
{kind=link}

H3N2 influenza 2025 As we move into December 2025, healthcare systems across the UK, the United States, and large parts of Asia are reporting a sharp rise in influenza‑related hospital visits, in what is being called the “super flu”. The term is a media-driven label, not a scientific one, for the dominant influenza strain this season: Influenza A (H3N2), Subclade K. Influenza, commonly known as the flu, is a contagious respiratory illness caused by influenza viruses that primarily infect the nose, throat, and lungs.
What’s different this year from the normal seasonal influenza is that population immunity seems to have thinned out, and the virus is spreading faster. This is because H3N2 has not been a dominant strain for a few years now; the H1N1s and other respiratory viruses were. So over time, immunity waned, and when this variant re‑emerged with enough genetic mutations to bypass old antibodies, it was able to infect a vulnerable population.
The economic ripple has been impossible to ignore, not because people are dying, but because the recovery time is much longer, stretching well into two weeks, and also coming with a post-viral fatigue. Unlike a standard cold, this H3N2 variant is causing record-breaking levels of workplace absenteeism and school closures.
What is H3N2 Subclade K?: H3N2 influenza 2025
Subclade K is not a new virus, just a version of Influenza A (H3N2), which is scientifically labeled as J.2.4.1 based on mutations. Early surveillance data suggest that this clade shows substantial antigenic drift compared with previously circulating H3N2 strains.
Normally, the flu virus is known to constantly accumulate minor mutations, a process called antigenic drift. Usually, these changes are minor, and our immune systems can still recognize the virus. And the seasonal flu vaccines also target any major mutations.
But Subclade K is different. It has more extensive mutations than those seen in recent seasons, and people infected with older versions of H3N2, or who were vaccinated against them, may have reduced immune recognition rather than complete protection.
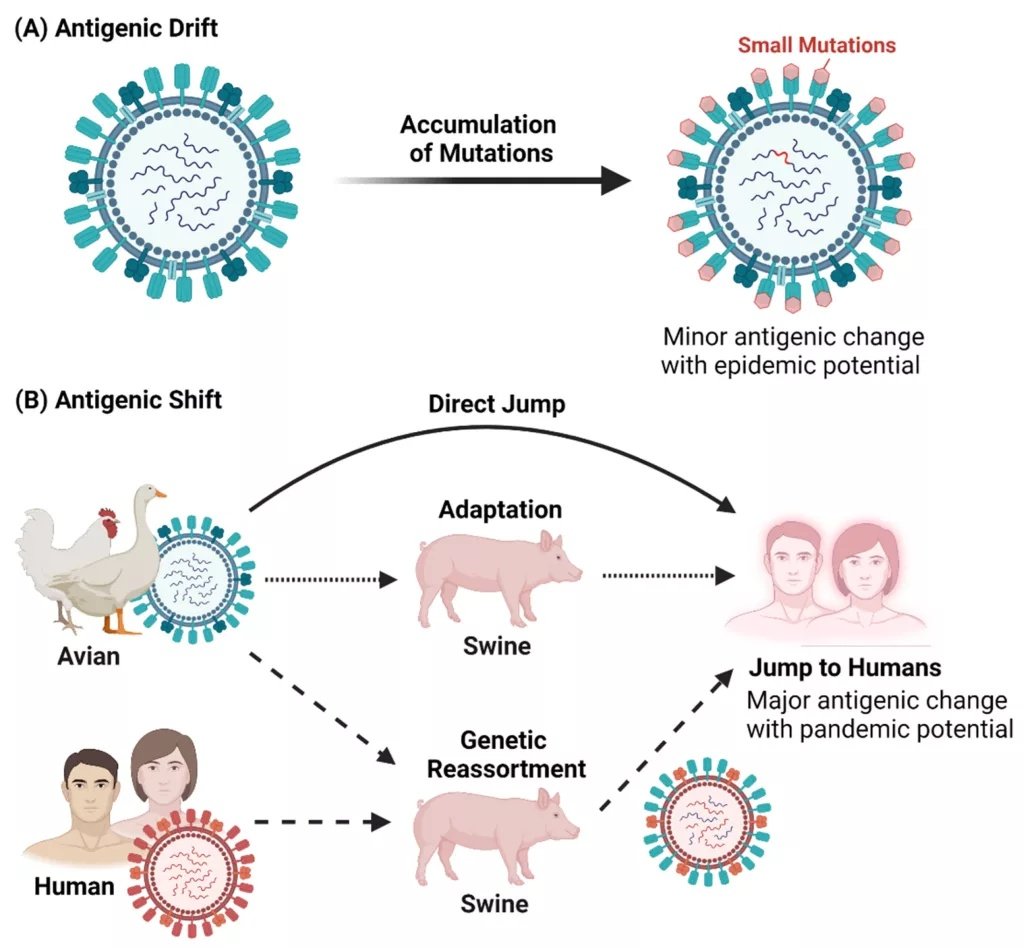
Antigenic drift and antigenic shift in Influenza A viruses: Antigenic drift refers to the gradual accumulation of small genetic mutations that lead to minor changes in viral surface proteins over time. Antigenic shift, in contrast, involves major genetic changes, often through reassortment or cross-species transmission, resulting in new influenza strains with pandemic potential (Image Courtesy: Yeo, J. Y., Ken-En Gan, S., Yeo, J. Y., & Ken-En Gan, S. (2021). Peering into Avian Influenza A(H5N8) for a Framework towards Pandemic Preparedness. Viruses, 13(11). Available fromMDPIand licensed under CC by 4.0)
Difference Between Influenza A and B
There are several types of influenza viruses, but Influenza A and Influenza B are responsible for nearly all seasonal flu infections in humans. These two types differ in how they evolve, whom they infect, and the kind of outbreaks they cause. Understanding these differences helps explain why some flu seasons are mild while others, like the current H3N2-dominated season, are more severe.
Influenza A
Type A is unique because it can infect both humans and animals (like birds and pigs). This is why type A is responsible for every major global pandemic in history. It mutates very quickly. This is why we need new vaccines every year and why strains like Subclade K can suddenly emerge and catch our immune systems off guard. Generally, Influenza A (especially H3N2) is associated with more severe symptoms in adults and the elderly.
Influenza B
As opposed to type A, type B almost exclusively infects humans. Because it doesn’t have an animal host to hide in and mutate, it evolves much more slowly than type A. It does not cause pandemics. While it can cause local outbreaks (like in a school), it doesn’t have the global explosive potential of type A. While Type A is often tougher on older adults, Influenza B is notorious for hitting children harder. In kids, type B is more likely to cause symptoms like vomiting and diarrhea.
The H3N2 Strain is Particularly Dangerous
Yes, seasons dominated by H3N2 tend to be worse than those dominated by H1N1 or Influenza B. There are a few reasons.
- First, H3N2 is good at replicating in the upper and lower respiratory tracts, so it produces a high viral load.
- Second, the Subclade K variant has an estimated R₀ (Basic Reproduction Number) of 1.4, more spreadable than the seasonal flu rate of 1.2. That means that this version of the flu moves through schools and office buildings much faster.
- Third, it’s incredibly good at evading the immune system in the very old and the very young, which means that more people start developing secondary infections, like pneumonia.
Symptoms of the 2025 Influenza Outbreak
While a common cold builds over days, H3N2 often strikes within hours. The symptoms are:
- Persistent cough
- Sneezing and a runny nose
- High-grade fever
- Fatigue and body aches
The signature symptom of this year’s flu strain is a dry, hacking, persistent cough that lasts 2 to 3 weeks. The virus causes significant inflammation in the lining of the respiratory tract. So even after the virus is gone, the irritated airway remains hypersensitive to cold air or talking, keeping the cough persistent.
H3N2 Influenza vs. COVID-19
In late 2025, COVID-19 and H3N2 are going around simultaneously. While they look similar, there are a few signs that can help you distinguish them (though a test is the only way to be 100% sure):
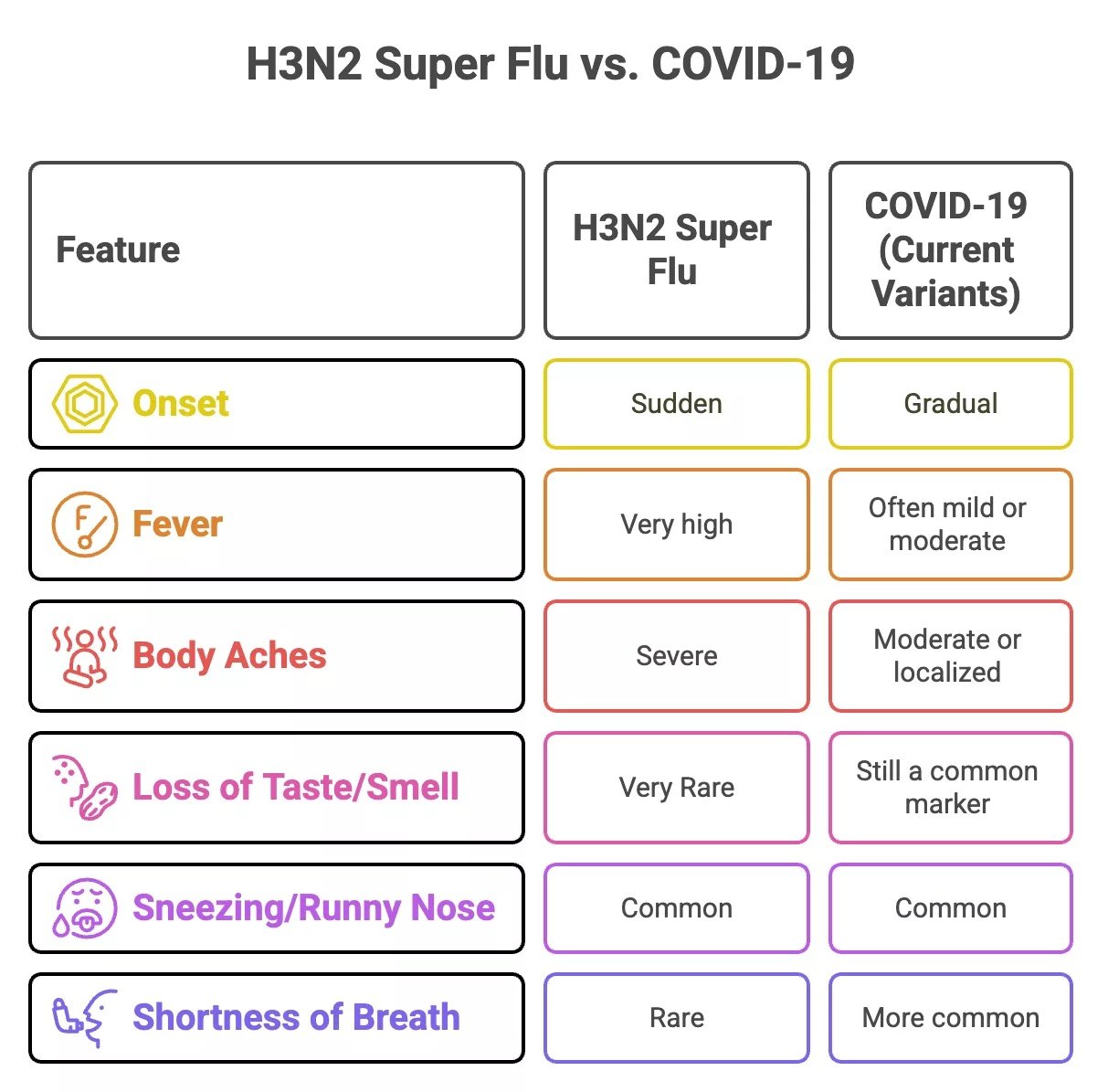
Comparison of H3N2 Influenza (“Super Flu”) and COVID-19. The table highlights key differences in symptom onset, fever intensity, respiratory features, etc., to help distinguish between the two illnesses during overlapping circulation periods.
The “Long Flu” Phenomenon
We’re all familiar with Long COVID, but 2025 has brought the “Long Flu.” The immune response provoked by H3N2 Subclade K is intense enough that it puts even more of a damper on recovery. This leads to post-viral fatigue lasting two weeks or more after the fever breaks. Patients also report tiredness, poor concentration, appetite loss, and “brain fog”.
Complications of H3N2 Influenza
According to early clinical observations, doctors are noting a higher rate of systemic complications with Subclade K. The most common complication of H3N2 isn’t the virus itself, but what follows it. The flu weakens your immune system and damages the lining of your lungs, making it easy for bacteria to move in.
- Bacterial Pneumonia: If you start feeling better for a day or two, but then your fever returns suddenly with a painful, productive (with phlegm) cough, you may have developed pneumonia. This is a leading cause of H3N2 hospitalizations in 2025.
- Cardiac Stress: The high, prolonged fever and inflammation put a massive strain on the heart.
- Dehydration and Renal Stress: Because H3N2 often causes a total loss of appetite and high sweat-inducing fevers, dehydration can set in quickly, leading to kidney stress, especially in old age.
When Does the Flu Season End?
With the unexpectedly early and severe arrival of the H3N2 Subclade K variant in 2025, you’d expect the wave to be over earlier as well. But both the history and the preliminary data suggest a very long season still lies ahead. In the Northern Hemisphere (which includes the US, UK, and Pakistan), peak flu season usually tends to occur over the last week of December till the first weeks of February.
And while the worst part of the flu often wanes by late March, there will still be plenty of virus circulating till May, and it’s not unusual to see a secondary bump in the curve in March or April, powered by Influenza B.
Is the 2025 Flu Vaccine Effective Against H3N2?
As the Subclade K variant mutated after the vaccine strains for the vaccine were selected, there is a technical mismatch. Ongoing surveillance and real-world effectiveness data are still being collected.
However, if you look at the preliminary data that is coming out from the UK Health Security Agency and the data from Europe, we’re still seeing people who have been vaccinated have 70-75% protection against hospitalization in children, and about 30-40% protection against hospitalization in adults.
Who Should Get the Flu Shot?
If you have not been vaccinated, it is not too late. Vaccines usually take 10 to 14 days for immunity to fully build. Those groups that are most at risk in the current outbreak are being encouraged by health officials to get the vaccine.
- School-going children
- Anyone over the age of 65
- Pregnant women
- Anyone with asthma or diabetes
Types of Influenza Vaccines Available
In late 2025, the global vaccine strategy has shifted. All vaccines are now Trivalent (targeting the three most active strains), instead of the previous quadrivalent ones, as the B/Yamagata virus has not been detected globally for several years. Depending on your age and health, you have four main options:
- Cell-Based & Recombinant (Flucelvax, Flublok)
- Nasal Spray (FluMist)
- High-Dose & Adjuvanted (Fluzone HD, Fluad)
- Standard Egg-Based (Vaxigrip, Influvac)
Global Influenza Vaccine Pricing
Many countries offer free flu shots to people who are at higher risk of contracting the virus. Other than that, flu shots are also available privately, ranging from $15 to $30 (PKR 4,200 to 8,400), and specialized high-dose or cell-based vaccines can cost up to $50 (PKR 14,000). In developing countries like Pakistan, the trivalent version is generally available for $9 to $11 (PKR 2,500 to 3,000). However, the final cost varies according to the brand, region, and facility.
Treatment for H3N2 Influenza
While a typical flu might resolve in 5 days, this year’s strain is leaving many patients sidelined for two weeks or more. It’s important to note here that antibiotics do not treat influenza itself and should only be used if a secondary bacterial infection, such as pneumonia or sinusitis, is strongly suspected. Using antibiotics for a viral illness is only going to add to antibiotic resistance.
Antiviral Therapy
The most potent weapon (medication) that we have against the Super Flu is antivirals. This class of drugs includes Oseltamivir (Tamiflu) and the newer Baloxavir (Xofluza). Oseltamivir works by inhibiting the viral neuraminidase enzyme, but Baloxavir has a different mechanism, inhibiting the cap-dependent endonuclease enzyme. This inhibition, in turn, diminishes the ability of the virus to replicate itself and thus leads to decreased viral distribution throughout the respiratory tree.

Influenza viral replication and antiviral targets: This schematic illustrates the influenza replication cycle and highlights the stages inhibited by approved antiviral medications, along with newer agents currently in clinical and preclinical development. (Image Courtesy: Caceres, C. J., Seibert, B., Faccin, F. C., Cardenas-Garcia, S., Rajao, D. S., & Perez, D. R. (2022). Influenza antivirals and animal models. FEBS Open Bio, 12(6), 1142-1165. Available fromFEBSand licensed under CC by 4.0)
Antiviral therapy provides the greatest treatment effect within 48 hours of symptom onset. Efficacy decreases with later treatment, though some high-risk patients appear to derive benefit with later therapy.
Importance of Home Care
- A humidifier will help reduce irritation from the persistent cough.
- Use oral rehydration salts (ORS) or electrolyte drinks to prevent dehydration.
- Gargle with warm salt water 3 to 4 times a day.
- Take adequate rest.
Recovery:
With this year’s virulent flu, recovery is going to be very slow. And that’s not a bad thing; trying to “power through” demanding schedules and responsibilities after an illness can provoke a setback if not a full-blown relapse. But you can use a simple benchmark as a reference, the 24-hour fever-free guideline: you’re safe to return to your usual routines if your fever hasn’t spiked in 24 hours and you didn’t use fever-reducing medicine.
When to Seek Emergency Medical Attention?
- Difficulty breathing while resting or having blue-tinted lips/fingernails.
- Persistent pressure or sharp pain in the chest when breathing.
- Sudden “brain fog”.
- Symptoms that improve at first but then return worse.
- Signs of dehydration: inability to pass urine, extreme dizziness, or a very dry mouth.
Can Influenza Be Prevented?
Like other common respiratory diseases, influenza is mostly transmitted via small respiratory droplets or contaminated surfaces. There are relatively simple measures we can all take consistently to help prevent infection.
- Wearing a well-fitted N95 or KN95 mask in crowded or under-ventilated areas like public transportation, waiting rooms, and indoor social gatherings
- If you reduce close contact, avoid social events, and just stay home in general early in the illness, you can protect the populations at risk.
- Frequent hand washing with soap, regular cleaning of high-contact surfaces (phone, door handles), and just good basic cleanliness in general can break the chain of infection.
Final Word
Calling it the “Super Flu” might be a bit sensationalist. The H3N2 Subclade K has had a worse impact and run than any flu strain of the modern era, but it’s still just a flu-like respiratory virus. If anything, the immunity gaps and antigenic drift simply aligned this year. But fortunately, it’s nowhere as deadly as the COVID-19 pandemic.
The best strategies for riding out the 2025 flu season are going to be vigilance and rest. As long as people remember how to use preventive measures, recognize its most severe symptoms, treat it early, get a head start on vaccination, and rest enough, we’ll be just fine.
References
[1] Kirsebom, F. C., Thompson, C., Talts, T., Kele, B., Whitaker, H. J., Andrews, N., Aziz, N. A., Rawlinson, C., Green, R. E., Quinot, C., Gardner, N., Waller, E., Allen, A., Watson, C. H., McDonald, S. L., Zambon, M., Pebody, R., Ramsay, M., Hoschler, K., . . . Bernal, J. L. (2025). Early influenza virus characterisation and vaccine effectiveness in England in autumn 2025, a period dominated by influenza A(H3N2) subclade K. Eurosurveillance, 30(46), 2500854.
[2] Pebody Richard, Warburton Fiona, Andrews Nick, Ellis Joanna, von Wissmann Beatrix, Robertson Chris, Yonova Ivelina, Cottrell Simon, Gallagher Naomh, Green Helen, Thompson Catherine, Galiano Monica, Marques Diogo, Gunson Rory, Reynolds Arlene, Moore Catherine, Mullett David, Pathirannehelage Sameera, Donati Matthew, Johnston Jillian, de Lusignan Simon, McMenamin Jim, Zambon Maria. Effectiveness of seasonal influenza vaccine in preventing laboratory-confirmed influenza in primary care in the United Kingdom: 2014/15 end of season results. Euro Surveill. 2015;20(36):pii=30013.
[3] Su, S., Chaves, S. S., Perez, A., D’Mello, T., Kirley, P. D., Yousey-Hindes, K., Farley, M. M., Harris, M., Sharangpani, R., Lynfield, R., Morin, C., Hancock, E. B., Zansky, S., Hollick, G. E., Fowler, B., McDonald-Hamm, C., Thomas, A., Horan, V., Lindegren, M. L., Schaffner, W., … Fry, A. M. (2014). Comparing clinical characteristics between hospitalized adults with laboratory-confirmed influenza A and B virus infection. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 59(2), 252–255.
[4] Vohra, M. , Amir, M. , Sharma, A. and Osoro, I. (2023). H3N2 Virus Outbreak: A latest global threat. Journal of Zoonotic Diseases, 7(2), 275-282.
[5] Sun R, Cheng Y, Hu H. Influenza A/H3N2 and Its Co-infection with Other Respiratory Pathogens: Higher Pneumonia Rates and Prolonged Hospital Stays in Pediatric Patients.Jundishapur J Microbiol.2024;17(7):e148636.
[6] Saha, S., Chadha, M., Shu, Y., Lijie, W., Chittaganpitch, M., Waicharoen, S., Lindblade, K. A., Phengta, V., Phonekeo, D., Corwin, A., Touch, S., Buchy, P., Lin, R., Low, C., Kheong, C. C., Amado Tandoc, I., Vito Roque, J., Arguelles, V., Dawood, F. S., . . . Lal, R. B. (2016). Divergent seasonal patterns of influenza types A and B across latitude gradient in Tropical Asia. Influenza and Other Respiratory Viruses, 10(3), 176.
[7] Kirsebom Freja CM, Thompson Catherine, Talts Tiina, Kele Beatrix, Whitaker Heather J, Andrews Nick, Abdul Aziz Nurin, Rawlinson Christopher, Green Rebecca E, Quinot Catherine, Gardner Nicholas, Waller Elizabeth, Allen Alex, Watson Conall H, McDonald Suzanna LR, Zambon Maria, Pebody Richard, Ramsay Mary, Hoschler Katja, Singanayagam Anika, Lopez Bernal Jamie. Early influenza virus characterisation and vaccine effectiveness in England in autumn 2025, a period dominated by influenza A(H3N2) subclade K. Euro Surveill. 2025;30(46):pii=2500854.
[8] Qaseem, A., Wilt, T. J., Harrod, C. S., Obley, A. J., Carroll, K., Humphrey, L. L., Population Health and Medical Science Committee of the American College of Physicians, Haeme, R., Jackson, C. D., Kansagara, D., Krain, A., Mackey, K., Poonacha, T., Saini, S. D., & Vigna, C. (2025). Influenza Vaccines for 2025-2026 in Adults Who Are Not Pregnant or Immunocompromised: Rapid Practice Points From the American College of Physicians. Annals of internal medicine, 10.7326/ANNALS-25-04056. Advance online publication.
[9] Ahmed, S. K., Hussein, S., Qurbani, K., Ibrahim, R. H., Fareeq, A., Mahmood, K. A., & Mohamed, M. G. (2024). Antimicrobial resistance: Impacts, challenges, and future prospects. Journal of Medicine, Surgery, and Public Health, 2, 100081.
[10] Świerczyńska, M., Mirowska-Guzel, D. M., & Pindelska, E. (2022). Antiviral Drugs in Influenza. International Journal of Environmental Research and Public Health, 19(5), 3018.