
{kind=link}

epiglottitis throat infection Epiglottitis is a serious medical emergency that involves acute inflammation and edema of the epiglottis, a small flap of cartilage located at the base of the tongue. It is most commonly caused by bacterial infections such as Haemophilus influenzae type b (Hib), though viruses, fungi, trauma, or thermal injury may also be responsible.
The epiglottis is a protective valve that covers the laryngeal inlet during swallowing to prevent food and liquids from entering the airway. When inflamed, the epiglottis can rapidly become swollen and obstruct the upper airway, and, therefore, breathing becomes very hard, and in extreme cases, it becomes impossible. Typical symptoms include a severe sore throat, fever, painful swallowing, muffled voice, drooling, and difficulty breathing, with symptoms often progressing rapidly.
In the past, Epiglottitis was a major threat to young children. Since the widespread introduction of the Haemophilus influenzae type b (Hib) vaccine in the late 1980s and early 1990s, its incidence in children has declined dramatically. Today, epiglottitis is more frequently diagnosed in adults, particularly middle-aged men with underlying medical conditions. It is a sharp lesson on how vaccination can radically change the face of the disease.
Why is Epiglottitis an Emergency?: epiglottitis throat infection
Epiglottitis is labeled as a life-threatening emergency because airway obstruction can develop rapidly, sometimes within hours. What begins as a sore throat may turn out to be a life-threatening airway obstruction quicker than most individuals can imagine. It is not one of the things you wait out. It is extremely dangerous and even lethal to deal with at home.
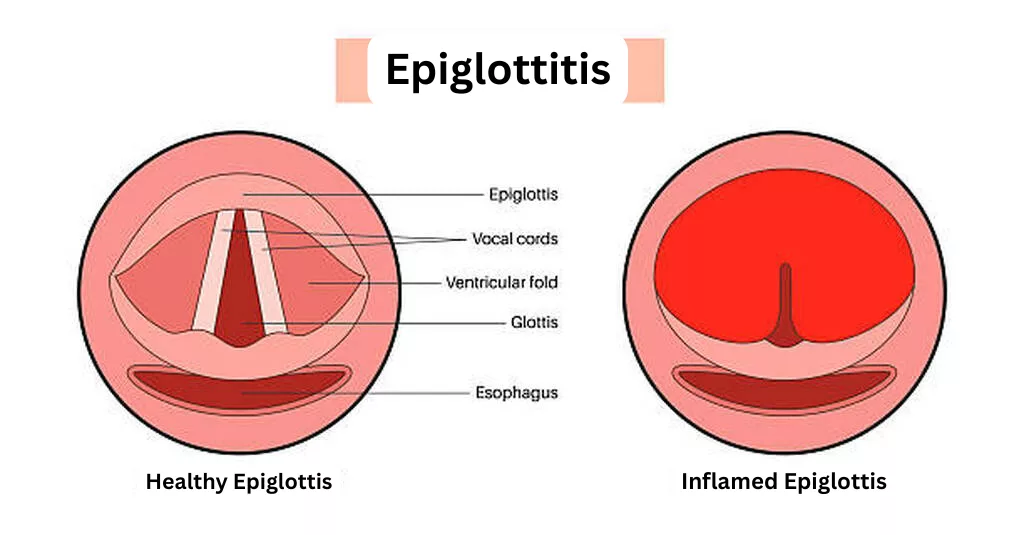
The difference between healthy epiglottis and inflamed epiglottis, which is seen in Epiglottitis
In the absence of immediate medical intervention to stabilize the airway, which should be in an emergency room, it can lead to respiratory arrest. Although mortality has decreased significantly with modern medical care, adult mortality rates are still reported at approximately 1–3%, particularly in high-risk individuals, underscoring the need for prompt action.
What Causes Epiglottitis?
Before the Hib vaccination era, most cases were caused by Haemophilus influenzae type b.Nowadays, this particular type is far rarer due to the highly efficient use of the Hib vaccine. Other bacteria are more frequently implicated, particularly among adults.
Common Bacterial Causes
The most common bacteria associated with the situation are:
- Streptococcus pneumoniae
- Staphylococcus aureus
- Group A Streptococcus
- Klebsiella pneumoniae
- Less commonly, Haemophilus influenzae (including non-typeable strains)
Other Causes Beyond Infection
The inflammation may also be triggered by:
- Viral infections, e.g, the cold sores (herpes simplex) or chicken pox (varicella-zoster).
- Infection by fungi, such as Candida (yeast), is especially those with impaired immune systems.
- Direct injury to the throat: This may occur due to physical trauma, by swallowing some sharp object, hot fluid incidentally, or by breathing in offensive chemicals or smoke.
Identifying the Signs: The Four D’s of Epiglottitis
The four Ds are a set of warning behaviors that medical professionals have to observe.
- Drooling: This is the inability to swallow their own saliva as the pain and swelling are too severe.
- Dysphagia: Severe pain and difficulty in swallowing.
- Dysphonia: A significantly soft, scratchy, or hot potato voice (it sounds like he is talking with a mouth full of hot food).
- Dyspnea (or Distress): An increasingly difficult breathing, which is the sign of the approaching airway blockage.
Epiglottitis Symptoms in Children
In children, the symptoms usually occur abruptly and develop quickly, in most cases within hours.
- Acute fever (usually going up to 104°F / 40°C)
- Bad, excruciating sore throat
- Excessive drooling
- Having trouble and pain when swallowing
- Noisy breathing with inspiratory stridor
- High level of irritability, disturbance, and anxiety- the child frequently appears incredibly sick.
- The Tripod Position: This is the most significant indication in which the child sits straight up, bends forward on the extended arms with the chin jutting forward and mouth wide open in an attempt to make breathing easier.
- Absence of cough, which helps distinguish epiglottitis from croup
What to Look For in Adults
In adults, symptom progression is often more gradual, developing over 24–48 hours, though airway risk remains significant.
- Extreme sore throat, which deteriorates quickly
- Pain during swallowing (odynophagia)
- A muffled or hoarse voice
- Breathing becomes difficult, and airways are perceived to be blocked
- Drooling
- Fever
- Neck tenderness
- Preference to sit upright and remain still to facilitate breathing
The fact that during a normal examination of the throat, the back may appear normal or slightly swollen is one of the most dangerous things about epiglottitis. The edema lies in the deeper part, at the windpipe opening.
Difference Between Epiglottitis and Croup
Epiglottitis and croup are both associated with breathing problems in children and have certain similar symptoms, such as stridor (noisy breathing), but they are fundamentally different disorders requiring very different management approaches.
Key Differences Between Croup and Epiglottitis
| Feature | Croup | Epiglottitis |
|---|---|---|
| Cause | Viral infection | Bacterial infection (usually, Hib, Streptococcus, Staphylococcus) |
| Location | Larynx, trachea, and bronchi | Upper airway and epiglottis |
| Onset | Gradual (over 2-3 days) | Sudden (hours) |
| Cough | Typical seal-like or barking cough | No cough or minimal cough |
| Drooling | Absent | Present (highly specific sign) |
| Fever | Low-grade (38-39°C) | High fever (often >40°C) |
| Age affected | 6 months to 3 years | Now more common in adults |
| Appearance | Mildly ill | Extremely ill, toxic appearance |
| Position | Any position comfortable | Tripod position preferred |
| Severity | Usually mild, self-limiting | Medical emergency requiring immediate intervention |
| Treatment | Steroids, nebulized epinephrine, supportive care | Airway protection, IV antibiotics, hospitalization |
The greatest distinction is that croup is usually a manageable disorder that can be cured through supportive care and medication, whereas epiglottitis will always be an emergency that must be taken to the hospital immediately, as it is life-threatening.
Who is at Risk?
These risk factors may be known to aid in prevention and early identification.
Non-Modifiable Risk Factors
- Sex and Age: It has an evident demographic pattern. The most prevalent group during the post-vaccine period is adult men between the ages of 40-60.
- Preexisting Health Conditions: There are some chronic diseases that form a background of susceptibility. Diabetes mellitus exhibits a very high association, presumably because it affects the risk of infection and recovery.
Modifiable Risk Factors
- Vaccination Status: In children, the status of not being vaccinated against Hib (Haemophilus influenzae type B) has been the largest domestic risk factor that can be avoided. Vaccination history may be a contributing factor even in adults.
- Lifestyle Factors: Smoking causes damage to the lining of the respiratory system, and it becomes easy to become infected. Excessive alcohol drinking may disrupt the immune system and defensive mechanisms.
- Obesity: Excess weight is linked to more severe cases as well, and it may be difficult to manage the airways when treating them.
Medical Conditions
In addition to the major risk factors, it is observed that the occurrence is more common among individuals with certain chronic problems, which include:
- Chronic obstructive pulmonary disease (COPD)
- Gastroesophageal reflux disease
- Tumors of the upper digestive/ respiratory tract
- Autoimmune diseases
Diagnosis of Epiglottitis
Diagnosis requires high clinical suspicion and prioritization of airway safety. The diagnostic method places airway safety first and above all, and the clinician should be ready to gain control of the airway at any time during the assessment process.
Clinical Presentation
The first evaluation starts with identifying the typical clinical presentation. The symptoms are usually an acute onset of severe sore throat, difficulty in swallowing, drooling, and a muffled or hoarse voice in patients.
The tripod sitting position, i.e., sitting upright and bending forward with the neck stretched out, is a worrisome symptom in children that is a sign of respiratory distress. The presence of fever is typical, and the patients can be highly anxious because of the difficulty in breathing.
Physical Examination
The inspection of the throat should be done very carefully. Direct inspection of the pharynx by use of a tongue depressor is usually not advised, especially in children, because the manipulation may cause laryngospasm and total airway blockage. In case the visualization is needed, it must be done in a controlled environment, like in an operating room.
Imaging Studies
Radiography of the lateral neck may be of supporting value in case of doubt in diagnosis and where the patient is stable. The radiographic findings are as follows:
- Thumb sign: The epiglottis is swollen in the shape of a thick and rounded shadow that looks like a thumb
- Obliterated vallecula
- Hypopharyngeal distension
Nevertheless, the imaging must not postpone the final airway care in the unstable patient. Referral to radiology should be thoughtfully weighed against the possibility of getting worse outside of emergency facilities. CT imaging may be considered in stable adults only.

The radiograph of the lateral soft-tissue neck shows the typical thumb sign of acute epiglottitis and an inflamed and swollen epiglottis.Image credit: Med Chaos, CC0, viaWikimedia Commons.
Direct Visualization
The gold standard of diagnosis is direct visualization by either fiberoptic laryngoscopy or nasopharyngoscopy. Findings include a markedly swollen, erythematous epiglottis, though the classic “cherry-red” appearance is not universal. This must be done by trained individuals in a well-controlled setting that is thoroughly prepared, with full preparation for emergency intubation or surgery to gain entry to the airway.

An image of laryngoscopy that shows significant swelling of the epiglottis, typical of epiglottitis, which may block the airway and require urgent medical care.Image credit: 藤澤孝志, CC BY-SA 3.0, viaWikimedia Commons.
Laboratory Testing
Laboratory investigations, such as complete blood count and blood cultures, are useful, but don’t postpone the treatment for them. High levels of white blood cells are usual, and blood cultures can determine the causative agent, although it takes some time. Throat cultures are not taken because there is a possibility of causing airway blockage.
Treatment of Epiglottitis
The management of epiglottitis revolves around two important priorities, i.e, ensuring the airway and giving proper antimicrobial therapy. It should be organized, with the participation of a multidisciplinary team including emergency medicine doctors, anesthesiologists, otolaryngologists, and intensivists.
Airway Management
The most important part of treatment is airway management. Any suspected epiglottitis must be observed in an environment that can offer airway interventions instantly. Supplemental oxygen therapy must be administered, and patients should not be forced to lie on their backs or be agitated, which may trigger acute obstruction. Patients must be left to keep in the position that gives them the most comfort in breathing.
Guidelines for Immediate Intubation
Immediately, intubation is needed in patients with the symptoms of impending respiratory failure:
- Severe stridor
- Cyanosis
- Altered mental status
- Lack of the ability to manage secretions
Intubation Procedure
Intubation is preferably done in the operating room by the most experienced available personnel, usually an anesthesiologist with an otolaryngologist standing by to do emergency tracheostomy as necessary. Key considerations include:
- Awake fiberoptic intubation: It is usually desirable in adults.
- Controlled inhalational induction: This is usually used in children
- Smaller endotracheal tube: This may be required because of airway edema
- Emergency backup: Cricothyrotomy or tracheostomy equipment ready
Antibiotic Therapy
Antibiotic treatment is to be provided as soon as the airway is controlled or airway management is underway. The most probable pathogens should be empirically treated, and these include Haemophilus influenzae type b, but Streptococcus pneumoniae, Staphylococcus aureus, and beta-hemolytic streptococci are also possible causes.
First-Line Antibiotics
- The best results in epiglotitis are of Third-generation cephalosporins like ceftriaxone or cefotaxime, which offer excellent coverage over H. influenzae that also includes beta-lactamase-producing strains.
- If the first one is not effective, then the substitute regimen is Ampicillin-sulbactam.
- In severe beta-lactam allergy: Fluoroquinolone with clindamycin.
Adjunctive Therapy
Inflammation and edema of the airway are commonly treated with corticosteroids, but there is limited evidence regarding their usefulness. However, most clinicians are incorporating them as supplement therapy since they have a potential positive effect and a low risk profile.
Supportive Care
There should be comprehensive supportive management that involves:
- Hydrating Intravenous fluids
- Antipyretics to treat fever
- ICU monitoring
- Intubation Period: 24 to 48 hours, usually
- Extubation criteria: improvement in the clinical condition, a drop in fever, and less swelling of the epiglottis on direct observation.
Prevention of Epiglottitis
Vaccination remains the most effective preventive strategy. This was a former childhood crisis, but now developed into a comparatively unusual case in immunized groups.
Hib Vaccination
The prevention strategy is based on the vaccination against Haemophilus influenzae type b (Hib), which is the primary cause of epiglottitis. The Hib vaccine that was introduced in the late 1980s and early 1990s has caused the incidence of epiglottitis in children to drastically reduce.
Vaccination Schedule
- First dose: 2 months of age
- Second dose: 4 months of age
- Third dose: 6 months of age
- Booster: 12 to 15 months of age
Impact
The effect of this immunization schedule has led to over 95 percent decrease in invasive Hib disease, including epiglottitis, in those countries that have a large number of people vaccinated.

HIB vaccine vial with a healthcare professional on the verge of making an injection to demonstrate that vaccination is one of the most significant preventative measures against Haemophilus influenzae type b infections, including epiglottitis.
Public Health Measures
High vaccination coverage by the public health programs is crucial in preventing further occurrences of the disease. Here, the role of healthcare providers is:
- Creating awareness of the importance of vaccines among parents.
- Discussing vaccine issues.
- Making sure children get full vaccination.
- To ensure the safety of vulnerable people, community immunity should be encouraged.
Chemoprophylaxis for Contacts
In close contacts of patients with Hib epiglottitis, chemoprophylaxis is suggested to avoid the development of second cases.
- Any household contact with unvaccinated or partially vaccinated children below the age of 4 years.
- Household contacts who are immunocompromised
Other Safety Measures
Pneumococcal Vaccination
Some protection is available against Streptococcus pneumoniae, which is an alternative causative organism, and this is achieved through pneumococcal vaccination. It has led to the general prevention of invasive bacterial infections such as epiglottitis by the routine vaccination of children and some adults at high risk, with the pneumococcal conjugate vaccine (PCV13 or PCV15/PCV20).
General Infection Prevention
Measures to avert the spread of the pathogen:
- Hand hygiene practices
- Respiratory etiquette
- Not going into contact with respiratory infection patients.
- Further safety measures against immunocompromised persons.
Wrapping Up
Epiglottitis is a severe emergency in medicine and is associated with the rapid blockage of the airways, which requires urgent hospitalization. Though the case in children has significantly reduced thanks to the Hib vaccine, adults, especially middle-aged men with comorbidities, are now most vulnerable.
The identification of the four Ds: drooling, dysphagia, dysphonia, and dyspnea is essential in the early diagnosis. The therapy depends on emergency airway precautions and intravenous antibiotics. Finally, the state of things supports the life-saving role of vaccination and the long-term need to have a rapid medical response in case of severe throat symptoms and difficulty with breathing.
References
[1] Guardiani, E., Bliss, M., & Harley, E. (2010). Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management.The Laryngoscope, 120(11), 2183-2188.
[2] Shah, R. K., Stocks, C. (2010). Epiglottitis in the United States: National trends, variances, prognosis, and management.The Laryngoscope, 120(6), 1256-1262.
[3] Sobol, S. E., & Zapata, S. (2008). Epiglottitis and croup.Otolaryngologic Clinics of North America, 41(3), 551–566.
[4] Berger, G., Landau, T., Berger, S., Finkelstein, Y., Bernheim, J., & Ophir, D. (2003). The rising incidence of adult acute epiglottitis and epiglottic abscess.American Journal of Otolaryngology, 24(6), 374–383.
[5] MayoSmith, M. F., Hirsch, P. J., Wodzinski, S. F., & Schiffman, F. J. (1986). Acute epiglottitis in adults. An eight-year experience in the state of Rhode Island.The New England Journal of Medicine, 314(18), 1133–1139.
[6] Katori, H., & Tsukuda, M. (2005). Acute epiglottitis: Analysis of factors associated with airway intervention.The Journal of Laryngology & Otology, 119(12), 967–972.
[7] Stroud, R. H., & Friedman, N. R. (2001). An update on inflammatory disorders of the pediatric airway: Epiglottitis, croup, and tracheitis.American Journal of Otolaryngology, 22(4), 268–275.
[8] Chang, Y. L., Lo, S. H., Wang, P. C., & Shu, Y. H. (2005). Adult acute epiglottitis: experiences in a Taiwanese setting.Otolaryngology–Head and Neck Surgery, 132(5), 689–693.
[9] Baird, S. M., Marsh, P. A., Padiglione, A., & Wills, T. E. (2010). Review of epiglottitis in the post Haemophilus influenzae type-b vaccine era.ANZ Journal of Surgery, 80(11), 800-801.
[10] Ismail, N. A., & Olveny, E. O. (2020). The role of imaging in acute epiglottitis: A systematic review.The Journal of Emergency Medicine, 58(4), 595-601.
[11] Wong, E. Y., & Berkowitz, R. G. (2001). Acute epiglottitis in children: The diagnostic role of lateral neck radiography.International Journal of Pediatric Otorhinolaryngology, 60(1), 23–28.
[12] Guldfred, L. A., Lyhne, D., & Becker, B. C. (2008). Acute epiglottitis: epidemiology, clinical presentation, management and outcome.The Journal of Laryngology & Otology, 122(8), 818–823.
[13] Ng, H. L., Sin, L. M., Li, M. F., Que, T. L., & Anandaciva, S. (2001). Acute epiglottitis in adults: a retrospective review of 106 patients in Hong Kong.Emergency Medicine Journal, 18(4), 271–275.
[14] Briere, E. C., Rubin, L., Moro, P. L., Cohn, A., Clark, T., & Messonnier, N. (2014). Prevention and control of Haemophilus influenzae type b disease: recommendations of the advisory committee on immunization practices (ACIP).Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports, 63(RR-01), 1–14