
 with a cutoff point <120°...){kind=link}

Coxa Vara Hip Coxa Vara is a pathological decrease in the neck-shaft angle of the femur (angle of inclination) with a cutoff point <120°. Angle of inclination is 150° at birth, and it gradually decreases to 125 to 135° at the time of skeletal maturity in adults. If it decreases much further than this angle, then the femoral neck becomes horizontally oriented, termed as Coxa Vara (or Coxa Varus). It causes limping, shortening of the limb, pain, severe difficulty in walking, and, if not managed properly, it can lead to degenerative changes.
Even minor changes in the angle can have a mechanical multiplier effect on the entire limb because the femur is associated with the development of the hip joint and also dictates the mechanics of weight transmission to the knee. The problem spectrum may extend from asymptomatic radiographic alteration to obvious functional impairment.
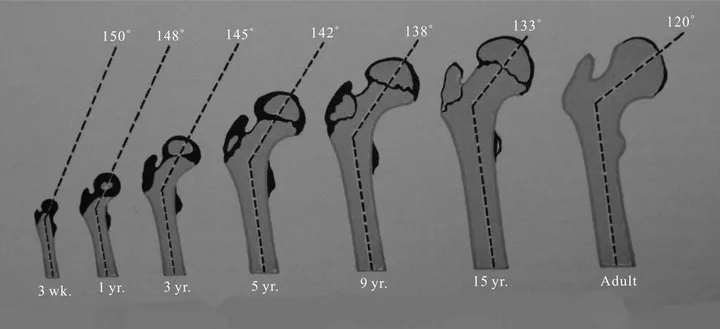
Normal femoral neck–shaft angle (angle of inclination) according to age group, illustrating how the angle decreases as skeletal maturity (Image Courtesy: Reproduced from M. B. Dobbs and J. A. Morcuende, “Other Condition of the Hip,” In: W. W. Lowell and R. B. Winter, Ed., Pediatric Orthopedics, Philadelphia, London, New York, J.B. Lippincott Company, 1986, pp. 1126-1148. Available fromSCIRP. Licensed under CC by 4.0)
Epidemiology: Coxa Vara Hip
Coxa vara is rare, particularly congenital coxa vara. The incidence of congenital coxa vara is approximately 1 per 25,000 births, according to the literature. It is a disorder that is more common among females, with a female-to-male ratio of 2:1. Almost one-half (30-50%) of all cases are bilateral, the rest affect one side only.
Congenital coxa vara presents in early childhood (age 1-6 years). Acquired coxa vara may present at a later age, depending on the cause. Trauma, infections, and metabolic diseases are common causes of coxa vara in the first decade of life, while metabolic causes are more common during periods of rapid growth of the skeleton in early childhood.
Since the incidence of acquired coxa vara is influenced by geographic factors, coxa vara is seen to be more common in some regions than others. This relationship is particularly true if the causative factors of coxa vara (e.g., poor nutritional and health status of the population) are more prevalent. An increased prevalence of orthopedic diseases may be seen in regions in which a nutritional deficiency state (e.g., Vitamin D deficiency or calcium deficit, which results in a higher prevalence of rickets) and other pediatric diseases (infectious and metabolic diseases) are widespread.
Mechanism of Varus Deformity
The femur is a long bone; its proximal end functions as a lever system, with the femoral head transmitting weight through the hip joint, and the hip abductors (mostly the gluteus medius and minimus) pull on the greater trochanter in order to stabilize the pelvis while walking.
In a normal hip, the neck-shaft angle is around 125–135°. This angle is crucial for the abductors to balance the weight when standing on one leg (Trendelenburg mechanism).
When coxa vara is present, the neck-shaft angle is reduced, so the femoral neck becomes shorter and positioned more horizontally. This has two biomechanical consequences:
- The lever arm on which the abductors work is shortened, meaning they must now work much harder to keep the pelvis level.
- Shear forces are generated on the upper part of the femoral neck, especially near the physis (growth plate), in children.
This means that each and every step causes excessive forces to act on an already weakened zone.
Especially in developmental coxa vara, where the bony tissue is still immature, the neck is unable to cope with these forces. Over time, it yields; with each step, the deformity gets worse, the neck shortens, and the angle reduces even more.
This is a vicious cycle that can only be stopped through bone realignment, typically with a valgus osteotomy.
Types & Causes of Coxa Vara
Coxa vara isn’t a single disease. It’s a radiographic and clinical endpoint that can be caused by a lot of other conditions. In general pediatric orthopedics, we commonly see 3 types:
- Congenital Coxa Vara: an abnormality present at the time of birth related to how the cartilage in the femoral neck developed.
- Developmental Coxa Vara: the most classic pediatric form, occurring between 1–6 years of age. Hypothesized to be the result of failure in primary endochondral ossification at the femoral neck base.
- Acquired Coxa Vara: appears later after fractures, infection, or in patients with metabolic bone disease (e.g, rickets, fibrous dysplasia).
Since the net mechanical effect is the same (decreased angle, inefficient abductor mechanics), the clinical manifestation can be the same. However, the treatment strategy is highly dependent on what is causing the coxa vara and the age of the patient.
Coxa Vara vs. Coxa Valga
Both are pathologic abnormalities of the femoral neck–shaft angle, but coxa vara is the exact opposite of coxa valga.
- In coxa vara, the angle is abnormally low, the femoral neck becomes more horizontal, and the trochanter is higher. This shortens the limb and makes the abductor lever arm shorter and more horizontal, putting more force on the femoral neck and causing limp and instability.
- In coxa valga, the angle is higher (>135°), the neck points upwards, creating a more vertical femur. The limb appears longer, but causes the acetabulum to be incompletely covered, which increases susceptibility for hip dislocation. There is also increased stress on the acetabulum.
In short, vara reduces power, valga reduces stability, and both disturb the lever biomechanics of keeping the pelvis level during the gait cycle. The clinical utility of this comparison is to help visualize correction angles in surgery as well as recognizing where an overcorrection is likely in a valgus osteotomy to push the hip from varus to valgus.
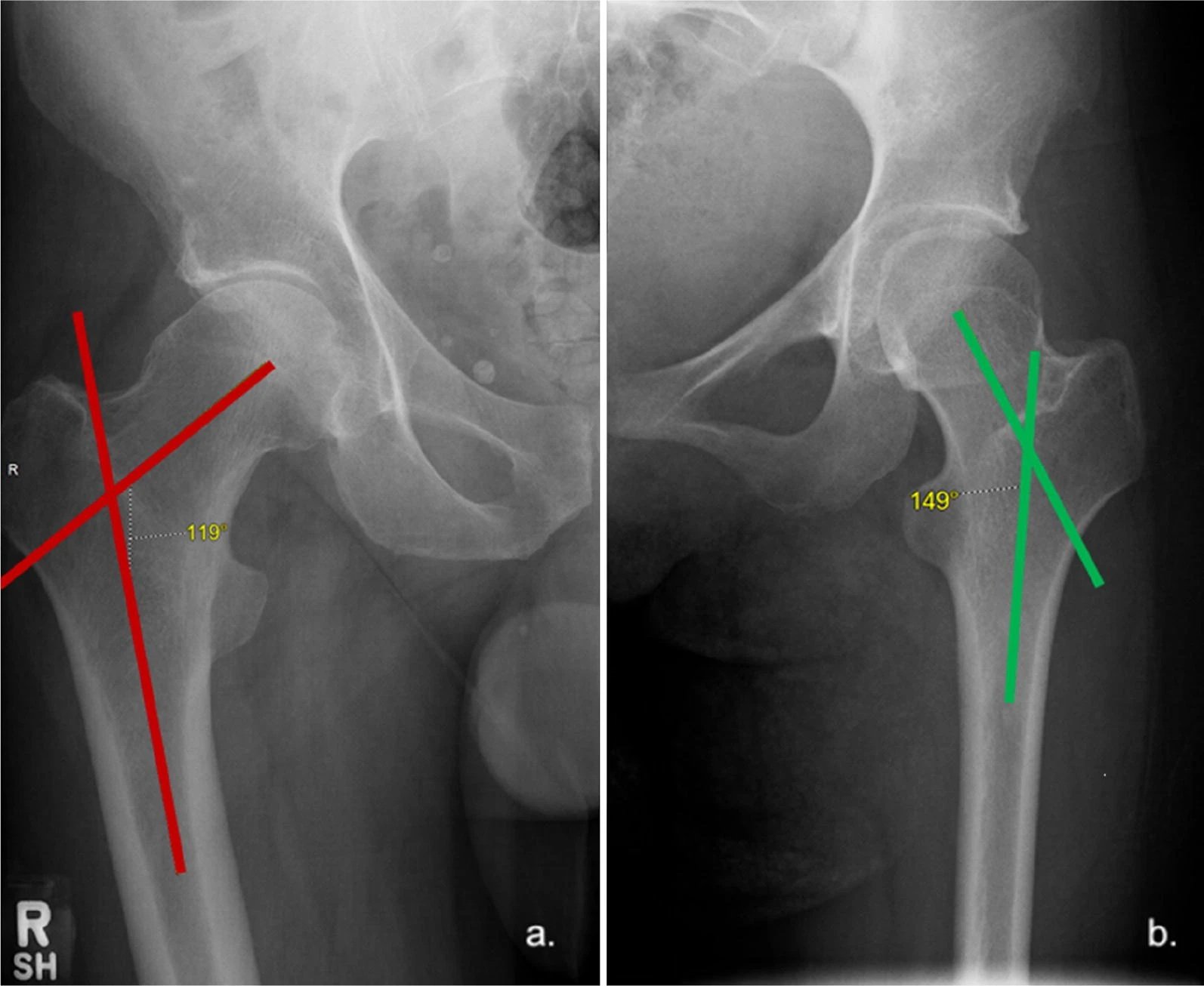
Neck-shaft angles as displayed on pelvic radiographs: On the right side (red angle), the measurement is 119°, indicating coxa vara, whereas on the left side (green angle), the angle measures 149°, indicating coxa valga (Image Courtesy: Popat, R., Lee, S., George, D.A. et al. Assessment of the young adult hip joint using plain radiographs. Musculoskelet Surg 104, 245–255 (2020). Available fromSpringer. Licensed under CC by 4.0)
Clinical Features of Coxa Vara
Symptoms:
Pain
Most children don’t complain of pain early on. But in acquired types, pain is often the presenting symptom. Patients describe mechanical hip or groin pain, which is made worse by activity. The pain is localized to the affected hip, and at times it can radiate down to the thigh or the knee.
Abnormal Gait & Leg Length Discrepancy
Because the hip is involved, the earliest manifestation of developmental coxa vara is often a painless limp. Parents might notice that one leg seems shorter or that the child appears to be swaying to one side when walking, the characteristic Trendelenburg gait.
Limited Function
As the deformity gets worse, it consequently limits the mobility of the hip. Children may find it hard to run properly or climb stairs, or take part in athletic sports. Adults report difficulty with walking for long distances, standing for too long, or activities where they have to stand on one leg for too long.
Physical Examination Findings:
On examination, the gait and range of motion abnormalities are usually diagnostic:
- True limb-length discrepancy
- Hip held in slight abduction and external rotation to increase femoral head coverage
- A high-riding greater trochanter, which can be palpated during examination
- Compensatory scoliosis with convexity toward the affected side
- Limited abduction and internal rotation of the hip
- Wasting of abductors and thigh muscles in chronic cases
- A positive Trendelenburg sign: when the patient stands on the affected leg, the pelvis drops toward the other side, indicating weakness or mechanical insufficiency of the hip abductors
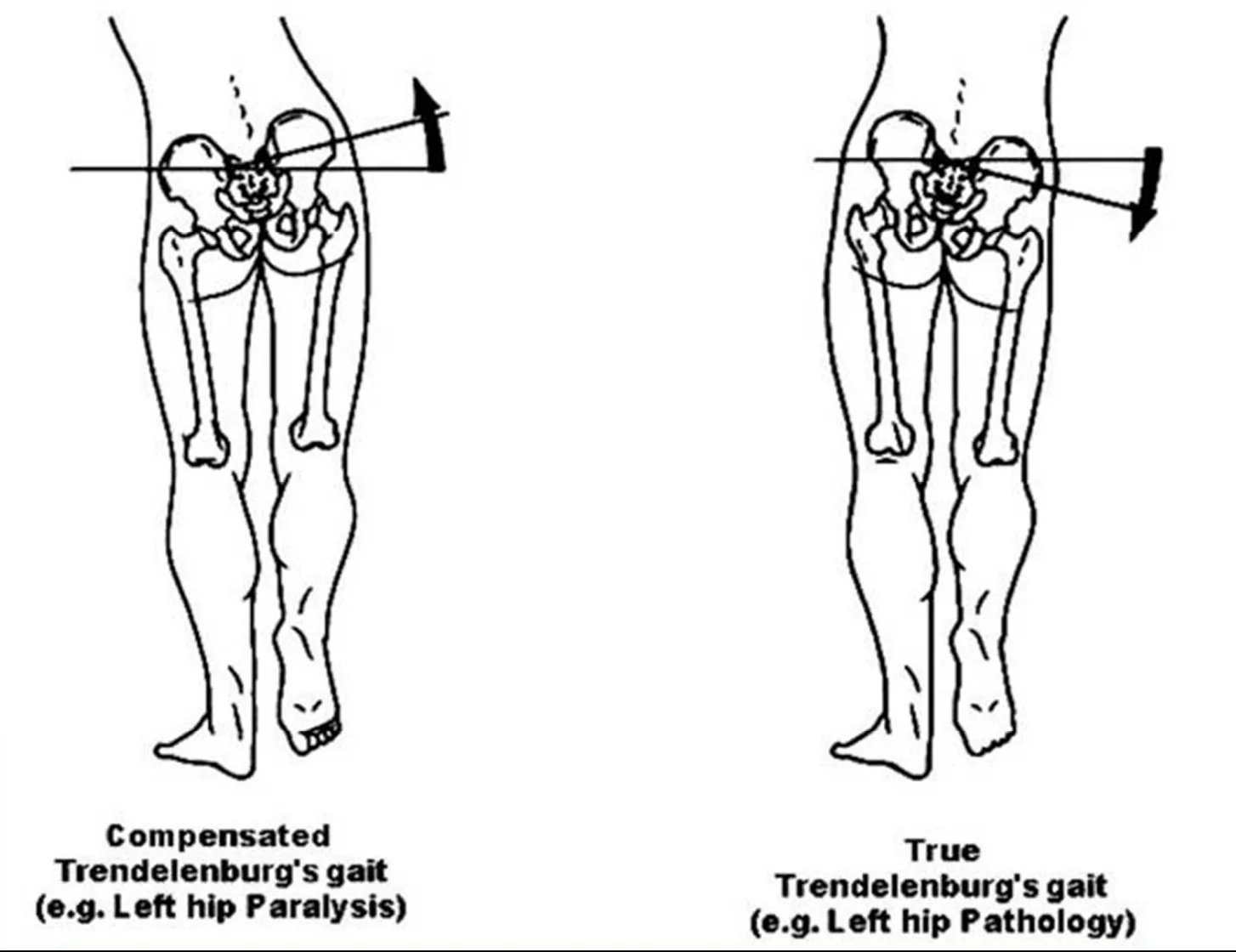
Illustration of True and Compensated Trendelenburg’s sign: In the true Trendelenburg gait (left), weakness of the hip abductor muscles causes the pelvis to drop on the opposite side during stance. On the other hand, in the compensated form (right), the patient leans the trunk toward the affected side to maintain balance and reduce pelvic tilt. (Image Courtesy: Ganesh Elumalai, Ameet Kumar Jha, Palani Kanagarajan, Sanjoy Sanyal. (2016). Soccer Syndrome – 3: Common Sacral Malalignments and Its Manual Diagnostic Techniques. American Journal of Sports Science, 4(2), 25-37. Available fromResearch Gate. Licensed under CC by 4.0)
Radiology & Diagnosis of Coxa Vara
History is usually irrelevant, except in acquired cases, where there is usually a more acute history of a fracture, infection, or a bone condition, for example, Vit D deficiency.
X-Ray Imaging
Diagnosis is simple and starts with an X-ray: an AP pelvis and a frog leg lateral view. Two angles are measured to help diagnose:
- The neck-shaft angle (angle of inclination) less than 120° confirms the neck is in varus alignment (<110° in some pediatric cases)
- The Hilgenreiner-epiphyseal angle (HE angle) describes how tilted the growth plate is. An HE angle above 25° indicates deformity, while values over 45° suggest progressive coxa vara, and angles beyond 60° almost always worsen without surgical correction.
A hallmark X-ray sign in developmental cases is a triangular defect on the inner femoral neck, a classic clue in developmental cases. It’s a small triangular inferior metaphyseal fragment.
Other Imaging Tests:
Cross-sectional imaging (CT or MRI) is not mandatory for diagnosis. Instead, their utility is to assess in preoperative planning. MRI may also be used to assess the growth plate, detect avascular necrosis, or identify fibrous dysplasia, tumors, etc, in patients presenting with hip pain.
Bone scan or SPECT has no role in diagnosis, can be used in selected cases mainly to differentiate an active fibrous dysplasia from other lesions, or to assess metabolic activity in cases where diagnosis is not clear.

X-ray of a seven-year-old with congenital femoral deficiency and coxa vara: The left femur is visibly shorter, with the knee joint sitting higher as a result (yellow circle), and the red arrow points to the normal right femur for comparison. (Image Courtesy: Bagga I B, Raghuveer R, Singh S (March 06, 2024) Physical Therapy Interventions: A Case Report of Building Strength, Confidence, and Mobility in a Seven-Year-Old With Congenital Femoral Deficiency With Coxa Vara. Cureus 16(3): e55662. Available fromCureus. Licensed under CC by 4.0)
Treatment Options & Principles
Observation:
Most of the progressive deformities need surgical correction; however, some of the mild, non-progressive cases can be managed by just observation and physiotherapy. It’s important to remember that observation is only safe for smaller-sized, non-progressive deformities, with normal HE angles and mild NSA (Neck-Shaft Angle) changes. Even in these cases, clinical examination every 3 months and radiography every 6 months is the protocol. If the HE angle rises or gait disturbances develop, surgery should be done.
The key indicators for surgery are:
- Progressive deformity on serial X-rays (increasing HE angle, decreasing NSA)
- Functional limitation or leg-length discrepancy
- Marked decrease in angle (<110°)
- Associated pathologies (malunited fracture, post-infection deformity, significant pain)
Conservative Management:
Conservative measures have limited roles and are largely supportive: activity modification, analgesia, physical therapy to strengthen abductors, and close radiographic follow-up for borderline cases. In acquired cases where pain is from inflammation rather than structural deformity, targeted treatment of the cause is primary. This stands true for metabolic causes like nutritional rickets as well.
Surgical Correction:
The purpose is to restore normal hip mechanics: return varus to planned alignment; optimize the HE angle; correct leg length to match the normal side; and also to prevent degeneration long-term.
For most correctable cases, the appropriate surgery is a valgus proximal femoral osteotomy (PFO). This involves osteotomy of the proximal femur and then fixing it to the proper angle using a plate or screws, or some combination thereof.
The target is to obtain a neck-shaft angle of 125° and the HE angle below 35°.
Different fixation options exist: blade plates, screws, hip plates, and even external fixation in some situations. Moreover, the osteotomy can be either intertrochanteric or subtrochanteric, depending on anatomy and the surgeon. There is no one right answer.
The principles are the same:
- Normalize the HE and NSA angles enough that the tilt doesn’t happen again. Undercorrecting the tilt will make recurrence more likely.
- Strengthen the abductor lever arm
- Center the femoral head in the socket
Post-op focuses on rehab for abductor strengthening and ambulation. Most kids do great, with improved biomechanics, limp, and leg length.
But under-correction or misalignment can lead to recurrence of the tilt, so calculated surgical planning and follow-up X-rays matter.
Alternative Surgical Approaches:
- In selected complex or recurrent cases, especially older children or those with multiplanar deformity, more sophisticated three-dimensional planning, corrective osteotomies in multiple planes, or even guided growth techniques may be used. Total hip replacement for secondary osteoarthritis may be needed in adult patients.
Outcomes & Complications
If a patient has appropriate correction of the HE angle and secure fixation, the results are normally excellent. Children recover near-normal gait and mobility, pain disappears, and limb length also improves.
Possible complications:
- Undercorrection may cause the deformity to return
- Over-correction shifts the hip to Coxa Valga.
- Hardware irritability, infection, non-union, or persistent leg-length difference.
- Later (2-10 years), the concern is early degenerative change if the hip biomechanics remain abnormal.
That’s why surgeons stress upon calculated angle correction as well as long-term follow-up.
Prognosis & Prevention
For developmental cases, the long-term outlook is excellent for most children as long as coxa vara is identified early and proper treatment is administered before the hip joint degenerates. However, left untreated, it can become much worse. Recurrence is most likely if the HE angle remains above 45° after correction.
There is no known way to prevent congenital and developmental coxa vara. Acquired forms can be minimized if optimal bone health is maintained through good nutrition, treatment of hip infections on time, and careful management of pediatric proximal femur fractures.
Conclusion
Coxa vara is a group of conditions with a lower-than-normal femoral neck-shaft angle. Even this small angular deformity has a dramatic effect on gait and range of motion. Manifestation ranges from a simple painless limp to visible limb shortening and sometimes early joint degeneration.
However, otherwise healthy children with coxa vara can regain normal gait and hip function with early diagnosis and proper planning of surgery. Regular follow-up, physiotherapy, and good bone nutrition after successful planned surgery can all help maintain hip alignment and prevent recurrence. However, for adult survivors with severe arthritis, total hip replacement can restore the function of the hip joint.
References
[1] Srisaarn, T., Salang, K., Klawson, B., Vipulakorn, K., Chalayon, O., & Eamsobhana, P. (2018). Surgical correction of coxa vara: Evaluation of neck shaft angle, Hilgenreiner-epiphyseal angle for indication of recurrence. Journal of Clinical Orthopaedics and Trauma, 10(3), 593.
[2] Velavan MV, Harshavardhan JKG. Coxa Vara of Unknown Etiology: A Unique Case Report. Journal of Orthopaedic Case Reports 2025 August, 15(08): 201-206.
[3] Audisio, A., Cacciola, G., Braconi, L., Giudice, C., Massè, A., & Aprato, A. (2024). Proximal femoral valgus osteotomy for the treatment of developmental coxa vara: A systematic review of the literature. Journal of Orthopaedics, 53, 87-93.
[4] Carpintero, P., Leon, F., Zafra, M., Serrano-Trenas, J. A., & Román, M. (2003). Stress fractures of the femoral neck and coxa vara. Archives of orthopaedic and trauma surgery, 123(6), 273–277.
[5] Jones J, Walizai T, Murphy A, et al. Coxa valga. Reference article, Radiopaedia.org (Accessed on 28 Oct 2025).
[6] Gandbhir VN, Lam JC, Lui F, et al. Trendelenburg Gait. [Updated 2024 Feb 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541094/
[7] Srisaarn, T., Salang, K., Klawson, B., Vipulakorn, K., Chalayon, O., & Eamsobhana, P. (2019). Surgical correction of coxa vara: Evaluation of neck shaft angle, Hilgenreiner-epiphyseal angle for indication of recurrence. Journal of Clinical Orthopaedics and Trauma, 10(3), 593-598.
[8] Audisio, A., Cacciola, G., Braconi, L., Giudice, C., Massè, A., & Aprato, A. (2024). Proximal femoral valgus osteotomy for the treatment of developmental coxa vara: a systematic review of the literature. Journal of Orthopaedics, 53, 87–93.
[9] Herring, J. A. (2021).Tachdjian’s Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children(6th ed.). Philadelphia, PA: Elsevier.