
{kind=link}

Serous Carcinoma Symptoms Serous Carcinoma is among the most aggressive and lethal human cancers. It is a high-grade epithelial disease, highly invasive, quick to grow, and frequently remains undetected until well into disease progression. Predominantly affecting the ovaries, fallopian tubes, and peritoneum (collectively termed pelvic high-grade serous carcinoma , HGSC ), it also arises in the endometrium ( uterine serous carcinoma , USC ) but rarely elsewhere. One of the most dangerous aspects of serous carcinoma is that its cellular behavior promotes rapid, uncontrolled growth. The tumor cells quickly develop the ability to invade healthy tissue and also ignore normal cell death signals. This is why it is a leading cause of gynecological deaths globally. To better explain, uterine serous carcinoma represents only about 10% of uterine cancers, yet accounts for 39% of uterine cancer-associated fatalities. 1 Ferriss, J. S., Erickson, B. K., Shih, I., & Fader, A. N. (2021). Uterine serous carcinoma: Key advances and novel treatment approaches. International Journal of Gynecological Cancer , 31 (8), 1165-1174. https://doi.org/10.1136/ijgc-2021-002753
Pathological Features of Serous Carcinoma: Serous Carcinoma Symptoms
Serous carcinoma is an epithelial tumor, which means that it is a cancer that starts in the thin layer of tissue that lines the outer surface of organs or that lines the cavities within organs. The term serous actually refers to its microscopic appearance, being similar to the fallopian tube epithelium. Most high grade serous cancers (HGSC) actually originate from the fallopian tubes.
Some histological features observed under the microscope are:
- Finger-like (papillary) structures
- Slit-like spaces between epithelial folds
- Tall, columnar cells with nuclear pleomorphism and prominent nucleoli
- High mitotic index, with rapid and chaotic cell division
- Round, calcified structures (Psammoma bodies)
Subtypes of Serous Carcinoma
On the basis of histology, behavior, and molecular profiles, there are three subtypes of serous carcinomas, and they differ a lot in diagnostic approach and treatment as well.
- High-Grade Serous Carcinoma (HGSC)
- Low-Grade Serous Carcinoma (LGSC)
- Uterine Serous Carcinoma (USC)
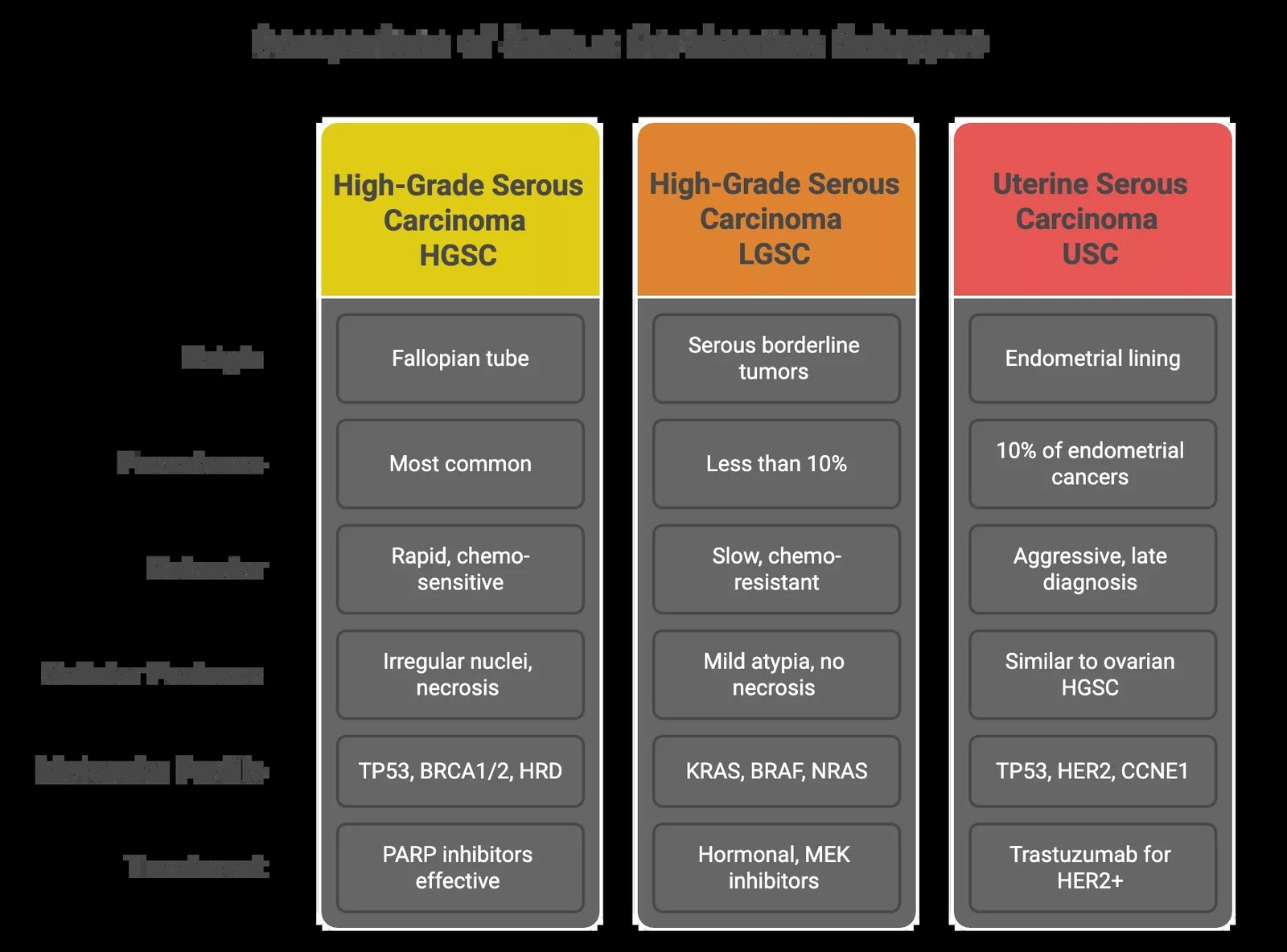
Quick comparison between the different subtypes of serous carcinoma: HGSC, LGSC, and USC. There are notable differences in their behaviors and molecular profiles, which guide the treatment plans.

Histological comparison of low-grade and high-grade serous ovarian carcinoma: Low-grade serous carcinoma (LGSC) shows relatively uniform cells and up to 12 mitoses per 10 high-power fields. In contrast, high-grade serous carcinoma (HGSC) displays marked nuclear atypia, significant pleomorphism, and more than 12 mitoses per 10 high-power fields. (Image Courtesy: Ciucci A., Franco Zannoni G., Buttarelli M., Martinelli E., Mascilini F., Petrillo M., Ferrandina G., Scambia G., Gallo D. Ovarian low and high grade serous carcinomas: hidden divergent features in the tumor microenvironment. Oncotarget. 2016; 7: 68033-68043. Available fromOncotarget. Licensed under CC by 3.0)
Epidemiology & Risk Factors
Serous carcinoma is one of the deadliest gynecologic cancers, and its risk factors vary by subtype, though they often overlap.
- High-Grade Serous Carcinoma (HGSC) is the most common subtype and accounts for the majority of ovarian cancer deaths (70-80%). It mostly affects postmenopausal women, especially in their 60s and 70s.
- Genetic predisposition is by far the largest factor. HGSC has a special relationship with germline mutations of BRCA1 and BRCA2. These mutations damage DNA repair systems, allowing cancer to take root. Other associated mutations include PALB2, RAD51C/D, BRIP1, and those found in Lynch syndrome (although USC is more affected by that).
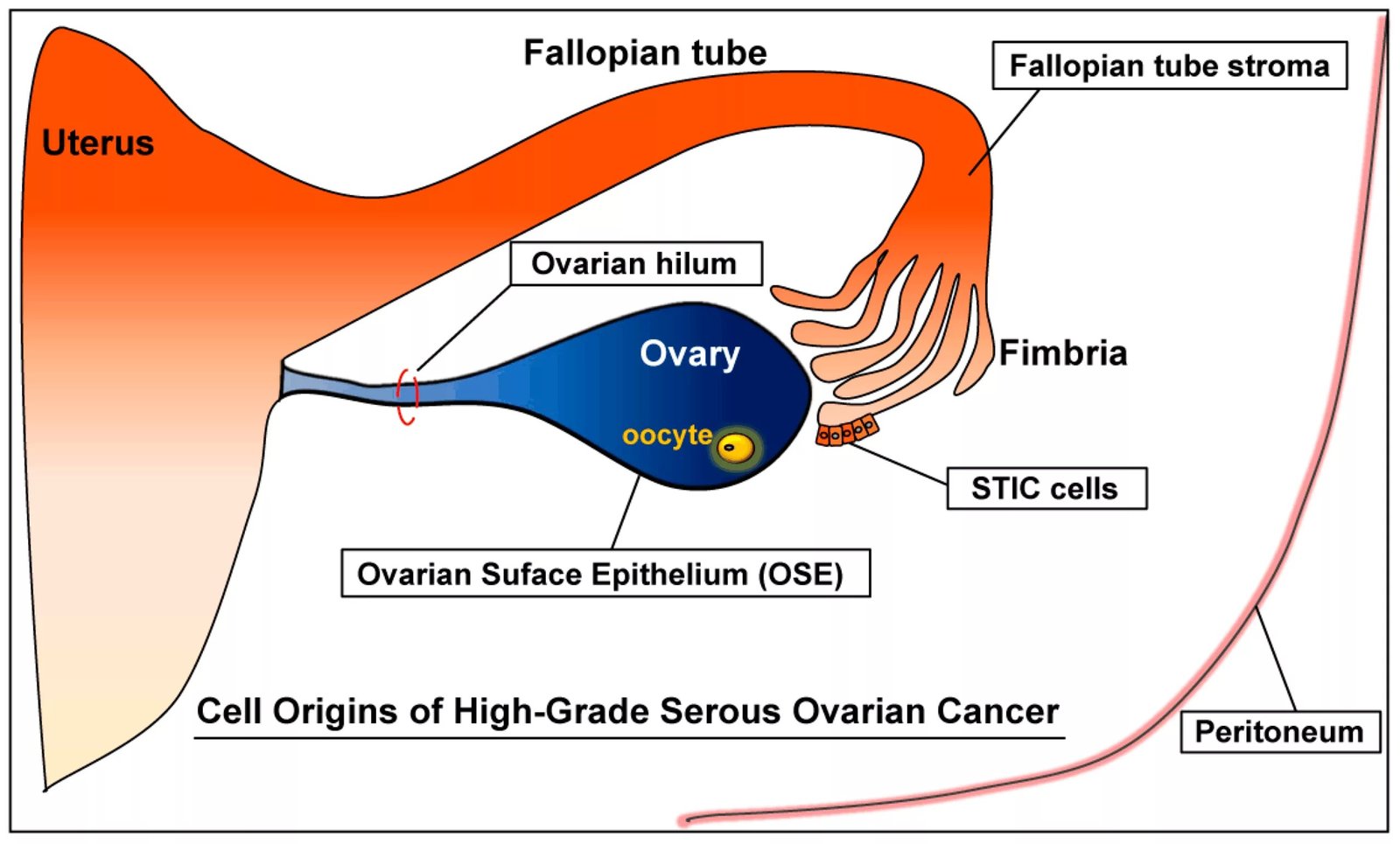
High-Grade Serous Carcinoma and its precursor lesion: Serous tubal intraepithelial carcinoma (STIC) at the fimbriated end of the fallopian tubes. (Image Courtesy: Kim, J., Park, E. Y., Kim, O., Schilder, J. M., Coffey, D. M., Cho, C., & Bast, R. C. (2018). Cell Origins of High-Grade Serous Ovarian Cancer. Cancers, 10(11), 433. https://doi.org/10.3390/cancers10110433. Available fromMDPI. Licensed under CC by 4.0)
- Low-Grade Serous Carcinoma (LGSC) is rarer and tends to affect younger women in their 40s or 50s. And while the progression is slower as compared to HGSC, it’s more resistant to standard chemotherapy. Risk factors include nulliparity because of uninterrupted ovulation, which is considered a risk factor for most gynecological cancers. Unlike HGSC, familial cancer syndromes are less frequently involved.
- Uterine Serous Carcinoma (USC) is statistically responsible for a major share of endometrial cancer deaths despite being less common overall. It usually develops in older women, especially those over 65. Black women, those with a history of tamoxifen use, and those who have never given birth may be at higher risk. HER2 amplification and TP53 mutations are key molecular drivers.
Signs & Symptoms of Serous Carcinoma
| Symptom | HGSC | LGSC | USC |
|---|---|---|---|
| Abdominal bloating | ✅ | ✅ | ❌ |
| Visible ascites | ✅ | ❌ | ❌ |
| Pelvic pain/pressure | ✅ | ✅ | ✅ |
| Early satiety | ✅ | ✅ | ❌ |
| Postmenopausal bleeding | ❌ | ❌ | ✅ |
| Vaginal discharge | ❌ | ❌ | ✅ |
| Urinary frequency | ✅ | ✅ | ❌ |
| Unexplained weight loss | ✅ | ✅ | ✅ |
Diagnosis of Serous Carcinoma
Diagnosing serous carcinoma is rarely straightforward because most patients present with vague symptoms that are very similar to benign conditions. By the time imaging is done, the disease is often advanced. Since the treatment plan (like eligibility for PARP inhibitors, trastuzumab, or immunotherapy) is mainly dependent on the subtype, identifying it is a major goal of diagnosis.
High-Grade Serous Carcinoma (HGSC):
Since HGSC is usually only diagnosed at an advanced stage (III/IV), most cases require a stepwise approach for confirmation.
Initial Imaging
- Transvaginal ultrasound for adnexal masses
- CT or MRI to see the disease spread
Tumor Marker Assessment
- Serum CA-125 is elevated in 80% of advanced cases
- It’s not specific enough to detect the tumor at an early stage
Surgical Exploration
- Diagnostic laparoscopy or laparotomy for tissue confirmation and removal (debulking)
Histopathology
- Definitive diagnosis requires histopathological examination after surgical exploration: complex papillary architecture, high mitotic index, marked nuclear atypia
- Immunohistochemistry often shows strong p53 staining
Molecular & Genetic Testing
- BRCA1/2 testing is standard for all diagnosed patients, even if there’s no family history
- Most significant is Homologous Recombination Deficiency (HRD). HRD mainly arises from germline mutations in BRCA1/ and somatic mutations in BRCA1/2
- HRD testing informs eligibility for PARP inhibitors
Low-Grade Serous Carcinoma (LGSC):
LGSC presents similarly to HGSC but often with a longer symptom history. Many cases arise from serous borderline tumors, which may be diagnosed incidentally or during workup for pelvic symptoms.
Imaging
- Transvaginal ultrasound shows complex or cystic masses
- CT/MRI used for staging and preoperative planning
Tumor Marker
- CA-125 is often elevated, but inconsistent
Surgical Staging
- Standard gynecologic oncology approach: oophorectomy (surgical removal of ovaries), omentectomy (removal of omentum, which is a fatty tissue layer in the abdomen that covers and protects the intestines and other organs), lymph node assessment
Histopathological Evaluation
- Shows mild atypia, low mitotic rate, and uniform nuclei
- You can see signs of transition from borderline tumors
Molecular Testing
- KRAS, BRAF, and NRAS mutations are common
- TP53, HRD, and BRCA mutations are rare
Uterine Serous Carcinoma (USC):
USC presents with postmenopausal bleeding and is frequently diagnosed through endometrial evaluation.
Transvaginal Ultrasound
- Detects endometrial thickening or intrauterine masses
Endometrial Biopsy or Hysteroscopy
- Confirms serous subtype based on high-grade nuclear features and prominent nucleoli
Immunohistochemistry & Molecular Profiling
- p53 overexpression is the hallmark of USC
- HER2/neu amplification in 25–30% cases, which guides trastuzumab use
- MMR/MSI status testing to guide immunotherapy
- Additional mutations sometimes seen are FBXW7, PP2R1A, CCNE1
Surgical Staging
- Total hysterectomy with bilateral salpingo-oophorectomy (removal of both ovaries and fallopian tubes)
- Omentectomy and peritoneal biopsies as indicated
Stages of Serous Carcinoma
Serous carcinoma staging follows the FIGO (International Federation of Gynecology and Obstetrics) system, which categorizes disease progression from Stage I (early/localized) to Stage IV (advanced/metastatic).
Ovarian / Fallopian Tube / Peritoneal Serous Carcinoma (HGSC & LGSC):
HGSC and LGSC both follow FIGO ovarian cancer staging.
| Stage | Description |
|---|---|
| Stage I | Tumor confined to one or both ovaries/fallopian tubes |
| Stage II | Spread to pelvis (e.g. uterus, bladder, rectum) |
| Stage III | Spread to the abdominal cavity or the retroperitoneal lymph nodes |
| Stage IV | Distant metastasis (e.g. pleura, liver parenchyma, lungs) |
Uterine Serous Carcinoma (USC)
USC follows FIGO endometrial cancer staging.
| Stage | Description |
|---|---|
| Stage I | Tumor confined to uterus |
| Stage II | Invasion of cervical stroma |
| Stage III | Spread to ovaries, pelvic tissues, or lymph nodes |
| Stage IV | Invasion into bladder/rectum or distant metastasis (e.g. lungs, liver) |
Treatment of Serous Carcinoma
Treatment for serous carcinoma is not a one-size-fits-all approach. It depends on:
- Location of the tumor
- Stage of cancer at diagnosis
- Histologic grade of the tumor
- Molecular profiling

The exact treatment plan for serous carcinomas is guided according to the subtype, stage at the time of diagnosis, and molecular profiles
High-Grade Serous Carcinoma:
A combined approach of surgery and chemotherapy is almost always the recommended treatment of HGSC.
First-Line Treatment
- Surgery: Doctors aim to remove as much visible tumor as possible. This surgery is called “cytoreduction.”10Pomel, C., Jeyarajah, A., Oram, D., Shepherd, J., Milliken, D., Dauplat, J., & Reynolds, K. (2007). Cytoreductive surgery in ovarian cancer. Cancer imaging : the official publication of the International Cancer Imaging Society, 7(1), 210–215. https://doi.org/10.1102/1470-7330.2007.0030 and significantly affects survival.
- Chemotherapy: Typically 6 cycles of carboplatin and paclitaxel, given every 3 weeks. If surgery isn’t possible right away (due to disease spread or the patient is not medically fit), chemotherapy may be started first (called neoadjuvant chemotherapy).
- Targeted Therapy (Bevacizumab): Some patients receive a drug called bevacizumab, which blocks the blood supply to the tumor. It is added to chemo and continued afterward as maintenance.
Maintenance Therapy
Once primary chemo is done, maintenance therapy is started, based on HRD and BRCA status:
- BRCA1/2 mutation: PARP inhibitors (Olaparib or Niraparib)
- HRD-positive (but BRCA negative): PARP inhibitor alone or combined with bevacizumab
- HRD-negative: Bevacizumab is the main option; PARP inhibitors show limited benefit
Recurrent Disease
- Platinum-Sensitive Recurrence (after 6 months): Re-treatment with platinum-based chemo is standard, possibly with bevacizumab. PARP inhibitors may be used again if not used before.
- Platinum-Resistant Recurrence (within 6 months):
Low-Grade Serous Carcinoma (Ovarian):
LGSC grows slowly but shows resistance to standard chemotherapy. It demands a tailored, sometimes more hormonal or molecular approach.
Standard Treatment
- Surgery: Follows a similar surgical approach to HGSC, to remove as much tumor as possible
- Chemotherapy: Often used post-surgery, response rates are lower than in HGSC
- Hormonal Maintenance Therapy: After surgery, many patients receive hormone-blocking medications like aromatase inhibitors to slow tumor growth
Recurrent Disease:
- Hormonal therapies (like AIs, tamoxifen, GnRH agonists) are frequently used
- Targeted drugs (like MEK inhibitors) show promise, especially in tumors with KRAS or BRAF mutations
- Chemotherapy is considered case-by-case, depending on symptoms and progression
Uterine Serous Carcinoma (USC):
Even though USC arises in the uterus, it behaves more like HGSC than other endometrial cancers.
First-Line Treatment
- Surgery: Total abdominal hysterectomy, with removal of ovaries, fallopian tubes, omentum, and lymph nodes
- Adjuvant Therapy: Given USC’s high recurrence rate, adjuvant treatment is nearly always needed after surgery, even in early-stage disease.
| Stage | Standard Adjuvant Therapy |
|---|---|
| Stage I | Vaginal brachytherapy with chemotherapy |
| Stage II–IV | Carboplatin + Paclitaxel often combined with external beam radiation therapy (EBRT) |
| HER2-positive tumors | AddTrastuzumab (herceptin)to chemotherapy |
Recurrent or Metastatic Disease
- Same chemotherapy regimens, with trastuzumab (if HER2-positive), are first-line
- PARP inhibitors may help if the tumor is HRD-positive
- Immunotherapy for MSI-high or MMR-deficient tumors
Prognosis & Life Expectancy for Serous Carcinoma
Serous carcinomas vary widely in behavior and treatment response, which means prognosis isn’t one-size-fits-all. Factors like cancer stage at diagnosis, subtype, molecular profile, and treatment response all play a role in shaping a patient’s outlook.
| Subtype | Typical Stage at Diagnosis | 5-Year Survival Rate11Aluloski, I., Tanturovski, M., Jovanovic, R., Kostadinova-Kunovska, S., Petrusevska, G., Stojkovski, I., & Petreska, B. (2017). Survival of Advanced Stage High-Grade Serous Ovarian Cancer Patients in the Republic of Macedonia. Open Access Macedonian Journal of Medical Sciences, 5(7), 904. https://doi.org/10.3889/oamjms.2017.215 | Key Prognostic Factors |
|---|---|---|---|
| HGSC | Stage III/IV in 70%+ cases | ~45–50% (Stage III), <30% (Stage IV) | Surgical debulking success, BRCA/HRD status, PARPi use |
| LGSC | Often Stage I–III | ~70–85% (early), 40–60% (advanced) | Indolent course but chemo-resistant; hormonal therapy may help |
| USC | Often Stage III–IV | ~60% (Stage I), ~30% (advanced) | Early spread, HER2 status, response to chemo/trastuzumab |
Other than staging, molecular markers also predict prognosis:
- BRCA1/2 Mutations / HRD+ Tumors (HGSC) respond well to PARP inhibitors
- HER2/neu Amplification (USC) identifies patients who may benefit from trastuzumab-based therapy
- CCNE1 Amplification (HGSC/USC) is associated with poor prognosis and PARP resistance
- KRAS / BRAF mutations (LGSC) define molecular targets for experimental therapies like MEK inhibitors
Emerging Therapies for Treatment of Serous Carcinoma
Serous carcinoma treatment is changing rapidly. New drugs are attacking the individual vulnerabilities inside the cancer cells, replacing toxic chemotherapy with precision medicine.
Beating PARP Inhibitor Resistance:
PARP inhibitors (like Olaparib) are for HRD-positive tumors, but most tumors become resistant over time. We have a number of clinical trials looking for a solution. The most common are combinations of PARPi with:
- ATR inhibitors (attack the cell’s backup repair system)
- WEE1 inhibitors (block cancer cells from repairing DNA damage)
- Immunotherapy (helps immune cells find and kill tumor cells)
Smarter Chemotherapy: Antibody-Drug Conjugates (ADCs)
ADCs are chemotherapy agents designed like targeted missiles, armed to kill only the cancer cells, none of the normal cells. Some approaches are already being used, like Mirvetuximab for recurrent HGSC with Folate receptor alpha (FRα). Several others are still in active clinical development, like drugs targeting NaPi2b, Mesothelin, and other tumor-specific markers.
Targeting Cyclin E:
Some cells show abnormal expression of Cyclin E (CCNE1), which imparts an aggressive nature and renders tumor cells PARP inhibitor resistant. CDK2 inhibitors, which target the Cyclin E-CDK2 complexes in tumor cells, have entered into clinical trials.
Immunotherapy Combinations:
Currently, it gives benefit in very few cases with MSI-H/dMMR mutations. But trials are testing combos to widen its use (PD-1/PD-L1 inhibitors with PARP inhibitors, antiangiogenics, chemotherapy, or novel immunomodulators).
Prevention & Prediction of Serous Carcinoma
There’s no sure way to prevent serous carcinoma, and it’s hard to detect until it’s in an advanced stage. But prevention and detection are getting better.
- Since many high-grade serous carcinomas (HGSC) start in the fallopian tubes, doctors now recommend removing the tubes during procedures like tubal ligation, C-sections, hysterectomies, and other gynecologic surgeries. This is called “opportunistic salpingectomy,” and it’s a low-risk way to cut cancer risk before it starts.
- Risk-reducing salpingo-oophorectomy (RRSO) works very well for BRCA carriers (especially premenopausal women). It is recommended to be tested for BRCA1, BRCA2, and other HRR genes if you have a strong family history of ovarian, breast, and endometrial cancer. This can reduce ovarian cancer risk by over 80%.
- There’s currently no reliable screening test for HGSC. But scientists are working on liquid biopsies (tumor DNA in blood), AI-based imaging tools, and new blood biomarkers that may detect cancer earlier.
Conclusion
Serous carcinoma, HGSC in particular, remains one of the most lethal forms of gynecologic cancer. It’s often diagnosed late and is difficult to treat. But new molecular profiling, targeted therapies, and personalized treatment have transformed the landscape.
We now understand that serous carcinoma isn’t just one disease: it’s several subtypes with distinct behaviors and genetic signatures. This shift has allowed us to match the right therapy to the right patient, using tools like BRCA and HRD testing, HER2 profiling, and targeted therapies like PARP inhibitors and antibody-drug conjugates.
That said, challenges remain: early detection is still difficult, resistance can develop, and not every patient has access to the latest treatments. But with continued research, patient education, and better clinical options, there’s real hope for longer survival.
References
[1] Ferriss, J. S., Erickson, B. K., Shih, I., & Fader, A. N. (2021). Uterine serous carcinoma: Key advances and novel treatment approaches.International Journal of Gynecological Cancer,31(8), 1165-1174. https://doi.org/10.1136/ijgc-2021-002753
[2] Reade, C. J., McVey, R. M., Tone, A. A., Finlayson, S. J., McAlpine, J. N., Fung-Kee-Fung, M., & Ferguson, S. E. (2014). The fallopian tube as the origin of high grade serous ovarian cancer: review of a paradigm shift. Journal of obstetrics and gynaecology Canada : JOGC = Journal d’obstetrique et gynecologie du Canada : JOGC, 36(2), 133–140. https://doi.org/10.1016/S1701-2163(15)30659-9
[3] Gaillard F, Yap J, Yu Y, et al. Psammoma bodies. Reference article, Radiopaedia.org (Accessed on 30 Jul 2025) https://doi.org/10.53347/rID-1928
[4] Ferlay, J., Shin, R., Bray, F., Forman, D., Mathers, C., & Parkin, D. M. (2010). Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International Journal of Cancer, 127(12), 2893-2917. https://doi.org/10.1002/ijc.25516
[5] Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. 1998 Sep 4 [Updated 2025 Mar 20]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1247/
[6] Stewart, M. D., Merino Vega, D., Arend, R. C., Baden, J. F., Barbash, O., Beaubier, N., Collins, G., French, T., Ghahramani, N., Hinson, P., Jelinic, P., Marton, M. J., McGregor, K., Parsons, J., Ramamurthy, L., Sausen, M., Sokol, E. S., Stenzinger, A., Stires, H., Timms, K. M., … Allen, J. (2022). Homologous Recombination Deficiency: Concepts, Definitions, and Assays. The oncologist, 27(3), 167–174. https://doi.org/10.1093/oncolo/oyab053
[7] Wallis, B., Bowman, K. R., Lu, P., & Lim, C. S. (2023). The Challenges and Prospects of p53-Based Therapies in Ovarian Cancer. Biomolecules, 13(1), 159. https://doi.org/10.3390/biom13010159
[8] Prat, J., & Oncology, G. (2015). FIGO’s staging classification for cancer of the ovary, fallopian tube, and peritoneum: Abridged republication. Journal of Gynecologic Oncology, 26(2), 87. https://doi.org/10.3802/jgo.2015.26.2.87
[9] Berek, J. S., Matias-Guiu, X., Creutzberg, C., Fotopoulou, C., Gaffney, D., Kehoe, S., Lindemann, K., Mutch, D., & Concin, N. (2023). FIGO staging of endometrial cancer: 2023. International Journal of Gynecology & Obstetrics, 162(2), 383-394. https://doi.org/10.1002/ijgo.14923
[10] Pomel, C., Jeyarajah, A., Oram, D., Shepherd, J., Milliken, D., Dauplat, J., & Reynolds, K. (2007). Cytoreductive surgery in ovarian cancer. Cancer imaging : the official publication of the International Cancer Imaging Society, 7(1), 210–215. https://doi.org/10.1102/1470-7330.2007.0030
[11] Aluloski, I., Tanturovski, M., Jovanovic, R., Kostadinova-Kunovska, S., Petrusevska, G., Stojkovski, I., & Petreska, B. (2017). Survival of Advanced Stage High-Grade Serous Ovarian Cancer Patients in the Republic of Macedonia. Open Access Macedonian Journal of Medical Sciences, 5(7), 904. https://doi.org/10.3889/oamjms.2017.215
[12] Pettinato M. C. (2021). Introduction to Antibody-Drug Conjugates. Antibodies (Basel, Switzerland), 10(4), 42. https://doi.org/10.3390/antib10040042
[13] Mor-Hadar, D., Wilailak, S., Berek, J., & McNally, O. M. (2024). FIGO position statement on opportunistic salpingectomy as an ovarian cancer prevention strategy. International Journal of Gynecology & Obstetrics, 167(3), 976-980. https://doi.org/10.1002/ijgo.15884