
{kind=link}

Meningitis Outbreak UK The United Kingdom is currently facing a new public health challenge in the form of an invasive meningococcal disease outbreak. The cases started being tracked by health authorities in mid-March 2026, when they noticed an unusual concentration of cases in and around Canterbury, Kent. But as of 20th March, the Kent meningitis outbreak seems to have expanded. There have been cases confirmed in London and even as far as France.
The outbreak has been linked to a cluster of cases in Canterbury, with several infections reported among university students and close-contact social settings, according to public health authorities. According to reports by The Guardian, the outbreak has been linked to the University of Kent and gatherings at a Canterbury nightclub between 5 and 7 March, with multiple confirmed and probable cases and two fatalities reported. Medical professionals are emphasizing an urgent national response to prevent further spread among young adults.
What Is Meningitis?: Meningitis Outbreak UK
Meningitis is inflammation of the meninges: the protective membranes that surround the brain and spinal cord. It is a clinical syndrome with several possible causes, including bacteria, viruses, fungi, and in rare cases, parasites. Other than these, even some non-infectious conditions can cause this inflammation.
Unlike viral meningitis, which is often mild, bacterial meningitis caused by the B strain is a medical emergency that can lead to:
- Meningitis: Inflammation of the protective membranes (meninges) covering the brain and spinal cord.
- Septicaemia: A life-threatening blood poisoning that causes rapid organ failure.
The overall case fatality rate for bacterial meningitis is estimated at up to 10%, and survivors can be left with long-term complications, includinghearing loss, cognitive impairment, and limb loss, which is why early recognition and treatment are critical.

A 20-month-old survivor of meningococcal septicemia (Neisseria meningitidis) following life-altering amputations of both feet and the left hand. This case illustrates the rapid progression of arterial occlusions and gangrene—complications that can arise when bacteria enter the bloodstream. Early diagnosis and vaccination remain the primary defenses against such devastating outcomes. (Image Courtesy: Available fromPHILunder public domain)
What Is Meningitis B?
There are several distinct serogroups of Neisseria meningitidis, classified by the structure of their outer polysaccharide capsule: MenA, MenB, MenC, MenW, MenX, and MenY. Each requires a different vaccine formulation for protection.
In the current outbreak, the causative organism has been identified as Neisseria meningitidis serogroup B (known as meningococcal B, or MenB). It is actually the form most commonly associated with outbreaks in most temperate regions, including Europe, North America, and Australia.
Is there a vaccine for meningitis?
Yes, in fact, several vaccines against meningitis are part of national immunization campaigns as well as under the WHO. For example:
| Vaccine | Details |
|---|---|
| MMR vaccine | Protects againstmumps, a viral cause of meningitis |
| Pneumococcal vaccine | Provides protection against Streptococcus pneumoniae, a bacterial cause of meningitis |
| 6-in-1 vaccine | Includes protection against Hib (Haemophilus influenzae type b), which can also cause meningitis |
| MenACWY vaccine | Offered to teenagers in school Years 9 and 10, and to first-year university students up to age 25. Protects against serogroups A, C, W, and Y, but not B. |
| MenB vaccine (Bexsero)3Rappuoli, R., Pizza, M., Masignani, V., & Vadivelu, K. (2018). Meningococcal B vaccine (4CMenB): the journey from research to real world experience.Expert Review of Vaccines,17(12), 1111–1121. | Provides protection against meningococcal B disease |
Can You Still Get Meningitis If You Have Been Vaccinated?
Yes. No vaccine provides absolute protection, which is why you might have heard about booster doses for certain vaccines. In the case of this outbreak, understanding this point is especially important.
The MenB vaccine significantly reduces the risk of serious illness but does not cover all MenB strains, and it does not prevent a person from carrying and transmitting the bacteria. The MenACWY vaccine does not provide any protection against MenB at all. Vaccination status should never replace awareness of symptoms and prompt medical attention.
Vaccine Gap in Meningitis B
MenB has historically been difficult to vaccinate against because, structurally, the outer capsule is very similar to normal tissue. This has burdened vaccine developers for many years, although in the end, we did get a MenB vaccine (Bexsero), which was introduced into the NHS childhood vaccination schedule as recently as September 2015.
This is crucial context for the current outbreak: young people who are now at university, typically aged 18 to 22, were born before 2015 and did not receive MenB as part of the routine childhood schedule, unless they had a private MenB vaccine. Many of them will have received the MenACWY vaccine (offered in Years 9 and 10 at school), which protects against four other serogroups but provides no protection against MenB. This gap in population immunity is one reason why university-age students are particularly vulnerable right now.
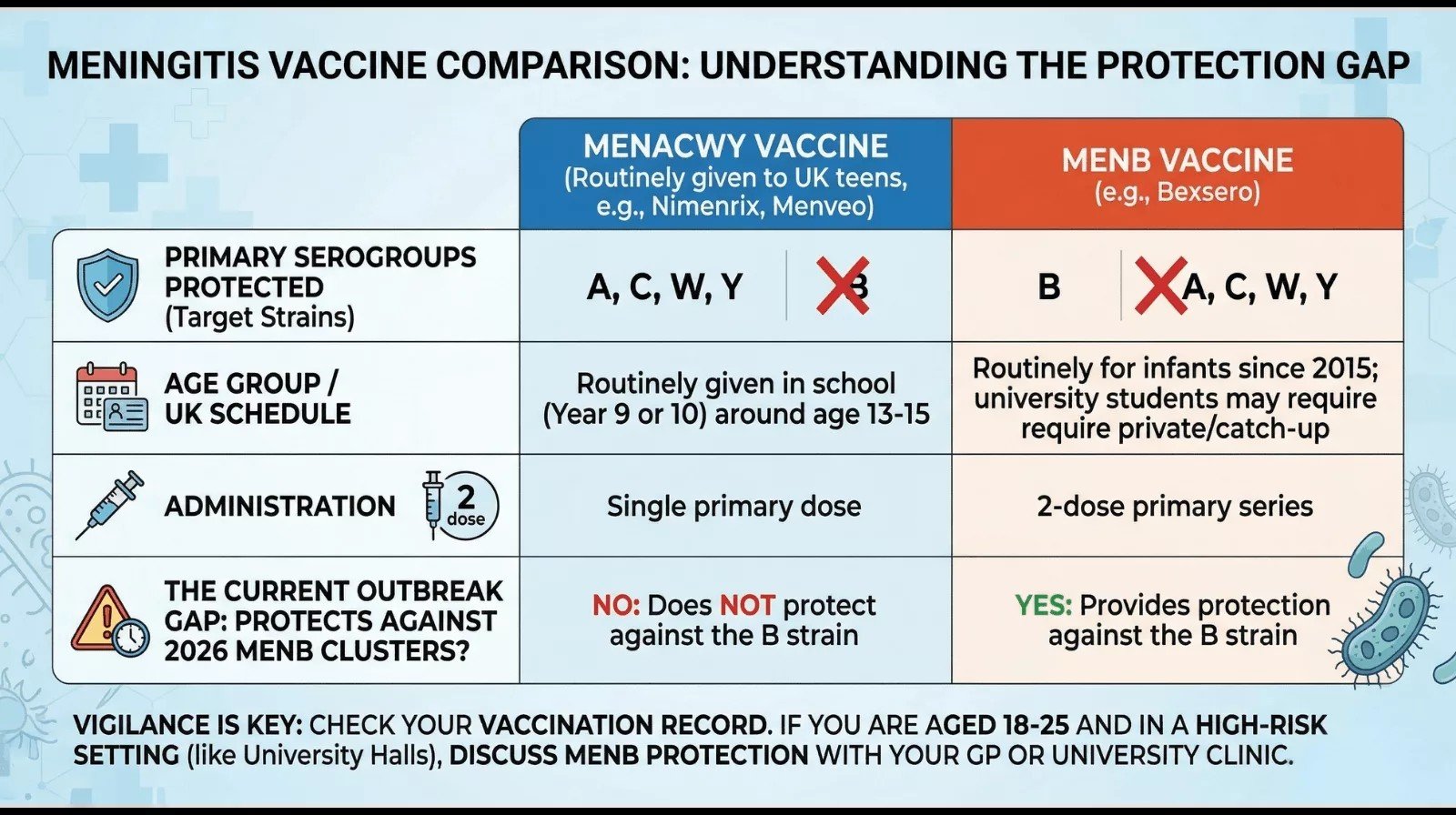
Many UK students believe they are protected because they received a meningitis jab in school. However, the routine MenACWY vaccine does not cover the B strain responsible for the 2026 Kent and London clusters. Only the MenB vaccine (Bexsero) provides the necessary protection for the current outbreak.
Is Meningitis Contagious?
This is one of the most common questions in the context of the Kent outbreak, and the answer requires some nuance. Meningitis itself, the inflammation, is obviously not contagious. However, Neisseria meningitidis, the bacteria are carried in the nose and throat and spread through respiratory droplets and direct contact with an infected person’s secretions, saliva, for instance.
Important to say that MenB isn’t airborne like measles or COVID-19. Casual, transient contact (i.e., sitting near someone on a bus or passing by them in a hallway) is not going to pose any increased risk. It requires close, sustained contact. It may also be carried asymptomatically; in general, approximately 10-20% of the population is a carrier, but this can be higher in settings of congregate living, like dorms.
That is what makes university environments epidemiologically concerning: high carrier rates, close living conditions, shared social spaces, and a younger age group that has not been fully vaccinated against MenB all create conditions in which an outbreak can gain momentum quickly.
Symptoms of Meningitis
One of the most dangerous characteristics of meningococcal disease is that its early symptoms are non-specific and easily mistaken for other illnesses, like a bad cold. Also, invasive meningitis moves with terrifying speed. Patients can go from just feeling unwell to a critical condition in under 24 hours.
Common Symptoms in Older Children and Adults
Symptoms will not all necessarily be present, but include:
- Severe headache occurs in ~ 90% of bacterial meningitis cases
- High fever
- Stiff neck, difficulty flexing the neck forward
- Sensitivity to light (photophobia) or loud noise
- Nausea and vomiting
- Drowsiness, confusion, or altered consciousness
- Rapid breathing and cold hands or feet
- A non-blanching rash, i.e., red or purple blotches that do not fade when pressed
The rash is one of the most recognisable signs of meningococcal septicaemia, but it does not always appear, and even when it does, it may develop late. On darker skin, it is important to check the palms, soles of the feet, the inside of the eyelids, and the roof of the mouth. The classic triad includes fever, neck stiffness, and altered mental status, although not all patients present with all three.
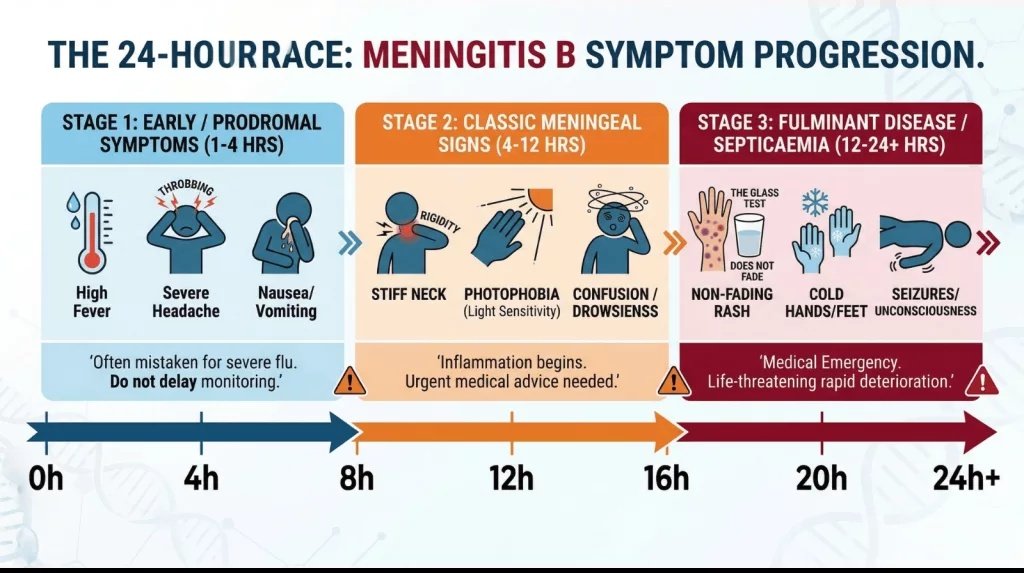
The 24-Hour Race of Meningitis B Progression.This timeline illustrates how bacterial meningitis can evolve from vague, flu-like symptoms into a life-threatening medical emergency within a single day.Note:Symptoms do not always appear in this exact order; if you suspect meningitis, seek emergency care immediately.
Symptoms in Babies
Infants cannot communicate pain, so it’s all the more important to be vigilant about signs:
- A bulging fontanelle (the soft spot on the head)
- High-pitched or unusual crying
- Poor feeding or refusing feeds
- Stiffness or floppiness
- Extreme irritability or, conversely, difficulty waking
- Cold hands and feet with a mottled or pale appearance
The Public Health Response
The meningitis UK strategy for this outbreak and for any future outbreak has two aspects:
1. Prophylactic Antibiotics
The immediate priority is prophylactic antibiotics (ciprofloxacin), vaccination alone at this point is not going to have an effect. Antibiotics are being given to close contacts of confirmed or suspected cases to prevent infection from spreading onward.
2. Targeted Vaccination
A mass meningitis B vaccine program is underway at the University of Kent. Students are being encouraged to access the private meningitis B vaccine through private pharmacies like Boots, though the NHS is providing it for free to those in the immediate risk zone in Canterbury.
Are People Outside Kent At Risk?
This outbreak poses a bigger risk for young adults, particularly those with direct connections to the University of Kent and the Canterbury area. For the general population in the rest of England, UKHSA has consistently stated that the overall risk of MenB outside the Kent area remains low. MenB is not as contagious as other respiratory infections, and its transmission requires close, sustained contact rather than brief or casual exposure.
Until now, the cases identified in London and the one case in France have all been traced back to the University of Kent, and the outbreak measures are expected to control the spread.
That said, anyone can develop meningitis, and vigilance is always needed. Babies and young children, teenagers, and young adults remain the demographic groups most commonly affected. Adults with weakened immune systems or who have had their spleen removed are also at higher risk.
Takeaway
If you or someone you know is in any of the at-risk groups or has been in the Canterbury area, watch out for any symptoms to develop, and act immediately if they appear. It can be fever, severe headache, stiff neck, light sensitivity, vomiting, drowsiness, and a non-blanching rash.
It’s also recommended to collect prophylactic antibiotics from a distribution site or your local GP. Check your vaccination history. If you have not received MenACWY (offered in school Years 9 and 10), contact your doctor, and also consider MenB vaccination privately.
Do not dismiss symptoms; meningitis B deteriorates very dramatically, and early intervention might be the only thing preventing a fatal outcome.
References
[1] The Guardian. Kent meningitis outbreak timeline and authorities’ response. The Guardian [Internet]. 2026 Mar 17 [cited 2026 Mar 21]. Available from: https://www.theguardian.com/society/2026/mar/17/kent-meningitis-outbreak-timeline-authorities-response
[2] Harrison, O. B., Claus, H., Jiang, Y., Bennett, J. S., Bratcher, H. B., Jolley, K. A., Corton, C., Care, R., Poolman, J. T., Zollinger, W. D., Frasch, C. E., Stephens, D. S., Feavers, I., Frosch, M., Parkhill, J., Vogel, U., Quail, M. A., Bentley, S. D., & Maiden, M. C. (2013). Description and nomenclature of Neisseria meningitidis capsule locus. Emerging infectious diseases, 19(4), 566–573.
[3] Rappuoli, R., Pizza, M., Masignani, V., & Vadivelu, K. (2018). Meningococcal B vaccine (4CMenB): the journey from research to real world experience.Expert Review of Vaccines,17(12), 1111–1121.
[4] Gonzalez Tome, M., Gonzalez-Quevedo, R., Escudeiro Dos Santos, M., Dornbusch, H. J., Straus, S., & Cooke, E. (2025). Meningococcal B Vaccines as a Paradigm of Safe and Effective Vaccines for Children. Vaccines, 13(7), 770.
[5] Villena, R., Kriz, P., Tin Tin Htar, M., Burman, C., Findlow, J., Balmer, P., & Jodar, L. (2023). Real-world impact and effectiveness of MenACWY-TT. Human vaccines & immunotherapeutics, 19(2), 2251825.
[6] Jeppesen, C. A., Snape, M. D., Robinson, H., Gossger, N., John, T. M., Voysey, M., Ladhani, S., Okike, I. O., Oeser, C., Kent, A., Oliver, J., Taylor, P., Morales-Aza, B., Clarke, S. C., Casey, M., Martins, F., Kitchin, N. R., Anderson, A. S., Jones, H., Jansen, K. U., … Pollard, A. J. (2015). Meningococcal carriage in adolescents in the United Kingdom to inform timing of an adolescent vaccination strategy. The Journal of infection, 71(1), 43–52.
[7] Weil, L. M., Crowe, S. J., Rubis, A. B., Soeters, H. M., Meyer, S. A., Hariri, S., & McNamara, L. A. (2023). Risk Factors for Serogroup B Meningococcal Disease Among College Students. Open forum infectious diseases, 10(12), ofad607.
[8] Wells, L. C., Smith, J. C., Weston, V. C., Collier, J., & Rutter, N. (2001). The child with a non-blanching rash: how likely is meningococcal disease?. Archives of disease in childhood, 85(3), 218–222.
[9] Zainel, A., Mitchell, H., & Sadarangani, M. (2021). Bacterial Meningitis in Children: Neurological Complications, Associated Risk Factors, and Prevention. Microorganisms, 9(3), 535.
[10] UK Health Security Agency. Meningococcal disease: guidance, data and analysis. UKHSA [Internet]. 2024 [cited 2026 Mar 21]. Available from: https://www.gov.uk/government/collections/meningococcal-disease-guidance-data-and-analysis
[11] National Health Service (NHS). Meningitis B vaccine overview. NHS [Internet]. 2024 [cited 2026 Mar 21]. Available from: https://www.nhs.uk/conditions/vaccinations/meningitis-b-vaccine/