
{kind=link}

Retinal Detachment Medical Eye diseases are naturally a scare for most people; being able to see is an underrated blessing and something we take for granted. On top of that, most of the eye conditions that threaten your vision do not come with much warning, even if there are signs of warning, we tend to ignore them. Retinal detachment is one such condition that affects vision. In fact, it is an important cause of potentially preventable vision loss if not treated in time.
It is painless, which is why patients delay treatment. That said, it does have some warning signs, e.g, floaters and flashes, that should alert the patient to seek medical consultation. It is a medical emergency that requires urgent intervention, ideally within hours to days depending on macular involvement, and patients describe it as a ‘curtain’ or ‘shadow’ suddenly covering their vision.
Is it treatable? Yes, but only if intervention can be started immediately. Every hour of delay lowers the chances of reversal.
What is Retinal Detachment?: Retinal Detachment Medical
The retina is the light-sensitive layer at the back of the eye; you can think of it as the film inside a camera. It converts light into electrical signals sent to the brain via the optic nerve. Retinal detachment is actually the separation of the two layers of the retina. These two layers are: the neurosensory retina and the retinal pigment epithelium.
And the three types of retinal detachment are:
- Rhegmatogenous
- Tractional
- Exudative (serous)
Normal Anatomy
The neurosensory retina is actually the part that detects light and converts it into signals via cones and rods. But the RPE is just as important; it facilitates metabolic exchange and supports the neurosensory retina via the underlying choroidal circulation. Moreover, because there is basically no actual bonding between the layers, rather they are held together because of multiple factors: hydrostatic pressure, exchange of metabolic materials, and the vitreous. The RPE actively pumps fluid out of the subretinal space to maintain pressure that keeps the layers in contact. So basically, this is an active, ongoing process.
As soon as the layers are separated, nutrition cuts off, and retinal cells begin to die, which is why the speed of treatment is so important.
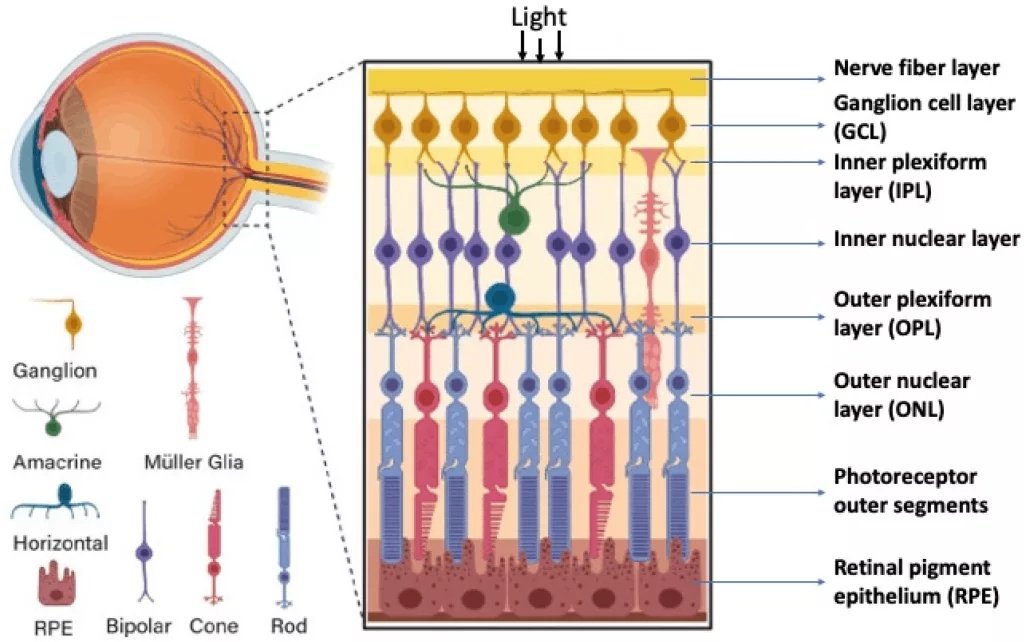
Structure of the retina, including the various layers and cell types. The photoreceptors and cells make up the sensory-neural retina, under which lies the RPE, closely related to the choroid. (Image Courtesy: Grigoryan, E. N. (2022). Self-Organization of the Retina during Eye Development, Retinal Regeneration In Vivo, and in Retinal 3D Organoids In Vitro. Biomedicines, 10(6), 1458. Available fromMDPIand licensed under CC by 4.0)
How Detachment Happens?
Rhegmatogenous:
- This is the most commonly seen. It begins when a full-thickness retinal tear develops in the neurosensory layer.
- Vitreous fluid passes through this break and starts accumulating in the subretinal space, and the RPE cannot pump fast enough to remove it.
- As a result, the neurosensory layer starts lifting off the RPE.
- Once separated, the photoreceptors (rods and cones) inside the sensory layer do not get oxygen and nutrition from the choroid under the RPE and slowly start to die. This is the irreversible part.
Tractional:
- This is seen most commonly in diabetic retinopathy, wherein fibrovascular proliferative membranes form on the retinal surface.
- There is no tear involved. Instead, these membranes start contracting over time, which creates mechanical traction.
- The traction pulls the retina away from the RPE, but compared to other types, this detachment is localized and slower, so there is more time to start treatment.
- Some other conditions where this presents are sickle cell disease and retinopathy of prematurity.
Exudative:
- As the name suggests, this type of detachment involves inflammatory processes, not tears. Essentially, the RPE or choroid vessels are disrupted by either inflammation, a tumor, or a systemic vascular disease.
- Fluid leaks into the subretinal space, and RPE isn’t able to clear it out fast enough.
- The retina gets separated even though there is no tear or traction.
- In this case, if the underlying cause is managed, the fluid is sometimes able to be reabsorbed, and the retinal layers may reattach.
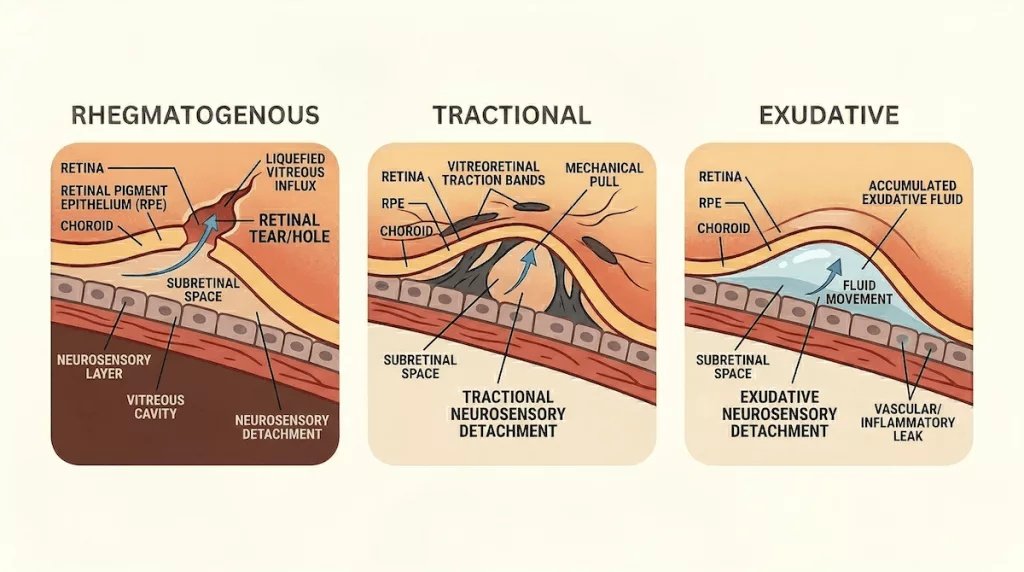
The three primary types of retinal detachment are Rhegmatogenous, characterized by a retinal tear allowing fluid into the subretinal space; Tractional, where vitreoretinal traction bands pull the retina away; and Exudative, caused by fluid accumulating beneath the retina due to leaks.
What is Vitreous Detachment?
The vitreous is a gel that fills 80% of the eye’s structure. It is confined inside the vitreous body, which lies in the posterior segment of the eye, and borders the retina. After the age of 50, it starts to shrink and move away from the retina; this is what we call posterior vitreous detachment (PVD).
Now, PVD itself does not cause vision loss; it is common and harmless. The problem arises in about 10-15% cases when it tugs hard enough on the retina and causes a tear. This tear can then lead to rhegmatogenous retinal detachment. This doesn’t always happen, but some risk factors that can cause a PVD to progress into a tear are high myopia, a history of eye trauma, or a previous surgery.
PVD presents as a sudden onset of floaters (cobwebs or rings) and flashes of light, especially in the peripheral vision, and this needs urgent medical care. Laser photocoagulation or cryotherapy can seal a tear before it becomes worse.
Causes of Detached Retina
Combining all three types, there can be several causes of retinal detachment:
- Ageing is the single biggest factor, for example, in the context of PVD
- High myopia (short-sightedness), because the eyeball becomes thinner and the retina is more stretched
- Previous retina detachment in the other eye is not per se a cause, but should indicate a risk
- Family history
- Physical trauma to the eye, like a blunt or penetrating injury
- Previous surgery, such as for a cataract
- Diabetic retinopathy
- Inflammatory eye diseases
How Does Retinal Detachment Present?
Retinal detachment presents with tell-tale symptoms and signs:
- Sudden increase in floaters
- Seeing flashes of light in the peripheral vision, which may seem like camera flashes
- A shadow or a curtain suddenly moving across the vision
- Blurred vision
- A dark area in the visual field that slowly expands
- Whichever of these changes the patient notices, they are painless
- Central vision may be preserved (if the macula is spared)
Involvement of the Macula
The macula is the central spot on the retina. It is the one point that has the most cones anywhere in the eye, and is responsible for fine details and color vision. When detachment involves the macula and subretinal fluid reaches it, the cone death is even quicker than in the other parts.
This is why the clinical distinction between macula-on and macula-off detachment is so important, prognosis-wise; it reflects how far the pathological process has advanced.
How Long Before Retinal Detachment Causes Blindness?
Retinal detachment is an emergency, and the opportunity for reversal depends on the location and speed of progression. For example, if the macula is spared, we can expect a good outcome if treated within 72 hours. But if the macula is also involved, central vision and sharp vision may not fully recover.
If left untreated, there might be complete detachment and severe vision loss within days. The message here stays the same: if you notice floaters, you need a same-day emergency assessment.
Diagnosis of Retinal Detachment
The symptoms are usually telling enough, but to see the exact extent of the condition, we use:
- Ophthalmoscopy (dilated fundus exam) is the gold standard, as it allows us to see the detachment directly
- Slit lamp examination with indirect ophthalmoscopy
- B-scan ultrasound for when the retina isn’t visible enough (e.g., with a dense cataract or vitreous haemorrhage)
- OCT (optical coherence tomography) can be useful for subtle or shallow detachments, and for assessing the macula
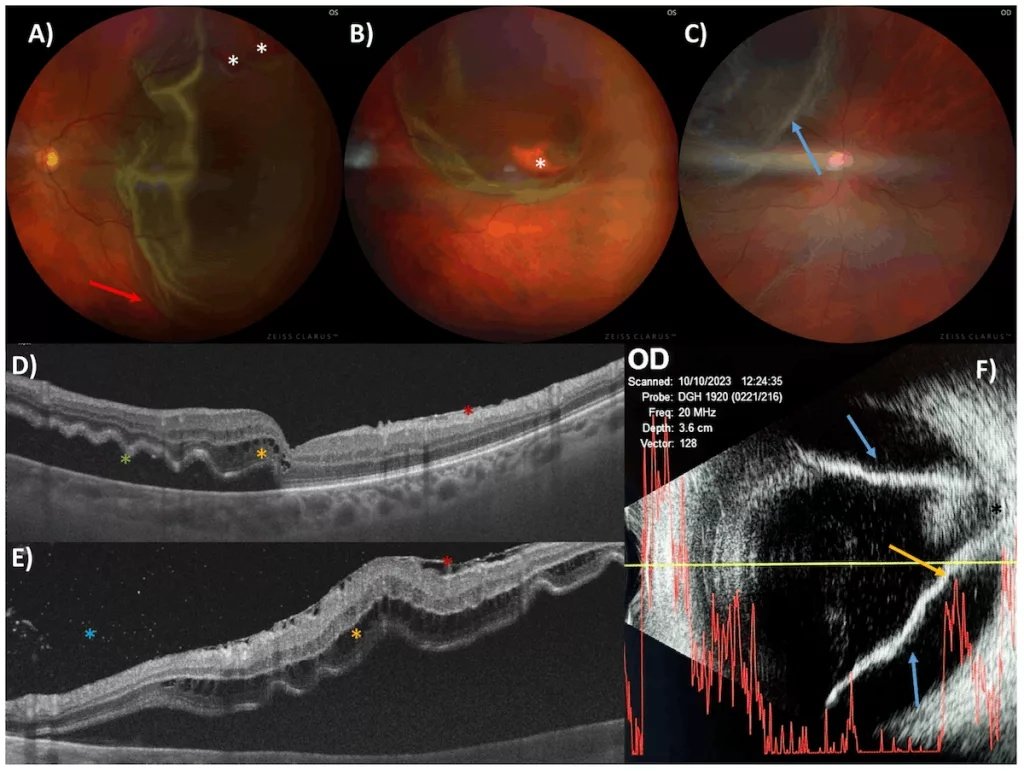
Diagnostic imaging in different patients with Rhegmatogenous Retinal Detachment (RRD):Fundus Photos (A–C):Clearly shows the physicalretinal tears(white stars) and chronicfolds(red arrows). Note the pale appearance of the detached tissue in panel(C).OCT Scans (D, E):High-resolution cross-sections revealingfluid cysts(yellow stars) andmembranes(red stars) forming on the retinal surface.Ocular Ultrasound (F):A classic“funnel-shaped” detachment(blue arrows). The A-scan confirms the separation by showing two distinct echo peaks for the detached layers. (Image Courtesy: Redruello-Guerrero, P., Gómez-Tomás, M., Rechi-Sierra, T., Molinero-Sicilia, L., Galindo-Cabello, N., Usategui-Martín, R., & Pastor-Idoate, S. (2025). Inflammatory Mechanisms in the Management and Treatment of Retinal Detachment. Metabolites, 15(7), 442. Available fromMDPIand licensed under CC by 4.0)
Treatment of Retinal Detachment
The treatment of choice depends on what stage the detachment process or the underlying cause is at. Fortunately, the success rates are high; ~80-90% of cases recover after a single procedure, and most remaining ones also reattach after a second procedure.
- Laser photocoagulation/cryotherapy is the intervention of choice for retinal tears, but only before the actual detachment occurs. The treatment creates a scar that seals the tear.
- In pneumatic retinopexy a gas bubble is injected into the eye that is supposed to push the retina back. The caveat here is that the patient must hold a specific head position for days. This is only used for certain detachment locations.
- Scleral buckle is where a silicone band is sutured around the outside of the eye to indent the wall and relieve traction. This is very effective, especially in younger patients.
- Vitrectomy is used when the cause is the shrinkage of the vitreous body. The vitreous gel is removed and replaced with gas or silicone oil; the retina is reattached from the inside. The most commonly used surgical approach today. However, silicon oil cases need a second operation later to remove the oil, which is not the case if gas is used instead.
Prognosis
Again, the prognosis is heavily dependent on the condition of the macula. In macula-on detachment, if treated promptly, there are excellent outcomes in most cases. However, in macula-off detachment, recovery is often incomplete because central vision can not be restored, peripheral vision is restored, though. The longer the macula has been detached, the worse the prognosis.
Post-surgery recovery also depends on the patient adhering to instructions, e.g., patients who have had gas bubbles placed cannot fly. Pressure changes in the air can cause the bubble to expand. Once someone has had retinal detachment in one eye, the other eye has a lifetime risk and needs to be monitored.
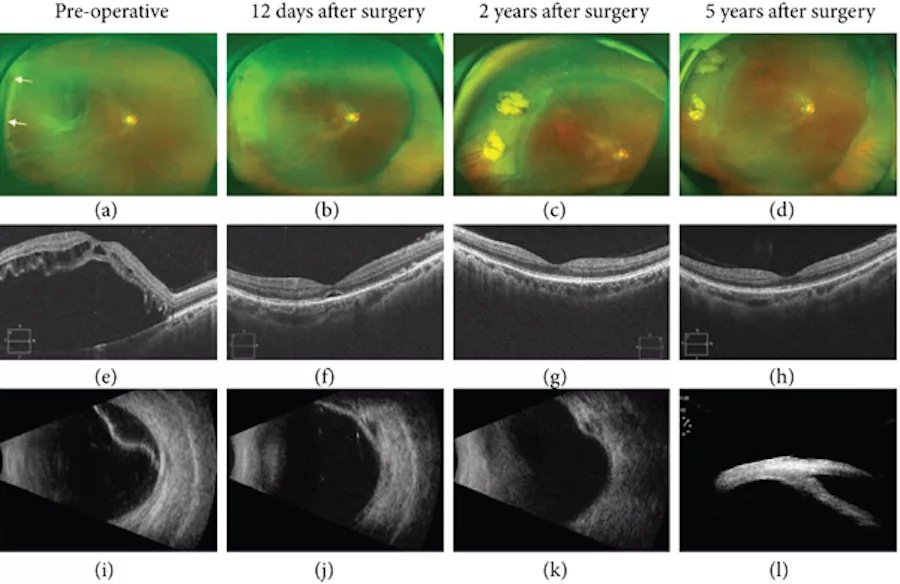
Improvement in a retinal detachment case over time:Before Surgery (a, e, i):Imaging shows a “macula-off” detachment with visible retinal holes and fluid cysts.After Surgery (b–l):A successful recovery sequence showing the retina reattached, the macula repositioned, and the surgical “buckle” in place, confirmed via photography, OCT, and ultrasound. (Image Courtesy: Li, Hui, Zhang, Conghui, Wei, Jiayi, Keyal, Khusbu, Wang, Fang, Six-Year Outcomes of 25-Gauge Chandelier Illumination-Assisted Scleral Buckling, BioMed Research International, 2021, 4628160, 6 pages, 2021. Available fromWileyand licensed under CC by 4.0)
Final Words
Medical literacy and public awareness about vision health are important. People need to know that any change in vision, or sudden appearance of floaters, is not something to be taken lightly, even if it’s painless. You should not wait for a routine GP appointment or delay a consultation, thinking it harmless.
Even flashes alone, without any other symptoms, warrant an urgent eye checkup within 24 hours. Every second lost is a risk against recovery. Also, the importance of follow-ups cannot be overstated. Redetachment is more common than you’d think.
References
[1] Wang, S., Li, W., Chen, M., Cao, Y., Lu, W., & Li, X. (2023). The retinal pigment epithelium: Functions and roles in ocular diseases. Fundamental research, 4(6), 1710–1718.
[2] Feltgen, N., & Walter, P. (2014). Rhegmatogenous retinal detachment–an ophthalmologic emergency. Deutsches Arzteblatt international, 111(1-2), 12–22.
[3] Stewart, M. W., Browning, D. J., & Landers, M. B. (2018). Current management of diabetic tractional retinal detachments. Indian journal of ophthalmology, 66(12), 1751–1762.
[4] Shah, D. N., Al-Moujahed, A., Newcomb, C. W., Kaçmaz, R. O., Daniel, E., Thorne, J. E., Foster, C. S., Jabs, D. A., Levy-Clarke, G. A., Nussenblatt, R. B., Rosenbaum, J. T., Sen, H. N., Suhler, E. B., Bhatt, N. P., Kempen, J. H., & Systemic Immunosuppressive Therapy for Eye Diseases Research Group (2020). Exudative Retinal Detachment in Ocular Inflammatory Diseases: Risk and Predictive Factors. American journal of ophthalmology, 218, 279–287.
[5] Ahmed F, Tripathy K. Posterior Vitreous Detachment. [Updated 2023 Aug 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-.
[6] Williams, K., & Hammond, C. (2019). High myopia and its risks. Community eye health, 32(105), 5–6.
[7] Mahmoudi, S., & Almony, A. (2016). Macula-Sparing Rhegmatogenous Retinal Detachment: Is Emergent Surgery Necessary?. Journal of ophthalmic & vision research, 11(1), 100–107.
[8] Bhende, M., Shetty, S., Parthasarathy, M. K., & Ramya, S. (2018). Optical coherence tomography: A guide to interpretation of common macular diseases. Indian journal of ophthalmology, 66(1), 20–35.
[9] Steel D. (2014). Retinal detachment. BMJ clinical evidence, 2014, 0710.
[10] Velez-Montoya, R., León, A. G., & Hernández-Quintela, E. (2019). Assessment of Postural Compliance After Pneumatic Retinopexy. Translational vision science & technology, 8(3), 4.
[11] Foster, W.J., Dowla, N., Joshi, S.Y. et al. The fluid mechanics of scleral buckling surgery for the repair of retinal detachment. Graefes Arch Clin Exp Ophthalmol 248, 31–36 (2010).
[12] Ross W. H. (2002). Visual recovery after macula-off retinal detachment. Eye (London, England), 16(4), 440–446.