
 is what we call effort thrombosis of the upper extremity. It’s a type of...){kind=link}

Paget Schroetter Syndrome Paget-Schroetter Syndrome (or PSS for short) is what we call effort thrombosis of the upper extremity. It’s a type of deep vein thrombosis, but instead of affecting the legs, it affects the subclavian vein: the main vein that drains the arm.
Unlike the usual deep vein thrombosis, though, this doesn’t usually happen to sedentary or sick patients. It happens to fit young, active people: athletes, swimmers, baseball pitchers, even manual workers, after repetitive overhead motion.
Even though it’s uncommon compared to lower extremity DVT, it’s actually the most important cause of upper limb venous thrombosis in healthy adults.
Global Trends: Paget Schroetter Syndrome
Upper-extremity DVTs make up about 1–4% of all DVTs; Paget–Schroetter syndrome is a leading cause of primary (effort-related) upper-extremity DVT. In young, active adults, and population incidence estimates are low (roughly 1–2 cases per 100,000 per year). In all of these people, the right side is slightly more commonly affected because a majority of people are right-hand dominant.
In general, the group most affected is young men between 20 to 40 years of age who participate in activities involving repetitive arm elevation or overhead movements. This doesn’t have to be an intense gym workout necessarily; it can be something as simple as baseball, swimming, or tennis.
Underlying Cause of Paget-Schroetter Syndrome
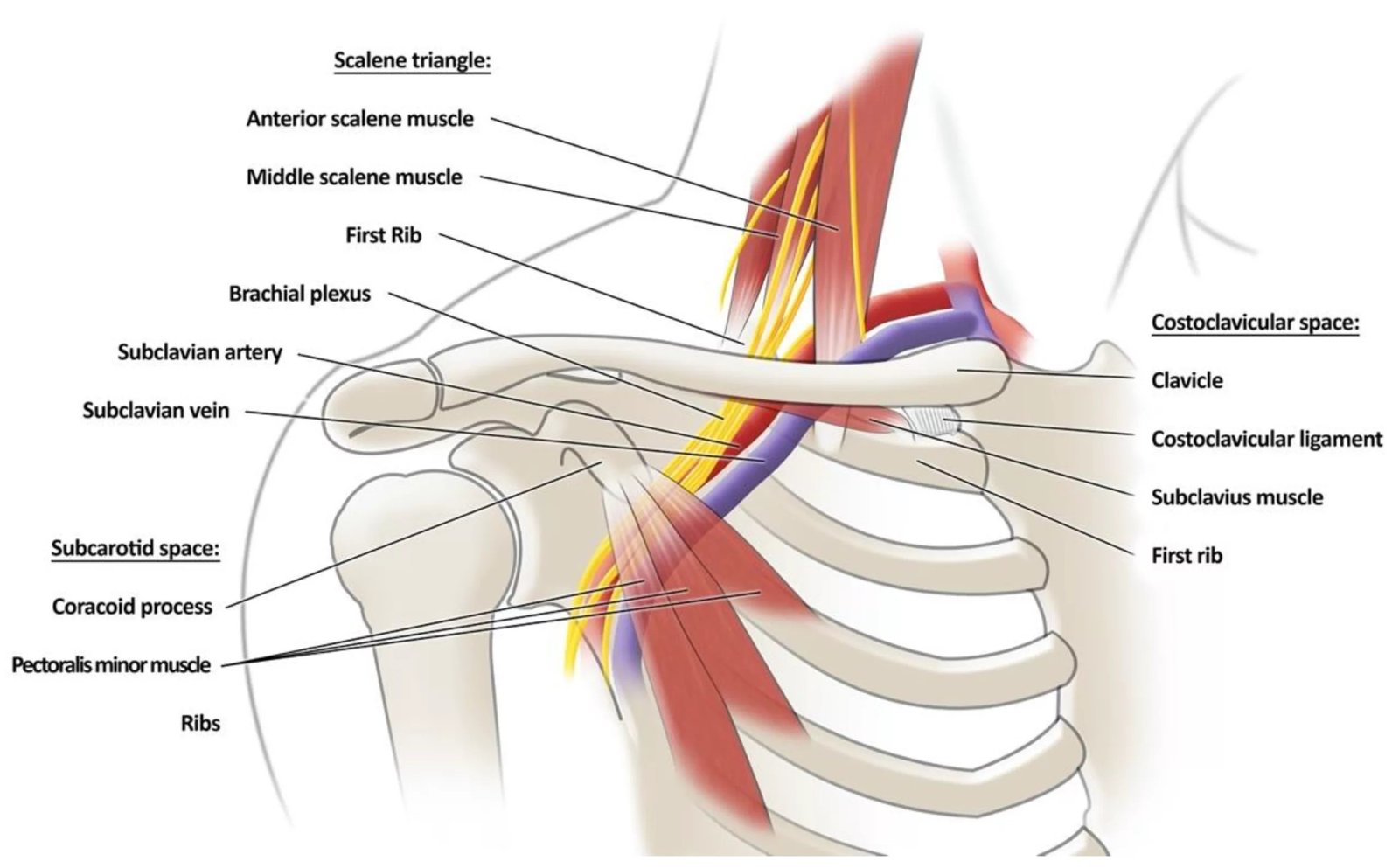
The subclavian vein runs under the clavicle through a tunnel-like anatomical space called the costoclavicular space, to meet the internal jugular vein and from there create the brachiocephalic vein before draining into the heart. This is essentially a very narrow anatomic space between the clavicle, the first rib, and some small muscles like the scalenes and subclavius.
The deep venous system of the upper extremity. The subclavian vein passes beneath the clavicle to join the internal jugular vein before entering the thorax. (Image Courtesy: Bosch, F. T., Nisio, M. D., Büller, H. R., & Van Es, N. (2020). Diagnostic and Therapeutic Management of Upper Extremity Deep Vein Thrombosis. Journal of Clinical Medicine, 9(7), 2069. Available fromMDPI. Licensed under CC by 4.0)
The vein gets compressed a little naturally, but in susceptible individuals, vigorous or repetitive arm movement causes mechanical compression of the vein against these structures, particularly between the first rib and clavicle.
That repeated compression:
1. Injures the inner wall (endothelium) of the vein
2. Slows down the blood flow
3. Triggers clot formation
Together, these form the classic Virchow’s triad: endothelial injury, stasis, and hypercoagulability.
Anatomical Predisposition
What makes some people more susceptible to Paget-Schroetter Syndrome are certain structural anomalies in the thoracic outlet:
- Narrow costoclavicular space
- Hypertrophied scalene or subclavius muscles
- Presence of a cervical rib or fibrous bands
- Posture-related compression from shoulder depression or forward rotation
Risk Factors for PSS
While repetitive arm movement is the overwhelmingly predominant trigger, some other predisposing factors exist. Identifying secondary factors is also important to prevent recurrence.
- Swimmers, baseball pitchers, rowers, weightlifters, and anyone who has to do repetitive lifting or carrying.
- Individuals with congenital anatomical anomalies, like a cervical rib, a narrow costoclavicular space, or tight fibrous bands that compress the vein even at rest.
- Drooping shoulders or forward head posture can also reduce the thoracic outlet space.
- External compression because of backpack straps or tight shoulder garments.
- Hypercoagulable state resulting from Factor V Leiden mutation, oral contraceptives, or malignancy.
- Prior shoulder trauma or central venous catheterization.

Anatomic variations, including fibrous bands and cervical ribs, serve as structural risk factors for thoracic outlet syndrome. (Image Courtesy: Maślanka, K., Zielinska, N., Karauda, P., Balcerzak, A., Georgiev, G., Borowski, A., Drobniewski, M., & Olewnik, Ł. (2022). Congenital, Acquired, and Trauma-Related Risk Factors for Thoracic Outlet Syndrome—Review of the Literature. Journal of Clinical Medicine, 12(21), 6811. Available fromMDPI. Licensed under CC by 4.0)
Symptoms of Paget-Schroetter Syndrome
Symptoms are usually acute in nature and have a sudden onset after some strenuous activity of the arm, e.g., gym workouts, weight training, rowing, or playing sports that require overhead throwing activities.
1. Pain and swelling in one arm
The patient almost always describes severe, acutely developing swelling with a dull ache and a sense of heaviness in an arm, typically following overhead work or exercise. The swelling is often described as warm.
In most cases, this swelling affects the whole arm, even including the shoulder and neck region. This is because the subclavian actually drains the entire limb.
However, a localized swelling should not automatically exclude this diagnosis. This is often the case in early or partial clots, and only later does it become more diffuse.

Right upper extremity edema and erythema indicate acute venous congestion from subclavian vein thrombosis. (Image Courtesy: Tan, G., Ng, M. Emergency department point-of-care ultrasound for upper extremity deep venous thrombosis ED POCUS for upper extremity DVT. Int J Emerg Med 14, 66 (2021). Available fromBMC. Licensed under CC by 4.0)
2. Bluish discoloration and visible veins
Due to venous congestion, the skin may appear bluish or purplish (cyanotic), and the superficial collateral veins over the shoulder and chest become visibly prominent. This appearance is known as Urschel’s sign, and is a giveaway sign.
3. Feeling of numbness or tightness
Some patients report experiencing sensory changes, for example, tingling or numbness, because of the engorged veins compressing their adjacent nerves, but major neurological deficits like true weakness or paralysis are rare.
4. Symptoms improve with rest
A notable differentiating feature from other similar causes of upper limb swelling is that raising the arm noticeably worsens these symptoms. On the other hand, there is a clear improvement in the symptoms with rest.

Physical examination showed left upper limb swelling and prominent superficial veins consistent with Paget–Schroetter Syndrome. (Image Courtesy: Fukushima, A., Kobayashi, T., Kuno, H., Hiroki, J., & Yoshida, A. (2023). Paget–Schroetter syndrome occurs in the nondominant hand. Clinical Case Reports, 11(12), e8308. Available fromWiley Online. Licensed under CC by 4.0)
Paget-Schroetter Syndrome vs. Thoracic Outlet Syndrome
Paget-Schroetter syndrome is often called the venous form of thoracic outlet syndrome. Thoracic Outlet Syndrome refers to a group of conditions that occur when the blood vessels or nerves passing through the thoracic outlet, the narrow space between the clavicle and first rib, become compressed. TOS can be neurogenic, arterial, or venous.
Neurogenic TOS results from brachial plexus compression, and arterial TOS from subclavian artery compression; venous TOS specifically affects the subclavian vein. Hence, PSS and TOS do indeed overlap.
While Paget-Schroetter Syndrome is classified as the venous subtype of Thoracic Outlet Syndrome, it differs in both its underlying mechanism and clinical presentation. This distinction is crucial to make because both conditions can present at the same time. Paget-Schroetter Syndrome is vascular and can cause thrombosis, requiring urgent anticoagulation and thrombolysis. The table below highlights key distinctions between Paget-Schroetter Syndrome and the more common neurogenic type of Thoracic Outlet Syndrome to help differentiate the two conditions.
| Feature | Paget-Schroetter Syndrome | Thoracic Outlet Syndrome (Neurogenic Type) |
|---|---|---|
| Primary structure involved | Subclavian vein | Brachial plexus |
| Main symptoms | Swelling, cyanosis, heaviness | Numbness, tingling, weakness |
| Onset | Acute or subacute after exertion | Chronic, progressive |
| Physical findings | Distended superficial veins, discoloration | Positive Adson’s or Roos test |
| Treatment | Thrombolysis + first-rib resection | Nerve decompression, posture therapy |
Differential Diagnosis of PSS
Other causes of unilateral arm swelling and pain to consider include upper extremity cellulitis, lymphatic obstruction, hematoma, central venous catheter thrombosis, and secondary DVT due to malignancy or thrombophilia.
Diagnosis of Paget-Schroetter Syndrome
1. Clinical Evaluation
A detailed history and physical examination are the first step of diagnosis.
The clinician inquires about recent physical exertion, heavy lifting, or sports involving arm elevation, history of CV catheter, or carcinoma.
Typical findings on immediate physical examination include:
- Unilateral arm swelling, pain, and discoloration
- Prominent collateral veins over the chest wall or the shoulder
- Tenderness along the axillary or subclavian vein
- Signs and symptoms worsening with arm abduction or elevation
If these findings are noted, imaging is immediately warranted.
2. Imaging Studies
Duplex Ultrasonography
This is the first-line investigation. It is fast, non-invasive, easily available, and can confirm the absence of blood flow or show a thrombus in the subclavian or axillary vein. But sometimes, the clavicle blocks proper visualization of the subclavian.
Here are the likely findings on a Doppler:
- First, the subclavian vein won’t compress the way it normally should when pressure is applied with the probe. That’s the first clue there’s a clot sitting inside.
- Second, the thrombus itself could be visible as an echogenic mass within the vein’s lumen.
- Third, on a color Doppler, there’s little to no venous flow in that area, or it’s sometimes very sluggish.
- Finally, in chronic cases, collateral veins can be seen forming around the blockage. This is the body’s backup drainage system, trying to keep blood moving despite the obstruction.

Ultrasound image showing a 5 mm echogenic thrombus within the lumen of the left axillary vein. (Image Courtesy: Fukushima, A., Kobayashi, T., Kuno, H., Hiroki, J., & Yoshida, A. (2023). Paget–Schroetter syndrome occurs in the nondominant hand. Clinical Case Reports, 11(12), e8308. Available fromWiley Online. Licensed under CC by 4.0)
Contrast Venography
Venography is still considered the gold standard, but is now mainly used for detailed anatomical assessment or when planning endovascular or surgical intervention. It can show:
- A visible clot in the lumen
- An abrupt cut-off of contrast in the subclavian or axillary vein
- Collateral flow pathways
Dynamic venography, with arm movement and periods of rest, can even show positional compression.
CT or MR Venography
Cross-sectional imaging helps identify anatomic compression points and assess the surrounding muscles, clavicle, and first rib all in one frame, and it’s great for pre-operative planning.

Computed tomography with contrast demonstrating reduced venous opacification in the superior thoracic aperture, indicative of subclavian vein thrombosis in Paget–Schroetter Syndrome. (Image Courtesy: Fukushima, A., Kobayashi, T., Kuno, H., Hiroki, J., & Yoshida, A. (2023). Paget–Schroetter syndrome occurring in the nondominant hand. Clinical Case Reports, 11(12), e8308. Available fromWiley Online. Licensed under CC by 4.0)
Other Tests
If we suspect a recurrent or spontaneous event, it’s advised to check for thrombophilia, inherited clotting tendencies like Factor V Leiden or prothrombin mutations.
Treatment of Paget-Schroetter Syndrome
The goal is simple: restore venous patency, prevent pulmonary embolism or another clot, and fix the underlying cause.
1. Immediate (Acute) Management
Anticoagulation
Initial treatment classically is with heparin of some form (LMWH or UFH), to prevent the clot from expanding. The treatment then switches to an oral anticoagulant (usually warfarin or DOACs). The duration varies and is related to the time for venous recovery, the relevant risk factors, and the time to surgery. Since Paget–Schroetter Syndrome is a provoked event, therapy is limited to about three months unless other thrombophilic conditions are present.
They don’t dissolve the clot directly; they just stop it from growing while the body’s natural fibrinolytic system clears it.
Thrombolysis
If the clot is fresh, less than two weeks old, catheter-directed thrombolysis is the gold standard. The catheter delivers a thrombolytic drug like alteplase (tPA) right into the thrombus to dissolve it.
This can open up the vein relatively quickly, restore flow, reduce symptoms and swelling, and also help preserve venous function. It is followed by imaging to confirm that the vein is once again patent and flowing.
It carries a small risk of bleeding, though, and is contraindicated in patients who have recently undergone surgery or stroke.
2. Definitive (Surgical) Management
Thrombolysis alone isn’t enough; the underlying anatomical cause remains, and the clot can recur. The definitive treatment is only surgical decompression, and is usually performed after successful thrombolysis, once the acute inflammation settles, which is often within a few weeks.
- First-rib resection is the classic procedure: the surgeon removes part or all of the first rib to open up that narrow space and relieve the costoclavicular compression.
- At the same time, the surgeon may also perform a scalenectomy (remove the scalene muscles) or subclavius tenotomy to release fibromuscular structures that further narrow the passage.
- If, after decompression, the vein wall is found to be thickened or stenosed, a patch angioplasty can repair it.
- In selective cases, balloon venoplasty is done to widen the vein. However, stenting is avoided in this area of the body because stents are prone to fracture with shoulder movement.
3. Supportive Care
- After surgery, patients are asked to continue anticoagulation for an individualized duration advised by the treating team, and do gentle range-of-motion exercises to prevent stiffness.
- They are also advised to avoid strenuous, overhead activities till full healing.
- Compression sleeves can be of help in reducing edema.
- Pain control is managed with simple NSAIDs.
- Close follow-up imaging ensures vein patency and early detection of re-thrombosis.
Post-Thrombotic Complications
If diagnosis is delayed or only anticoagulation is used, the clot may scar the vein. That leads to post-thrombotic syndrome: chronic arm swelling, pain, and heaviness due to venous valvular damage. Recurrence is also more likely if the anatomic compression isn’t surgically corrected.
Even if Paget-Schroetter Syndrome is treated once, damage to the veins can be more long-lasting, with areas of permanent scarring and a decreased overall endurance. The condition does not typically result in death, although it is possible for a pulmonary embolism to re-occur if a part of the clot is dislodged.
Prognosis
Paget-Schroetter Syndrome rarely affects life expectancy. With early diagnosis and combined therapy (thrombolysis plus decompression), >90% of patients regain full limb function. They can go back to their sports, their jobs, and their normal lives.
Prevention and Lifestyle Measures
Because it’s not possible to change or fix the genetics and anatomy, Paget-Schroetter Syndrome is not really preventable. Still, the risk can be lowered somewhat by avoiding repetitive overhead movements and ensuring ergonomic arm postures in sports and work.
Conclusion
Paget-Schroetter Syndrome is an unusual condition in that it’s a thrombosis in young healthy patients with an active lifestyle. It’s caused by repetitive compression of the vein between the clavicle and first rib. This pathology shows that a tiny bit of anatomic narrowing of the thoracic inlet can lead to a critical condition.
Patients who have arm swelling, pain, and discoloration after arm exertion should be sent for immediate vascular evaluation. When treated promptly, patients enjoy full recovery with minimal sequelae.
References
[1] Zell, L., Kindermann, W., Marschall, F., Scheffler, P., Gross, J., & Buchter, A. (2001). Paget-Schroetter syndrome in sports activities–case study and literature review. Angiology, 52(5), 337–342. https://doi.org/10.1177/000331970105200507
[2] Illig, K. A., & Doyle, A. J. (2010). A comprehensive review of Paget-Schroetter syndrome. Journal of Vascular Surgery, 51(6), 1538–1547. https://doi.org/10.1016/j.jvs.2009.12.022
[3] Alla, V. M., Natarajan, N., Kaushik, M., Warrier, R., & Nair, C. K. (2010). Paget-Schroetter Syndrome: Review of Pathogenesis and Treatment of Effort Thrombosis. Western Journal of Emergency Medicine, 11(4), 358. https://pmc.ncbi.nlm.nih.gov/articles/PMC2967689/
[4] Illig, K. A., & Doyle, A. J. (2010). A comprehensive review of Paget-Schroetter syndrome. Journal of Vascular Surgery, 51(6), 1538–1547. https://doi.org/10.1016/j.jvs.2009.12.022
[5] Bagot, C. N., & Arya, R. (2008). Virchow and his triad: a question of attribution.British journal of haematology,143(2), 180–190. https://doi.org/10.1111/j.1365-2141.2008.07323.x
[6] Alla, V. M., Natarajan, N., Kaushik, M., Warrier, R., & Nair, C. K. (2010). Paget-Schroetter Syndrome: Review of Pathogenesis and Treatment of Effort Thrombosis. Western Journal of Emergency Medicine, 11(4), 358. https://pmc.ncbi.nlm.nih.gov/articles/PMC2967689/
[7] Garg, V., Poon, G., Tan, A., & Poon, K. B. (2017). Paget-Schroetter syndrome as a result of 1st rib stress fracture due to gym activity, presenting with Urschel’s sign – A case report and review of literature. International Journal of Surgery Case Reports, 49, 81-86. https://doi.org/10.1016/j.ijscr.2018.05.029
[8] Sanders, R. J., Hammond, S. L., & Rao, N. M. (2007). Diagnosis of thoracic outlet syndrome. Journal of vascular surgery, 46(3), 601–604. https://doi.org/10.1016/j.jvs.2007.04.050
[9] Rogers, S., Pole, R., Picton, A., & McCollum, C. (2020). Imaging subclavian vein thrombosis by duplex ultrasound: Getting it right. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 8(4), 700–701. https://doi.org/10.1016/j.jvsv.2020.01.020
[10] Karande GY, Hedgire SS, Sanchez Y, Baliyan V, Mishra V, Ganguli S, Prabhakar AM. Advanced imaging in acute and chronic deep vein thrombosis. Cardiovasc Diagn Ther 2016;6(6):493-507. doi: 10.21037/cdt.2016.12.06
[11] Hoexum, F., Hoebink, M., Coveliers, H. M. E., Wisselink, W., Jongkind, V., & Yeung, K. K. (2023). Management of Paget-Schroetter Syndrome: A Systematic Review and Meta-Analysis. European Journal of Vascular and Endovascular Surgery, 66(6), 866–875. https://doi.org/10.1016/j.ejvs.2023.08.065
[12] Fleck, D., Albadawi, H., Shamoun, F., Knuttinen, G., Naidu, S., & Oklu, R. (2017). Catheter-directed thrombolysis of deep vein thrombosis: Literature review and practice considerations. Cardiovascular Diagnosis and Therapy, 7(Suppl 3), S228. https://doi.org/10.21037/cdt.2017.09.15
[13] Hwang, J., Min, J., Jo, M., & Shin, J. S. (2017). Video-assisted thoracoscopic surgery for intrathoracic first rib resection in thoracic outlet syndrome. Journal of Thoracic Disease, 9(7), 2022. https://doi.org/10.21037/jtd.2017.06.122
[14] Kahn S. R. (2016). The post-thrombotic syndrome. Hematology. American Society of Hematology. Education Program, 2016(1), 413–418. https://doi.org/10.1182/asheducation-2016.1.413