
{kind=link}

Sialadenitis Symptoms Diagnosis Sialadenitis is the inflammation of one or more salivary glands, which are responsible for producing saliva in the mouth. It occurs mostly due to bacterial and viral infection and less commonly due to autoimmune disorders and sialolithiasis (stones in the salivary gland ducts). It should not be confused with sialadenosis (sialosis), which is a non-inflammatory, usually bilateral enlargement of the major salivary glands.
There are three major salivary glands in our mouth:
- Parotid gland (located in front of each ear)
- Submandibular gland (located beneath the jaw on both sides)
- Sublingual gland (located under the tongue on the floor of our mouth)
Additionally, numerous minor salivary glands are located in our lips, inner cheeks, and the lining of the oral cavity (oral mucosa). Sialadenitis primarily affects the parotid and submandibular glands, although minor glands can also be affected.
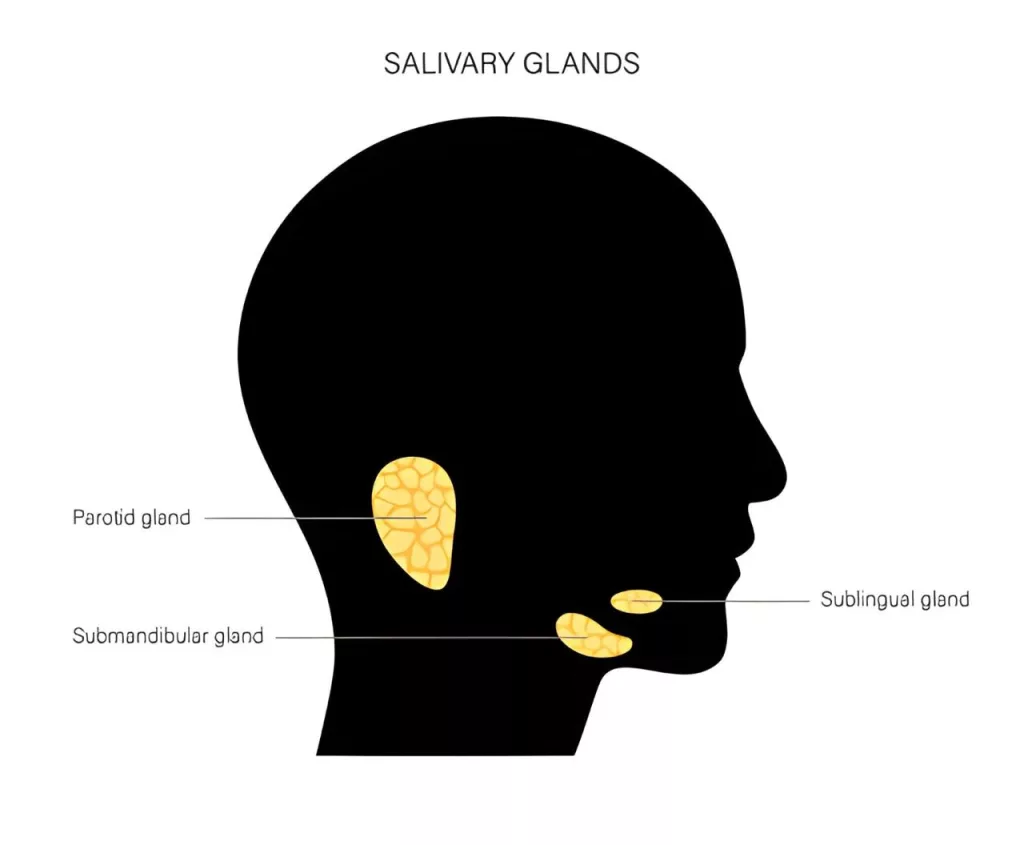
An illustration showing the location of the three major salivary glands, i.e., parotid, submandibular, and sublingual glands, in the mouth.
Causes of Sialadenitis: Sialadenitis Symptoms Diagnosis
There are multiple causes of salivary gland inflammation, including:
1. Reduced Hydration / Salivary Stasis:
Patients who are dehydrated, have poor oral hygiene, are post-operative, or post-radiation are at a higher risk of sialadenitis. Certain medications, including antihistamines, diuretics, beta-blockers, antipsychotics (e.g., clozapine), L-asparaginase, and NSAIDs like phenylbutazone, can reduce salivary flow and increase the risk.
2. Viral Infection:
Certain viruses cause inflammation of the salivary glands. Mumps, caused by the paramyxovirus, is the most common virus that affects the parotid (mainly) and submandibular glands. Other viruses include HIV, coxsackievirus, parainfluenza, cytomegalovirus (CMV), and Epstein-Barr virus (EBV).
3. Bacterial Infection:
Staphylococcus aureus is the most frequent bacterial cause, particularly in acute sialadenitis. Other organisms include Streptococcus pyogenes, Haemophilus influenzae, viridans streptococci, anaerobes, and rarely Mycobacterium tuberculosis (especially in submandibular glands).
4. Sialoliths (Salivary Stones):
Sialoliths or salivary gland calculi/stones cause obstruction of the salivary gland ducts, leading to decreased salivary flow and hence cause inflammation in the glands. The submandibular gland is most commonly affected due to its long, tortuous duct and thicker saliva. Chronic obstruction can require surgical intervention if stones do not pass spontaneously.
5. Auto-immune diseases:
Autoimmune conditions that can cause sialadenitis include Sjögren’s syndrome, sarcoidosis, and granulomatosis with polyangiitis. Sjögren’s syndrome and sarcoidosis are the most common causes of chronic sialadenitis. One well-known form of sarcoidosis is known as Heerfordt’s syndrome, which is characterized by facial nerve palsy, enlargement of the parotid gland, and anterior uveitis (inflammation in the middle layer of the eye).
6. Malignancy:
A tumor can directly affect salivary ducts, or ducts can also be affected by radiation therapy, which leads to inflammation in the salivary glands. Rarely, chronic sialadenitis also undergoes malignant transformation.
7. Idiopathic:
In some patients, there is no specific underlying cause of inflammation in salivary glands, as seen in juvenile recurrent parotitis and chronic sclerosing sialadenitis (Küttner’s tumor). IgG4-related disease is the latest proposed cause of the sialadenitis.
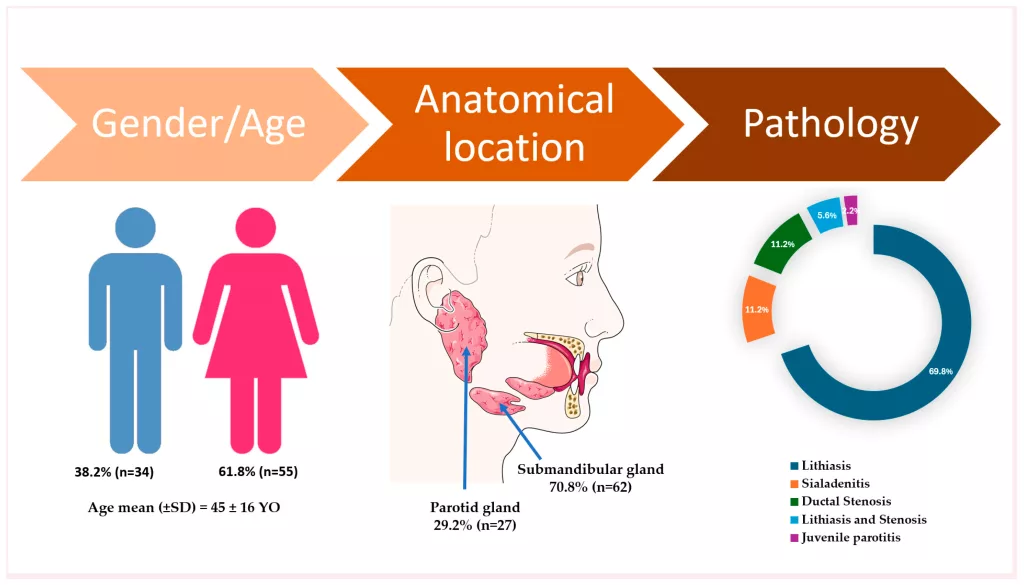
Descriptive data on demographic characteristics, gland involvement, and pathology in the included participants. The artwork used in this figure was adapted from Servier Medical Art (https://smart.servier.com/ accessed on 5 April 2025). Servier Medical Art by Servier is licensed under CC BY 4.0.https://www.mdpi.com/2077-0383/14/11/3938
Types of Sialadenitis:
Sialadenitis can be classified into acute and chronic categories. Acute sialadenitis typically results from bacterial or viral infections, presenting with rapid-onset pain and swelling. Chronic sialadenitis involves recurrent or persistent inflammation, often due to obstruction, such as salivary stones or strictures, and usually presents with swelling but without erythema.
1. Acute Sialadenitis:
Acute sialadenitis is a bacterial inflammation of the salivary gland. It typically affects one major salivary gland, most commonly the parotid, and is common in medically debilitated, hospitalized, or postoperative patients.
Risk Factors for Acute Sialadenitis:
The risk factors for acute sialadenitis include diabetes mellitus, hypothyroidism, renal failure, and Sjögren syndrome. The use of certain medications, especially anticholinergic drugs, can also reduce salivary flow. The most common bacterial cause of acute sialadenitis is Staphylococcus aureus, which has been cultured in 50% to 90% of cases.Streptococcal species and Haemophilus influenzae are also common causes.
Clinical Presentation of Acute Sialadenitis:
Patients with acute sialadenitis typically present with a sudden onset of pain and swelling of the affected gland. Physical examination may reveal induration, edema, redness, and extreme localized tenderness. Massage of the gland may express pus (purulent discharge) from the respective intraoral tissue.
2) Chronic Sialadenitis:
Chronic sialadenitis is characterized by repeated episodes of pain and inflammation caused by decreased salivary flow and salivary stasis. It most often affects the parotid gland.
Risk factors of chronic sialadenitis:
Sialolithiasis and duct strictures impair salivary flow and are more commonly associated with chronic or recurrent infections as compared to bacteria and viruses.
Clinical presentation of chronic sialadenitis:
Patients typically present with recurrent or low-grade swelling and tenderness of the affected gland, especially when eating. A physical examination may initially reveal enlargement of the gland, which may reverse later. Massaging the gland often does not produce visible saliva.
Symptoms of Sialadenitis:
The signs and symptoms of sialadenitis can vary from person to person, but there are some common symptoms as well.
Common Symptoms:
- Pain
- Swelling
- Pyrexia (fever)
- Lymphadenopathy
- Erythema (redness of the affected area)
- Xerostomia (dry mouth)
Specific Symptoms:
- Purulent discharge in bacterial infections
- Intermittent painless unilateral or bilateral swellings without accompanying signs of infection may be idiopathic or due to an underlying condition, such as ductal stenosis or autoimmune disease.
- Chronic sclerosing sialadenitis presents as a painless unilateral swelling that can mimic tumours. A biopsy is required for diagnosis. Airway compromise is an important potential consequence of acute glandular swelling.
Diagnosis of Sialadenitis:
The following steps should be taken to make the diagnosis of Sialadenitis:
History:
History plays a crucial role in evaluating the condition. It should address many factors, including:
- Duration of symptoms (acute vs chronic)
- The number of glands involved
- Discomfort associated with swelling
- Foul taste in the mouth
- Frequency of symptoms
- Aggravating factors (association with meals or salivary stimulants)
- Constitutional symptoms (fever, viral prodrome, weight loss)
- Systemic symptoms (e.g., joint pain, dry eyes, and mouth)
- Medical comorbidities (e.g., alcohol use, diabetes, bulimia, liver disease, autoimmune disease)
- History of radiation treatment
Physical Examination:
A physical exam includes a visual inspection of glands to observe the number of glands involved, erythema of overlying glands, palpation of the gland to note gland size, texture, and tenderness, and massage of the gland to express salivary discharge from the duct orifice and note the type of discharge. A focused cranial nerve exam is necessary to evaluate the facial nerve and trigeminal nerve, particularly the mandibular branch. Additionally, an examination of cervical lymph nodes is required. Fever may also be present.
Important Findings of Physical Examination:
On examination, the gland is swollen, indurated, and tender. Cervical lymphadenitis may be present in cases of infection.
- Chronic or recurrent sialadenitis causes repeated episodes of pain and swelling, often with meals and recurrent infections. Massaging the gland may reveal purulent saliva at the ductal orifice.
- Acute unifocal salivary gland swelling due to obstructive sialadenitis is usually the result of salivary gland stones and/or strictures. It is characterized by intermittent gland swelling occurring with the stimulation of meals.
- Mechanical obstruction of salivary flow within the duct causes swelling of the gland.
- Viral sialadenitis (e.g., mumps) presents with acute multifocal salivary gland swelling accompanied by constitutional symptoms, including fever, headache, malaise, and myalgia.
- Submandibular sialadenosis presents with painless bilateral submandibular enlargement and may be associated with mild discomfort. Approximately 50% of cases are associated with recognized risk factors, including diabetes, metabolic syndrome, alcoholism, bulimia, malnutrition, and liver disease.
Lab Tests and Scans
In addition to history and physical examination, evaluation of sialadenitis requires lab investigations, radiography, biopsy, if indicated, and other tests to rule out autoimmune etiology, including the following:
1. Culture and Sensitivity of Salivary Exudate:
This should be conducted before the initiation of empiric antibiotic therapy.
2. Complete Blood Count:
CBC is essential to rule out infections.
3. Imaging studies:11Abdel Razek AAK, Mukherji S. Imaging of sialadenitis. Neuroradiol J. 2017 Jun;30(3):205-215. [PMC free article] [PubMed] [Reference list]
[Image: CT Scan showing Sialadentis.]
Contrast-enhanced CT showing enlarged, heterogeneously enhancing submandibular gland (large arrow) with surrounding soft-tissue edema (small arrows) involving adjacent neck spaces, consistent with sialadenitis and no visible stone. Image sourced from theJETemarticle “Sialadenitis” by Lauren Sylwanowicz, MD, and Andrew Wong, MD, MBA, used under the Creative Commons CC BY 4.0 license.
- X-ray: This can be useful to detect sialoliths in chronic sialadenitis; around 70% to 80% of submandibular stones are radio-opaque.
- Ultrasonography: This can demonstrate a sialolith (>1 mm) and an abscess cavity, if present.
- Computed tomography scan: This is indicated if conventional plain films are negative or when the clinical presentation is severe and can demonstrate a sialolith. In chronic sclerosing sialadenitis, the salivary gland may be enlarged or atrophic.
- Sialography: Acute inflammation is a relative contraindication; this study can detect sialolith, ductal stricture, and loss of parenchymal integrity if present in chronic sialadenitis.
- Magnetic resonance imaging is warranted if neoplasia is suspected.
- Autoantibodies (anti-Ro/SSA, anti-La/SSB) are tested if autoimmune etiology is suspected.
4. Fine-needle aspiration cytology (FNAC)
Chronic sclerosing sialadenitis can present similarly to a tumor; fine needle aspiration is useful to exclude the presence of a neoplasm.
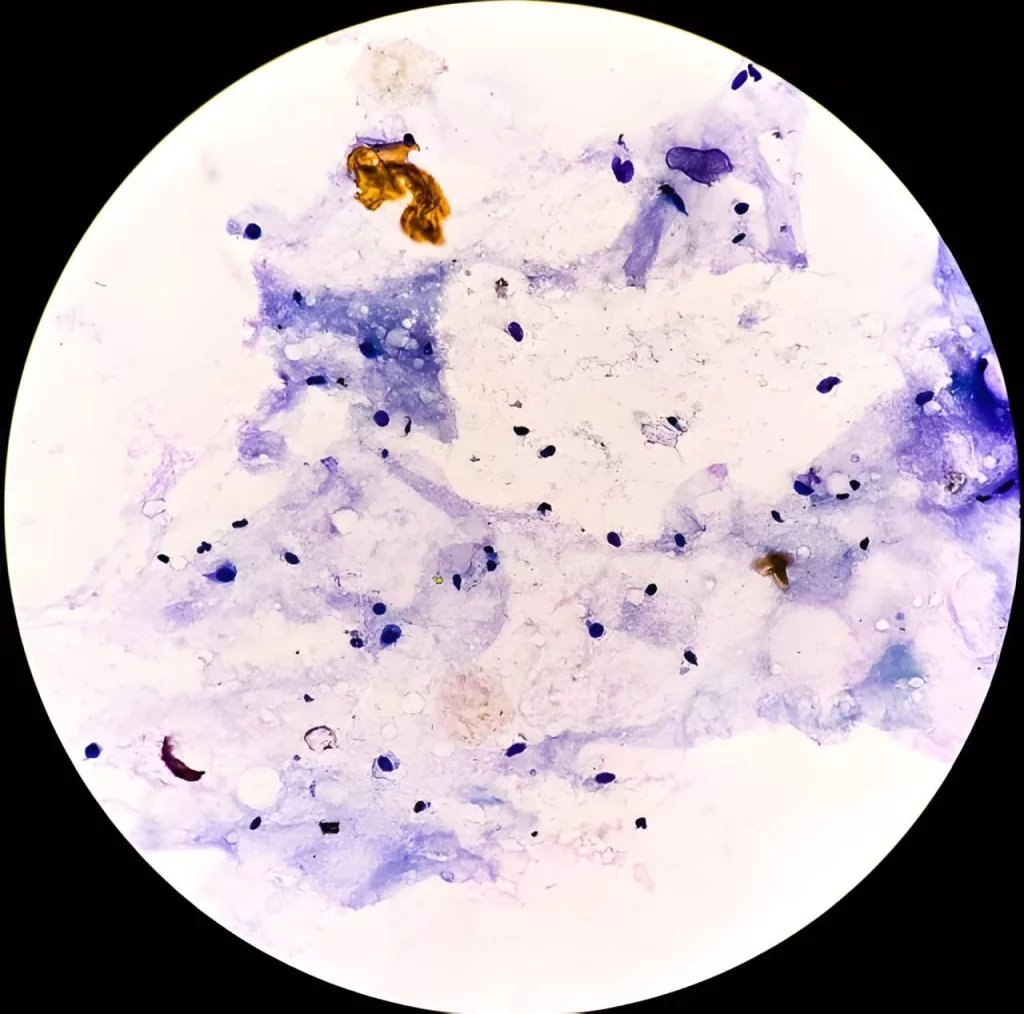
FNAC smear showing blue-stained inflammatory cells with scattered salivary gland epithelial cells in a proteinaceous background, consistent with sialadenitis.
Treatment of Sialadenitis:
The treatment options for sialadenitis depend on whether the condition is acute or chronic. The following are the treatment approaches to both:
Conservative Management
Most cases resolve with remedies like hydration, improving oral hygiene, warm compresses, and massage. Pain can be relieved with analgesics (e.g., nonsteroidal anti-inflammatory drugs), and salivary flow is restored through sialagogues.
Medical Management:
Antibiotics are usually the first line of treatment. Empiric antibiotic therapy starts with amoxicillin/clavulanate or clindamycin. But other antibiotics should be given according to culture and sensitivity reports. In severe cases, IV antibiotics can be given. Corticosteroids can be useful in patients with significant swelling if there is no contraindication.
Surgical Treatment:
In acute suppurative sialadenitis, an abscess is formed, which requires surgical incision and drainage. In the case of sialolithiasis, salivary gland stone removal should occur using interventional sialendoscopy or direct surgical removal. Extracorporeal shock wave lithotripsy, under ultrasonic guidance, is used for intraglandular duct stone removal. Salivary gland excision is recommended if there is recurrent sialadenitis (>3 episodes/year) or chronic sclerosing sialadenitis.
Prognosis:
Sialadenitis is usually more common in adults, irrespective of gender, but infants and the younger age group are more commonly affected by viral infection (mumps). Acute sialadenitis has an excellent prognosis. Most of the acute symptoms resolve in a week, except for edema, which resolves later. Chronic sialadenitis can have multiple relapses, and the prognosis is dependent on the underlying cause. If sialoliths require surgery, the prognosis is good. Symptoms of autoimmune sialadenitis often improve following medical management and treatment of the underlying condition (such as Sjogren’s syndrome).
Complications of Sialadenitis
Sialadenitis is highly treatable; rarely, complications can arise that require proper treatment.
Abscess:
Infection may spread along the spaces in the head and neck region, leading to difficulty in breathing and swallowing, which can be life-threatening and require immediate treatment. Seldom can an abscess affect the floor of the mouth, resulting in Ludwig’s angina.
Spread of Infection:
In severe bacterial sialadenitis, the infection can spread to surrounding tissues, potentially causing cellulitis, septicemia, or systemic infection.
Dental Complications:
As there is reduced saliva production, tooth protection is compromised, leading to increased acidicerosionof tooth enamel, which can cause carious decay of tooth structure.
Post-parotidectomy complications:
Temporary facial nerve palsy occurs in around one-third to two-thirds of patients following superficial parotidectomy. Normally, complete recovery occurs within 3 to 6 months, with permanent palsy occurring in <1%.
Is Sialadenitis Contagious?
Whether sialadenitis is contagious or not depends on its cause.
Contagious Causes:
- Viral infections: Viruses like the one causing mumps are highly contagious.
- Bacterial infections: Bacteria, such as Staphylococcus aureus, can cause sialadenitis and be spread from person to person.
Non-contagious causes:
- Salivary Gland Stones: Also known as sialolithiasis, are not infectious and cannot be passed on.
- Other factors: Other causes, like autoimmune diseases, blockages, poor oral hygiene, dehydration, or radiation therapy, do not make the condition contagious.
Sialadenitis vs.Parotitis:
What is Parotitis or Mumps?
Mumps is the most common cause of non-suppurative acute sialadenitis; 85% of cases occur in children younger than 15 years. The disease is highly contagious and spreads by airborne droplets from salivary, nasal, and urinary secretions. The symptoms of mumps include local pain and edema in the parotid gland region as well as otalgia (earache) and trismus (lockjaw). Most cases are bilateral, although they commonly begin on one side. Diagnosis is confirmed through viral serology. Treatment involves supportive measures, including hydration, oral hygiene, and pain control. Edema typically resolves slowly over time. MMR vaccination, typically completed by the age of 4 to 6, is very useful in preventing the condition at an early age; however, it can occur in the adult age group.
The image shows inflammation of the parotid gland.
Key Differentiating Features of Sialadenitis and Parotitis:
The important features that differentiate sialadentis from parotitis are as follows:
| Feature | Sialadenitis | Parotitis |
|---|---|---|
| Definition | Inflammation of any major or minor salivary gland (parotid, submandibular, sublingual, minor glands) | Inflammation specifically of theparotid gland |
| Glands Involved | Parotid, submandibular, sublingual, or minor salivary glands | Only theparotidgland |
| Etiology (Causes) | Bacterial (Staph aureus), viral, autoimmune (Sjögren), obstructive (stones), dehydration | Viral (most commonlymumps), bacterial, obstruction, autoimmune |
| Most Common Presentation | Painful swelling of theaffected gland, worse with eating if obstructive | Painful swellingin front of the ear and angle of the mandible, may be bilateral (e.g., mumps) |
| Age Group | Any age, depending on the cause | Supportive care for viral, antibiotics for bacterial; hydration; massage |
| Obstruction | Frequently due tosialolithiasis, especially the submandibular gland | Less commonly obstructive than the submandibular gland |
| Clinical Signs | Tender gland, erythema, reduced saliva, may have pus at the duct opening | Parotid swelling, pain, trismus, “ear displacement” outward, erythema |
| Duct Involved | Wharton’s duct (submandibular), Stensen’s duct | AlwaysStensen’s duct |
| Common Pathogens | Staph. aureus (acute), anaerobes, mixed flora; viral (CMV, EBV) | Mumps virus, Staph aureus, anaerobes |
| Complications | Abscess, chronic sialadenitis, duct stricture | Facial nerve involvement (rare), abscess, chronic parotitis |
| Treatment | Hydration, antibiotics (if bacterial), sialagogues, warm compress, stone removal | Supportive care for viral; antibiotics for bacterial; hydration; massage |
Conclusion:
Sialadenitis is a diverse inflammatory condition of the salivary glands, arising from infectious, obstructive, autoimmune, or idiopathic causes. Early recognition is important because timely management, whether through hydration, gland massage, antibiotics, or addressing underlying ductal obstruction, can prevent chronicity and complications such as abscess formation or gland dysfunction. With a proper understanding of the causes and severity of the condition (whether acute or chronic), a comprehensive treatment approach can be taken that ensures effective resolution and preservation of salivary gland function.
References
[1] M., Bruch, Jean (2010). Clinical oral medicine and pathology. Treister, Nathaniel S. New York: Humana Press. ISBN 9781603275200. OCLC 567351700.
[2] Virmani N, Dabholkar J. Primary Tubercular Sialadenitis – A Diagnostic Dilemma. Iran J Otorhinolaryngol. 2019 Jan;31(102):45-50. [PMC free article] [PubMed] [Reference list]
[3] Isacsson, Göran; Lundquist, Per-G. (1 August 1982). “Salivary calculi as an aetiological factor in chronic sialadenitis of the submandibular gland”. Clinical Otolaryngology and Allied Sciences. 7 (4): 231–236. doi:10.1111/j.1365-2273.1982.tb01389.x. ISSN 1365-2273. PMID 7127874.
[4] Gurwale SG, Gore CR, Gulati I, Dey I. Immunoglobulin G4-related chronic sclerosing sialadenitis: An emerging entity. J Oral Maxillofac Pathol. 2020 Feb;24(Suppl 1):S135-S138. [PMC free article] [PubMed] [Reference list]
[5] McQuone SJ. Acute viral and bacterial infections of the salivary glands. Otolaryngol Clin North Am. 1999;32(5):793-811
[6] Brook I, Frazier EH, Thompson DH. Aerobic and anaerobic microbiology of acute suppurative parotitis. Laryngoscope. 1991;101(2):170-172.
[7] Brook I. Diagnosis and management of parotitis. Arch Otolaryngol Head Neck Surg. 1992;118(5):469-471.
[8] Saunders JR, Hirata RM, Jaques DA. Salivary glands. Surg Clin North Am. 1986;66(1):59-81.
[9] Fattahi TT, Lyu PE, Van Sickels JE. Management of acute suppurative parotitis. J Oral Maxillofac Surg. 2002;60:446-448. Abstract
[10] Kraaij S, Karagozoglu KH, Forouzanfar T, et al. Salivary stones: symptoms, aetiology, biochemical composition and treatment. Br Dent J. 2014 Dec 5;217(11):E2
[11] Abdel Razek AAK, Mukherji S. Imaging of sialadenitis. Neuroradiol J. 2017 Jun;30(3):205-215. [PMC free article] [PubMed] [Reference list]
[12] Zhang YY, Hong X, Wang Z, Li W, Su JZ, Chen Y, Gao Y, Yu GY. Diagnostic utility of submandibular and labial salivary gland biopsy in IgG4-related sialadenitis. Clin Rheumatol. 2020 Dec;39(12):3715-3721. [PubMed] [Reference list]
[13] Klinovskaya AS, Gurgenadze AP, Bazikyan EA, Abrahamyan KD, Chunikhin AA. [Sialendoscopy in diagnosis and treatment of salivary gland disorders]. Stomatologiia (Mosk). 2020;99(3):83-86. [PubMed] [Reference list]
[14] Hammett JT, Walker C. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Sep 10, 2024. Sialolithiasis. [PubMed] [Reference list].
[15] McQuone SJ. Acute viral and bacterial infections of the salivary glands. Otolaryngol Clin North Am. 1999;32(5):793-811.