
 is a type of delayed hypersensitivity reaction that manifests about a week or two...){kind=link}

Serum Sickness Like Serum sickness-like reaction (SSLR) is a type of delayed hypersensitivity reaction that manifests about a week or two following exposure to a trigger (usually a drug or viral infection).
The clinical presentation is quite dramatic (abrupt onset of fever, skin rash, and joint pain). However, the actual clinical course is self-limiting and less severe than the name implies.
Though it takes the form of a fever-rash-arthralgia triad characteristic of classical serum sickness, we know that SSLR is a distinctive example of the modern immune response. There are no circulating immune complexes; the complement cascade isn’t activated, and does not progress to organ damage.
Epidemiology & Global Trends: Serum Sickness Like
A serum sickness-like reaction is something that can happen to a person during any period of life, but it generally occurs in children more than in adults. The median age is 3.2 years.
The incidence pattern is largely based on global trends in antibiotic prescription. 0.2–0.5% of beta-lactam antibiotic exposure is seen to result in an SSLR. In some countries (where cephalosporin consumption is currently high), cephalosporin cases still dominate. In other countries (where amoxicillin consumption continues to be high), the reverse is true.
Then there are seasonal patterns. In general, SSLR occurs more in winter: respiratory infections, and thus, antibiotics, are more common. A fraction of cases (5–15%) arise de novo without drug exposure, with the trigger being a viral infection (such as adenovirus, Epstein–Barr virus).
Other than these, SSLR shows no consistent sex difference and no other clustering.
Serum Sickness vs. Serum Sickness-Like Reaction
Although the two share a name and their symptoms look similar, they are fundamentally different. This difference in underlying mechanism is what makes SSLR far less dangerous, even though the clinical presentation can initially appear dramatic.
| Feature | Serum Sickness4Rixe N, Tavarez MM. Serum Sickness. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538312/ | Serum Sickness-Like Reaction |
|---|---|---|
| Immune complexes | Present | Absent |
| Complement levels (C3, C4) | Low | Normal |
| Common triggers | Animal-derived antiserum, monoclonal antibodies | Antibiotics, infections, NSAIDs |
| Onset after exposure | 7–10 days | 7–14 days |
| Organ involvement | Possible (kidneys, vessels) | Not expected |
| Severity | Can be serious | Generally mild/moderate |
| Treatment | Stop trigger, supportive | Stop trigger, supportive |
It’s important for the modern clinician to be able to recognize these differences. It not only prevents unnecessary alarm, but also ensures that patients with SSLR receive the management they need.
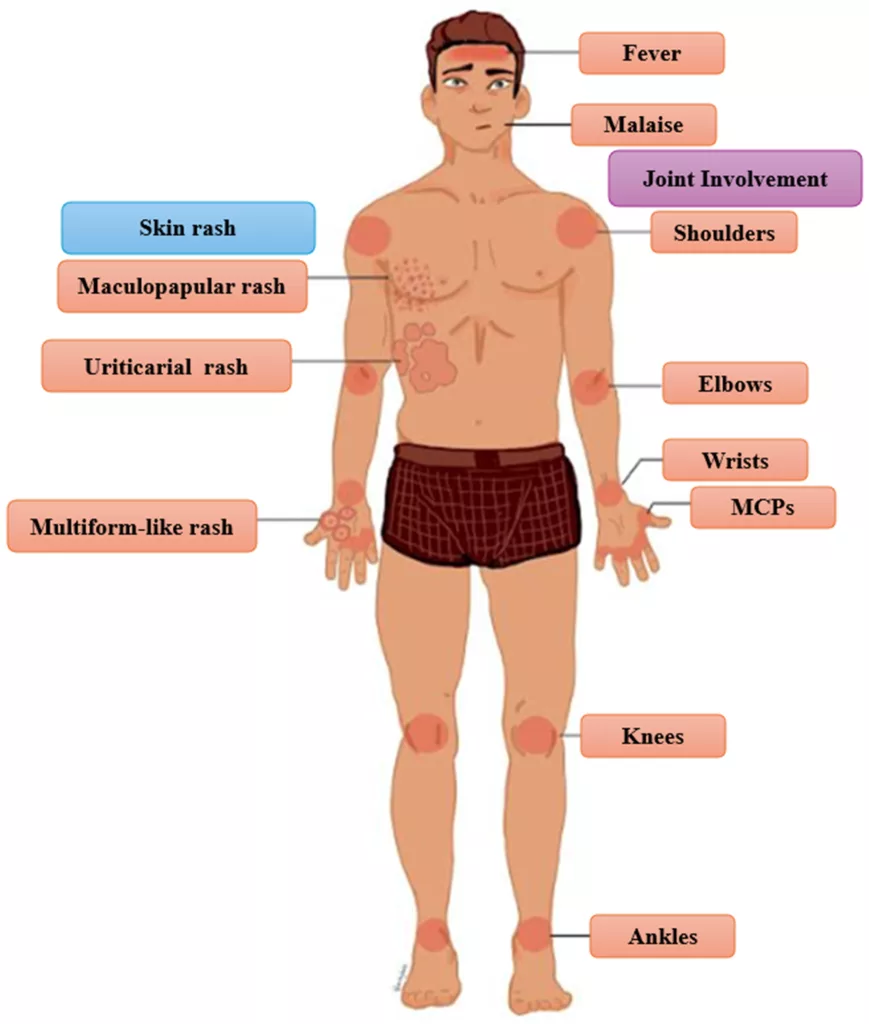
Key clinical features often seen in serum sickness-like reaction: the classic triad, typical rash pattern, and associated joint findings. (Image courtesy: Chatzigrigoriadis, C., Koufopoulos, E., Avramidis, P., Erginousakis, I., Karakoida, V., Papadopoulos, T., Sperdouli, D., Tachliabouri, M., Vilanakis, K., Zampounidis, D., Michou, V., Eskitzis, P., Galiatsatos, P., Lavasidis, L., & Anestakis, D. (2025). Serum Sickness-Like Reaction: A Narrative Review of Epidemiology, Immunopathogenesis, Diagnostic Challenges, and Therapeutic Approaches. Clinics and Practice, 15(10), 178. Available fromMDPI, licensed under CC by 4.0)
Causes of Serum Sickness-Like Reaction
The cause is exposure to a trigger that temporarily disrupts the immune system’s balance. The most frequent of these triggers include:
1. Medications
This still remains the leading cause, especially those to which children are exposed. These are:
- Antibiotics like Cefaclor, Amoxicillin, Cefprozil, and other beta-lactams
- NSAIDs (ibuprofen, naproxen)
- Some anticonvulsants (carbamazepine, lamotrigine)
Cefaclor has been historically reported as the major cause in children. The interesting part is that the rates of Cefaclor-triggered SSLR have decreased worldwide in correlation with its usage, since its prescription has decreased. But now, amoxicillin-induced SSLR has risen, indicating that amoxicillin is now being overprescribed.
2. Recent Infections
A smaller subset of SSLR is not triggered by medications, but by infections:
- Viral infections like adenovirus, Epstein–Barr virus, and enteroviruses
- Bacterial infections like Group A streptococcus and Mycoplasma pneumoniae
These infection-related cases behave clinically just like drug-triggered SSLR.
3. Vaccinations
SSLR post-vaccine is extremely rare and usually mild. There are only a few one-off instances, and no definite pattern of cause has been established. Also, when it comes to the COVID-19 vaccine, studies have still not been able to establish any significant relation.
Risk Factors
Risk factors include:
- A previous episode involving the same drug
- Frequent exposure to antibiotics
- Long-lasting viral infections
- Genetic predisposition to drug hypersensitivity
According to recent population-based estimates, SSLR affects 0.2 to 0.5 percent of children who are exposed to these high-risk medications.

Erythematous macular lesions over the lower limbs, documented in a reported case of serum sickness-like reaction associated with acute hepatitis B infection. (Image Courtesy: Gupta R, Fakunle I, Samji V, et al. (April 28, 2021) Serum Sickness-Like Reaction Associated With Acute Hepatitis B in a Previously Vaccinated Adult Male. Cureus 13(4): e14742. Available fromCureusand licensed under CC by 4.0)
Why and How Serum Sickness-Like Reaction Develops
Once you are exposed to a trigger, serum sickness-like reaction develops through immune pathways akin to classical hypersensitivity, but it’s very important to keep in mind that it does not form immune complexes or activate the complement cascade. Based on the cause, there might be a few possible mechanisms:
- Some drugs (often beta-lactam antibiotics) will metabolize to a reactive intermediate, which will then covalently bind to proteins. These modified proteins will act like new antigens (haptens), which activate T cells and cause a delayed immune response.
- In some, exposure to a drug or viral antigen causes a short-lived burst of cytokine activity. This creates the classic fever, rash, and joint pain picture. The symptoms last only as long as the stimulus is present, and the response rectifies itself as soon as the stimulus is stopped.
- Recovering from an infection, the immune system sometimes overshoots. Instead of returning to baseline, certain inflammatory pathways remain overactive, producing SSLR-like symptoms even in the absence of drug-based triggers. This is not because of the infection itself, but because of the immune system’s transitional state afterward.
Symptoms of Serum Sickness-Like Reaction
Symptoms usually begin a week or two after exposure, but may appear sooner (as early as 5 days) in case of repeat exposures. The timing is consistent enough that experienced clinicians often suspect SSLR before clinical testing even begins.
The Classic Triad
- Rash
- Joint swelling or pain
- Fever
Rash Characteristics
The rash is often the first visible sign. It may begin on the trunk or limbs and spread outward. It can look:
- Hive-like
- Morbilliform (measles-like)
- or a mix of raised and flat lesions
What distinguishes SSLR from ordinary urticaria is persistence. The lesions stay in place for hours, even days, rather than appearing and disappearing rapidly like typical hives. Many patients describe intense itching, but not all.
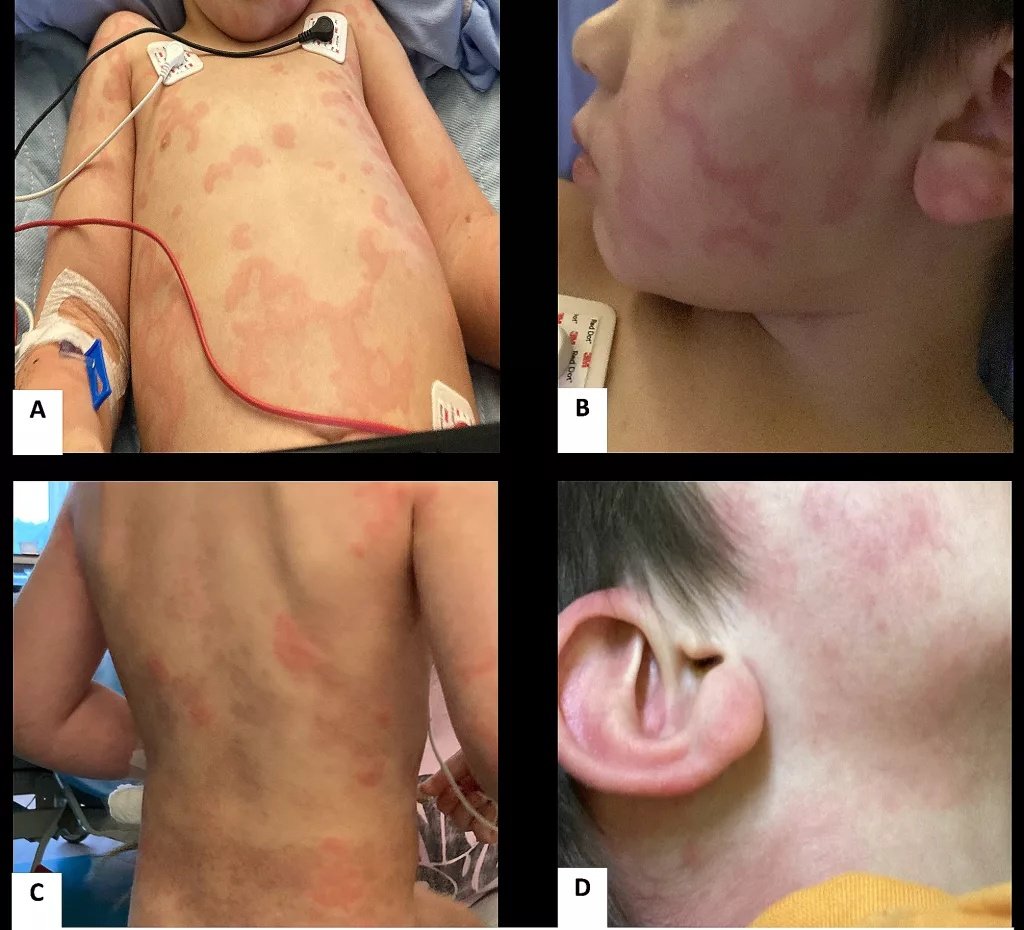
Scattered red, itchy papular lesions involving the torso, upper limbs (A), cheeks and sides of the neck (B, D), as well as the back (C). (Image courtesy: Bakshi, D., Tang, X. & Waserman, S. A case of pediatric serum sickness-like reaction (SSLR) after a 2-month re-exposure to amoxicillin. Allergy Asthma Clin Immunol 20, 29 (2024). Available fromSpringerand licensed under CC by 4.0)
Joint Symptoms
Joint pain follows closely, often accompanied by swelling and stiffness. The knees, ankles, wrists, and elbows are the usual sites. The pain may be:
- Symmetrical in large joints (knees, ankles, elbows)
- Migratory
- Or simply persistent in a few large joints
Morning stiffness is common, but unlike autoimmune arthritis, the swelling resolves completely without joint damage.
Fever and Systemic Features
Fever can be present, but is usually low to moderate grade. High fever suggests an alternative diagnosis. Some systemic symptoms may also be present in the patient:
- Fatigue
- Headache
- Facial swelling
- Swollen lymph nodes
- Mild gastrointestinal discomfort
Despite the theatrical presentation, the internal physiology remains stable. There is no renal involvement, no vasculitis, no GI bleeding, and no mucous membrane involvement, all features that would point firmly away from SSLR and toward more dangerous conditions such as Kawasaki disease, MIS-C, Stevens–Johnson syndrome, or IgA vasculitis.
Diagnosis of Serum Sickness-Like Reaction
Diagnosis begins with a good history, including the timing of medications, any recent infections, the onset of symptoms, and patterns of the rash and joint pain. But laboratory investigations help rule out more serious conditions.
1. Complete Blood Count (CBC)
CBC usually doesn’t reveal anything too drastic; the findings are only subtle:
- Mild leukocytosis
- Sometimes eosinophilia
- Normal platelets or mildly elevated levels
Naturally, these results reflect inflammation, not organ dysfunction.
2. ESR and CRP
Since these are both inflammatory markers, they may be elevated, though not dramatically. Extreme elevations should signal evaluation for Kawasaki disease, MIS-C, or bacterial infection.
3. Complement Levels
Complement testing (C3, C4, and CH50) is the most important differentiator in diagnosis.
- Normal complement levels suggest SSLR
- Low complement levels raise suspicion for true serum sickness
4. Urinalysis for Renal Evaluation
A simple urinalysis can rule out glomerular involvement. SSLR nearly always has:
- No hematuria
- No proteinuria
- And no urinary abnormalities
If these are present, clinicians must consider vasculitis or immune complex disease, as in true serum sickness.
5. Imaging Studies
Radiographic studies are rarely needed unless the clinician notices some significant joint involvement. As opposed to autoimmune arthritis, in this case, imaging shows no erosions or synovitis.
Differential Diagnosis
Serum sickness-like reaction can resemble other pediatric and adult illnesses. Here are some key differential points and alternative diagnoses:
| Features | Differential Diagnosis |
|---|---|
| Mouth, eye, or genital sores | Stevens–Johnson syndrome (SJS/TEN) or Kawasaki disease |
| Very high fever or multiple organs affected | MIS-C (a post–COVID inflammatory condition)8Lee, P. I., & Hsueh, P. R. (2023). Multisystem inflammatory syndrome in children: A dysregulated autoimmune disorder following COVID-19. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi, 56(2), 236–245. https://doi.org/10.1016/j.jmii.2023.01.001 |
| A purple, palpable, bruise-like rash | IgA vasculitis (Henoch–Schönlein purpura) |
| Migrating joint pain with heart-related symptoms | Acute rheumatic fever |
Treatment of Serum Sickness-Like Reaction
SSLR is quite self-resolving and predictable, so the overall management is quite simple. Once the diagnosis of SSLR is made, the best thing to do is to remove the triggers completely.
1. Remove the Trigger
The symptoms start to decrease within 24-48 hours once the trigger is removed. For example, in drug-induced SSLR, discontinuation of the drug leads to spontaneous cure.
2. Anti-histamines
These medications ease rash and itching by blocking histamine at H1 receptors. Modern second-generation antihistamines: cetirizine, loratadine, and fexofenadine offer symptom relief without sedation. These will also help reduce facial swelling.
3. NSAIDs for Joint Pain
NSAIDs are important in lowering inflammation and joint pain (arthralgia). They do this by inhibiting COX-mediated prostaglandin release. For most patients, Ibuprofen or naproxen is advised. The only exception would be if the clinician suspects it was triggered by an NSAID itself, in which case, NSAIDs have to be avoided completely.
4. Corticosteroid Therapy
If NSAIDs aren’t enough, which might be the case in moderate or severe levels of disease, short courses of oral corticosteroids can be given. They block cytokine release and T-cell activation, so the patient will get early relief from fever and joint swelling. Dosage is 0.5-1 mg/kg/day of Prednisolone, for 3-5days, after that tapered off.
5. Supportive Measures
The immune system will ultimately correct itself. In the meantime, hydration, cool compresses, and skin barrier creams help the patient feel better. But even these are really overkill. Most patients recover fine at home. However, a deterioration in clinical status is a clear sign that the diagnosis needs to be reconsidered.
Serum Sickness-Like Reaction Recovery
As long as the causative agent is removed, SSLR is, for the most part, a self-limited illness. The fever usually resolves within 48 hours, and the rash usually fades over 3-5 days. Itching (pruritus) can be treated with oral antihistamines.
In general, the illness spontaneously resolves over 1-2 weeks, though joint pain may even take 2-6 weeks to resolve. Children may appear uncomfortable, but the condition does not cause chronic disease, does not evolve into autoimmune illness, and does not damage joints or kidneys.
Prognosis
The prognosis is excellent because the immune system corrects itself as soon as the cause is removed. In terms of long-term consequences, the only thing worth noting is the need to avoid the triggering medication.
Prevention
The clinician must:
- Permanently avoid the offending agent
- Clearly document the reaction as SSLR in the medical records
- Avoid high-risk antibiotics when a suitable alternative exists
- Consider an appropriate alternative agent if possible, especially in patients with SSLR beta-lactam
No desensitization protocols exist for SSLR because the mechanism does not behave like classic IgE-mediated allergy.
Final Word
Serum sickness-like reaction is a new medical condition with an old name. It looks scary, rash, fever, joint swelling, but it’s really not as dangerous once you diagnose it. And while it has a similar name, it bears little resemblance in terms of mechanism or clinical course to classical serum sickness. Remove the offending medication, support the patient, and they will recover fully without long-term problems.
Making the distinction between serum sickness vs. serum sickness-like reaction allows us to better reassure patients, avoid unnecessary alarm, and help guide safe future prescribing.
References
[1] Del Pozzo-Magaña, B. R., Abuzgaia, A., Murray, B., Rieder, M. J., & Lazo-Langner, A. (2021). Paediatric serum sickness-like reaction: A 10-year retrospective cohort study. Paediatrics & child health, 26(7), 428–435. https://doi.org/10.1093/pch/pxab003
[2] Elzagallaai, A. A., Abuzgaia, A. M., R., B., Loubani, E., & Rieder, M. J. (2022). The role of in vitro testing in pharmacovigilance for ß-lactam-induced serum sickness-like reaction: A pilot study. Frontiers in Pharmacology, 13, 945545. https://doi.org/10.3389/fphar.2022.945545
[3] Ivanchikov V.V., Murashkin N.N., Ambarchian E.T., Kuzminova A.D. Serum Sickness-Like Reaction Associated with Epstein – Barr Virus: Clinical Case. Current Pediatrics. 2022;21(5):391-399. (In Russ.) https://doi.org/10.15690/vsp.v21i5.2455
[4] Rixe N, Tavarez MM. Serum Sickness. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538312/
[5] Bakshi, D., Tang, X., & Waserman, S. (2024). A case of pediatric serum sickness like reaction (SSLR) after a 2-month re-exposure to amoxicillin. Allergy, asthma, and clinical immunology : official journal of the Canadian Society of Allergy and Clinical Immunology, 20(1), 29. https://doi.org/10.1186/s13223-024-00887-7
[6] Norton, A. E., Risma, K., & Ben-Shoshan, M. (2025). Serum Sickness–Like Reactions in Children—Is Lifelong Avoidance Indicated? The Journal of Allergy and Clinical Immunology: In Practice, 13(5), 969-977. https://doi.org/10.1016/j.jaip.2025.01.041
[7] Khalaf, R., Choi, U., Prosty, C., & Ben-Shoshan, M. (2025). Serum Sickness-Like Reactions Clinical Characteristics and Management: A Systematic Review. The Journal of Allergy and Clinical Immunology: In Practice, 13(5), 1068-1074. https://doi.org/10.1016/j.jaip.2025.02.027
[8] Lee, P. I., & Hsueh, P. R. (2023). Multisystem inflammatory syndrome in children: A dysregulated autoimmune disorder following COVID-19. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi, 56(2), 236–245. https://doi.org/10.1016/j.jmii.2023.01.001
[9] Philpot E. E. (2000). Safety of second generation antihistamines. Allergy and asthma proceedings, 21(1), 15–20. https://doi.org/10.2500/108854100778249033