gait problems | ALS does not show iron deposits on MRI |
| Cortical vein thrombosis | Seizures, focal neurological episodes | CVT highlights a dark, tube-like shape along the venous path on MRI |
| Mineral or melanin deposits | Dark signals on MRI resembling iron | The distribution pattern and lack of clinical progression differ |
| Prior surgery or trauma | Similar MRI findings from an old hemorrhage | Clinical history and focused imaging reveal a true SS pattern |
| CSF leak causing hypotension | CSF leak symptoms and potential iron deposition | Dynamic CT myelography reveals a leak; the MRI pattern differs |
Management & Treatment options for Superficial Siderosis
Management and treatment of superficial siderosis involves the clearance of already deposited iron and blocking the source of bleeding.
Detection of Bleeding Source:
Once the superficial siderosis is diagnosed, the doctors focus on the detection of the source of blood leakage. Using the CT myelography, healthcare professionals identify the minor rupture in the meninges and surgically repair it.
It stops the progression of disease by halting the new iron accumulation in the subarachnoid space. Some patients show partial improvements in symptoms after the tear repair.
Iron Chelation:
In this method, your doctor uses the drugs that chemically bind to the already present iron on the brain and spinal cord surfaces to reduce the iron toxicity.
Deferiprone is the most prescribed iron chelating drug, which crosses the blood-brain barrier, a protective layer around the brain and spinal cord that usually stops the harmful chemicals from entering.
Many observational studies have shown that deferiprone stabilizes or modestly improves the symptoms after taking deferiprone. But the drug has its own some side effects, like a decrease in the white blood cells, the infection-fighting cells.
Multidisciplinary Approach:
Unfortunately, superficial siderosis is diagnosed after the irreversible damage has been done to the brain tissues and nerves, affecting different organs.
So, in these cases, the multidisciplinary approach is preferred, in which different specialists are coordinated for the supportive measures of the patient.
- Neurologist: The neurologist usually leads the care team by diagnosing and explaining the disease and treatment to other members of the team.
- ENT Specialist: You may need immediate treatment of hearing loss, though these measures have limited benefits due to permanent nerve damage.
- Urologist: Antispastic drugs, bladder training, and intermittent catheterization for emptying the bladder are beneficial in patients suffering from bladder problems.
- Physiotherapist: As muscle weakness and gait problems are common in SS, a physiotherapist helps patients with different exercises to improve stability, strengthen muscles, and prevent falls.
- Psychologist or Psychiatrist: As SS leads to permanent disability, healthcare professionals also recommend psychological support and counselling.
Other Medical Options:
Some reports have shown that steroids and anti-inflammatory drugs provide short-term relief, but these drugs have only limited temporary benefits.
Prognosis & Life Expectancy of Superficial Siderosis
Usually, repairing the bleeding source stabilizes or improves the symptoms in the patients. But if the bleeding continues, iron keeps accumulating, and the damage progresses.
The nerves have limited recovery. Although deferiprone reduces the iron deposition, improvements are variable and have some risks, too.
Superficial siderosis does not shorten life expectancy; it actually affects the quality of life, causing the patient to live with disability. Cortical SS, which is linked with cerebral amyloid angiopathy, is a life-threatening pattern that has a future risk of lobar intracerebral hemorrhage, the bleeding inside the brain.
How to prevent Superficial Siderosis?
Unfortunately, no medicine or drug prevents you from having superficial siderosis. The only prevention is to find out the causes that may lead to SS.
- If you already have vascular problems like an aneurysm or arteriovenous malformations, seek early treatment.
- If the patients have a prior history of brain or spinal surgery or trauma to these areas, regular check-ups and MRI scans are important to detect bleeding or leakage early in the subarachnoid space.
- High blood pressure and blood-thinning drugs like anti-coagulants and anti-platelets are risk factors for the SS. Control your blood pressure and take the blood-thinning drugs only when necessary.
- Cerebral amyloid angiography (CAA) increases the risk of cortical SS. If you have already been diagnosed with CAA, you should need regular MRIs.
Monitoring & Follow-Up of Superficial Siderosis
Once you are diagnosed with SS, keeping a close observation of the condition is important for the treatment.
- You need regular MRIs to see the improvements in treatment or new bleeding.
- If you are taking deferiprone, do weekly to fortnightly blood tests to note a drop in WBCs. If the WBCs are decreasing below the normal level, stop taking deferiprone.
- After surgical repair of the dural defect or bleeding source, follow-up visits are conducted to see whether the wound healing is proper.
As SS affects hearing, balance, or even bladder control, you may need ongoing assessment by different specialists.
Conclusion
Superficial siderosis (SS) results from the continuous minor bleeding over months to years into the CSF. The enzymes in the CSF break down the blood cells to extract the iron from them, which starts to deposit on the surfaces of the brain and spinal cord.
The excessive iron gets involved in the chemical reactions to produce ROSs, which are very toxic to brain tissues. Symptoms in the SS depend on the parts of the brain that the ROSs damage. Once the symptoms appear, specialized MRIs are used to detect the iron deposits on the brain and spinal cord surfaces. Unfortunately, the nerves that get damaged can’t be fully restored.
References
[1] S, Das JM, Thorell W. Intracranial Hemorrhage. [Updated 2024 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470242/
[2] Hoskin J, Kaneko K, Munakomi S, et al. Superficial Siderosis. [Updated 2024 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603744/
[3] David, S., Ryan, F., Jhelum, P., & Kroner, A. (2023). Ferroptosis in Neurological Disease. The Neuroscientist: a review journal bringing neurobiology, neurology and psychiatry, 29(5), 591–615. https://doi.org/10.1177/10738584221100183
[4] Miwa, T., Minoda, R., & Matsuyoshi, H. (2013). Vestibular function in superficial siderosis. BMC Ear, Nose, and Throat Disorders, 13, 5. https://doi.org/10.1186/1472-6815-13-5
[5] Charidimou, A., Linn, J., Vernooij, M. W., Opherk, C., Akoudad, S., Baron, J. C., Greenberg, S. M., Jäger, H. R., & Werring, D. J. (2015). Cortical superficial siderosis: detection and clinical significance in cerebral amyloid angiopathy and related conditions. Brain: a journal of neurology, 138(Pt 8), 2126–2139. https://doi.org/10.1093/brain/awv162
[6] Hoskin J, Kaneko K, Munakomi S, et al. Superficial Siderosis. [Updated 2024 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603744/
[7] Haacke, E. M., Xu, Y., Cheng, Y. C., & Reichenbach, J. R. (2004). Susceptibility weighted imaging (SWI). Magnetic resonance in medicine, 52(3), 612–618. https://doi.org/10.1002/mrm.20198
[8] Luetmer, P. H., & Mokri, B. (2003). Dynamic CT Myelography: A Technique for Localizing High-Flow Spinal Cerebrospinal Fluid Leaks. AJNR: American Journal of Neuroradiology, 24(8), 1711. https://pmc.ncbi.nlm.nih.gov/articles/PMC7973984/
[9] Cossu, G., Abbruzzese, G., Forni, G. L., Matta, G., Pinto, V., Ruffinengo, U., Oppo, V., & Marchese, R. (2019). Efficacy and safety of deferiprone for the treatment of superficial siderosis: results from a long-term observational study. Neurological sciences: official journal of the Italian Neurological Society and the Italian Society of Clinical Neurophysiology, 40(7), 1357–1361. https://doi.org/10.1007/s10072-019-03847-x
[10] Charidimou, A., Perosa, V., Frosch, M. P., Scherlek, A. A., & Greenberg, S. M. (2020). Neuropathological correlates of cortical superficial siderosis in cerebral amyloid angiopathy.Brain,143(11), 3343. https://doi.org/10.1093/brain/awaa266