
 is a medical device that automatically detects abnormalities in a patient’s...){kind=link}

AED Automated External An automated external defibrillator (AED) is a medical device that automatically detects abnormalities in a patient’s heart rhythm and accordingly delivers an electric shock to resume normal heart activity. It is primarily designed for the treatment of sudden cardiac arrest (SCA), a condition where the heart abruptly stops beating effectively. The compact and user-friendly design of AEDs allows members of the general public to use them with minimal training. The efficiency and ease-of-use of these devices validate their presence in public places like schools, airports, etc. Early defibrillation is one of the strongest predictors of survival in out-of-hospital cardiac arrest, emphasizing the importance of public access defibrillation programs.
Types Of External Defibrillators: AED Automated External
Based on the user interface, external defibrillators are divided into:
Semi-Automatic External Defibrillators (SAEDs): These defibrillators detect heart rhythm and decide the dosage of electric shock, but need you to press the shock button for delivery. SAEDs are more commonly available.
Fully Automatic External Defibrillators (FAEDs): A fully automatic device itself delivers the shock without the need to press a button. Studies show that fully automated AEDs reduce hesitation among non-medical people and can potentially improve AED effectiveness. [1]
Defibrillation For Sudden Cardiac Arrest
To understand the use of an AED, you must first learn about the different components that make up an automated defibrillator.
Components of an AED:
An AED looks like a typical first aid box. Some find it similar to a small toolbox. You will find two cables attached to the box with electrodes (which look like postcard-sized stickers). The detailed breakdown of AED’s components is given below:

An AED is installed in a park.
Electrode Pads:
Every defibrillator has electrode pads that attach to the patient’s skin. These self-adhesive pads are placed on the patient’s bare chest and help deliver an electric shock directly to the patient’s heart. Conventionally, sticking/adhesive pads have been used in defibrillators. However, developers now aim to utilize different treatment strategies in electrode pad development to increase the efficacy of the defibrillator. For example, a design of microneedle pads for an automated external defibrillator is being implemented.[2] Microneedling is a technique in which small, fine needles are inserted into the skin to trigger natural healing responses of the body.
Battery & Capacitor:
The power source of an AED is a battery that charges a capacitor, which releases high-energy voltage (shock). AED batteries are typically lithium-based and can last several years depending on use and storage conditions.
Processor:
Just like a computer’s CPU, the processing/control unit of an AED does the major job. It automatically analyzes the patient’s heartbeat and rhythm and decides whether the patient needs an electric shock or not. If needed, it also determines what intensity will be suitable in a particular case. It also calculates the required shock energy and provides instructions for safe use.
Control Panel:
The control panel is a very important part of an AED because, without it, the use of an AED without proper professional training is not possible. The panel consists of a display screen, a shock button, and an on/off power button. Audio and visual prompts, i.e., clear-cut guidance instructions, appear on the screen, which help the general public apply the electrode pads to the patient correctly. These prompts are designed to be intuitive and language-independent so that even untrained bystanders can use the AED effectively
Who can use an AED?
An automated defibrillator is easy to use. These advanced devices provide simple prompts to guide even a layman to attach the electrodes and help save a life. An AED can be used by anyone, not just medical professionals, thanks to the voice-guided instructions. In many countries, public training initiatives and Good Samaritan laws encourage bystanders to use AEDs without fear of legal repercussions, as early defibrillation significantly improves survival chances. However, you can expect the doctors, nurses, and paramedics to use it with greater command and ease.
AED Vs Conventional Manual Defibrillators: Benefits Of Automated Devices
User-Friendly:
A conventional defibrillator requires extensive medical training and proper certification to operate. On the other hand, an AED can be used by a layperson with minimal or no training.
Simple Interface:
As AEDs are designed for use by laypersons, the user interface is kept simple. The voice instructions and screen/button layout make it easy to use. Contrary to this, a manual defibrillator has complex buttons and control designs that can only be operated by a trained person. Proper audio-visual instructions play a significant role in guiding non-medical people and can save crucial time.[3]
Easier Operation:
With manual defibrillation devices, trained professionals have to analyze the patient’s ECG and decide what energy level (of shock) will work for the patient. However, advanced automated devices automatically analyze the patient’s heartbeat and rhythm. It also adjusts the shock intensity without human guidance.
Quick Delivery of Care:
In the management of sudden cardiac arrest, time is crucial. A minute’s delay in defibrillation reduces survival chances by about 10%. Therefore, quicker delivery of defibrillation always favors the patient. On-the-spot defibrillation by a layman is possible with an AED, which can save a life, contrary to a conventional device, which is carried and operated by emergency medical responders. For manual defibrillation, you have to wait for professionals to arrive, which wastes time.
Safe:
A major concern in AED usage is the safety of the device. Studies show that errors associated with AEDs are very rare, i.e., 4%. This makes it a safe device for the patients.[4] Their internal algorithms prevent accidental shocks by delivering energy only when shockable rhythms, such as ventricular fibrillation or pulseless ventricular tachycardia, are detected.
How Does An AED Work?
Once the electrodes are properly placed on the patient’s chest, an automated external defibrillator identifies either of the two heart conditions:
Ventricular Tachycardia:
Pulseless ventricular tachycardia (pVT) is a condition in which the heart beats so fast that there isn’t sufficient time for the heart muscle to fill up with blood. This overactivity of the ventricles leads to an insufficient supply of blood to the organs. Thus, within a few seconds of onset, the person becomes unresponsive and collapses. Defibrillation interrupts this abnormal rhythm and allows the heart’s natural pacemaker to restore normal contractions.
Ventricular Fibrillation (V-fib):
It is a heart condition in which the heart muscle contracts in a chaotic way. The contractions are way faster than normal. The heart has four chambers, i.e., the atria and the ventricles. When ventricles follow this abrupt, chaotic rhythm of contraction, it is called ventricular fibrillation. When under fibrillation, the heart begins to twitch rather than pump blood to the body. This renders the heart inefficient to pump blood, which has negative consequences. It is the most common cause of sudden cardiac arrest.
An automated defibrillator identifies the erratic rhythm and gives an electric shock to restore a normal heartbeat. Defibrillation strategies help save the lives of ventricular fibrillation patients.[5]
Studies show that automated external defibrillators with a larger electrode size show better success rates in managing ventricular fibrillation.[6]
Asystole:
There is no need for an electric shock in asystole, and an AED accurately identifies the situation! As mentioned, automated defibrillators have smart algorithms that allow them to identify situations that require shocks. However, in conditions such as asystole, where there is a complete lack of heart activity, an electric shock won’t help. Thus, the AED guides you to give cardiac compressions to the patient.
Research shows that with accurate automated detection of the circulation, AEDs can detect the presence or absence of a pulsatile rhythm within the first 3 seconds (and respond accordingly).[7]
How to use an AED?
In almost all cases, the revival of an unconscious person requires defibrillation and resuscitation. If you have help, you can divide tasks. One of you should start doing chest compressions while the other person arranges the defibrillator and calls for ambulance/paramedic help!
Note: If managing alone, call an ambulance first and then immediately start chest compressions.
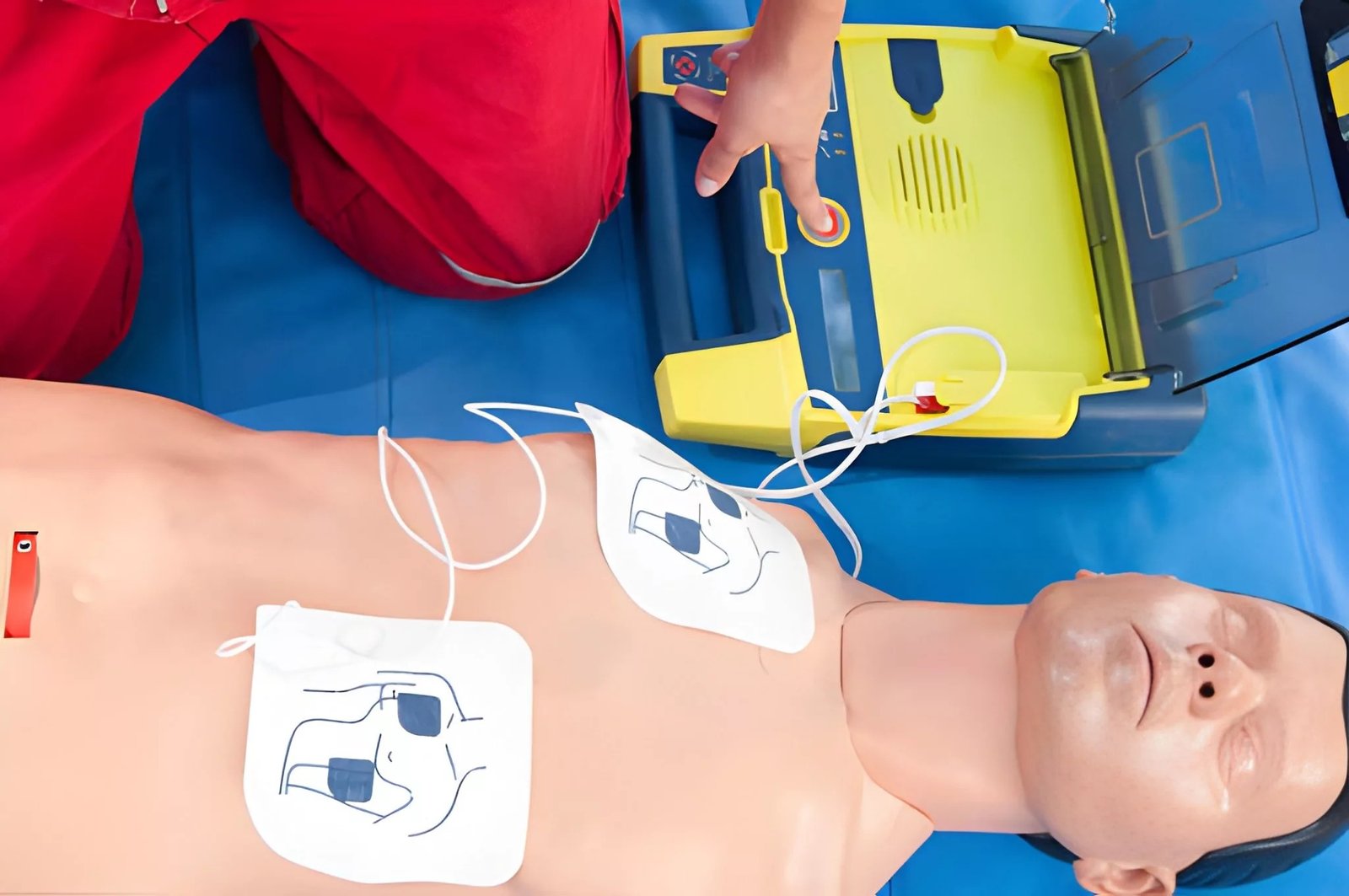
The picture shows the exact position of the electrode pads of an AED
Steps to use an AED:
- Turn on the automated external defibrillator and connect it.
- Expose the chest/abdomen region of the unconscious person.
- One person should continue with the chest compressions while you connect the electrodes to the chest of the unconscious person.
- Place one electrode under the right collarbone.
- Place the other electrode under the armpit on the left side of the chest.
- Ensure good skin contact and avoid placing pads over pacemakers, metal jewelry, or wet skin.[8]
- Follow the audio-visual instructions given by the AED.
- After connecting the electrodes, the AED will guide you if the person needs a shock or chest compressions.
- If the unconscious person’s heart is fibrillating, a semi-automatic external defibrillator machine will ask you to press the shock button (that usually has a “lightning” symbol).
- Fully automatic external defibrillators automatically deliver a shock if no rhythm is detected.
- Carefully follow further instructions from the AED.
Note: No one should be in contact (touching) with the unconscious person when the shock button is pressed (or the shock is being delivered)!
After fibrillation, continue the AED’s instructions regarding repeated chest compressions, etc.
Unconscious Person Management:
Automated defibrillators are smart machines that properly guide even a layman. Situations that require shock delivery can be managed well with a defibrillator, but the general public must be aware of how to do cardiopulmonary resuscitation. Proper training of adults on CPR and defibrillation can make a significant difference in society.[9]
AED Vs CPR:
Both defibrillation (from an AED) and cardiopulmonary resuscitation (CPR) are different yet crucial life-saving interventions for a person suffering from sudden cardiac arrest.
An automated defibrillator analyzes the fibrillations in a heart and delivers an electric shock to restore its normal beating rhythm. On the other hand, a CPR involves giving chest compressions and a breathing aid (rescue breaths) to circulate blood in the heart that triggers heart contraction.
While both techniques are used in unconscious persons, CPR is given to a patient whose heart has stopped beating completely. A defibrillation is needed when the heart goes into fibrillation (twitching), so it can not pump blood to the body.
Most of the time, both AED and CPR are needed to revive an unconscious person.
Instructions Regarding AED
Minimum Age for AED use:
There is no age restriction for AED usage. However, health experts advise using pediatric AED pads for children that can adjust the shock energy dosage according to the smaller body size. These pads are used for children aged below 8 years or weighing less than 25 kg.
You will need to modify the electrode placement if pediatric pads are not available. The larger-sized adult electrode pads can touch each other on a small (child’s) body. Thus, you should place one electrode pad on the front, i.e., the chest, while the other electrode should be placed on the back between the shoulder blades. This ensures the safety of the patient by preventing the touching of the pads.
Most advanced AEDs come with a dose attenuator for use on infants. However, health professionals prefer manual defibrillators for infants.
AED use on Pregnant Women:
Defibrillation with an AED is safe for pregnant women. It doesn’t pose any harm to the mother or the fetus as long as the electrode pads are placed properly. All you need to do is place one pad on the upper right chest and the other on the lower left side (below the breast). Shocks are delivered across the chest, not the abdomen, and therefore do not harm the fetus. Early intervention can save both maternal and fetal lives.
Risks & Complications
AEDs are very safe and accurate in identifying situations that require an electric shock. A defibrillator works only for heart conditions like ventricular fibrillation and ventricular tachycardia. If mistakenly given for any other kind of arrhythmia, a defibrillator can induce defibrillation and cardiac arrest. Minor skin irritation or burns at the electrode site are the most common complications, though rare.[10]
Advancements In AEDs
Different nations are adopting measures to improve emergency management services. As per studies, around 20% of all deaths in industrialized countries are attributed to sudden cardiac arrest.[11]It is estimated that the survival rate of a person decreases by approximately 10% for every 1-minute delay in treatment.
Therefore, different governments are trying methods of quick delivery of AEDs. In a simulation study done in the UK, delivery of an AED via a drone was found to be feasible.[12] This AED drone delivery method improves healthcare in rural and remote settings.[13]
Conclusion
Automated external defibrillators, i.e., AEDs, are smart medical devices that deliver a shock to restore a normal heart beating rhythm in unconscious individuals having pulseless ventricular tachycardia or ventricular fibrillation. These devices come with smart algorithms that allow them to detect the pulse, identify the cardiac problem, and adjust the shock dosage after electrodes are placed.
Even non-medical bystanders can very easily use AEDs to resuscitate an individual. All you need to do is just place the electrodes (one under the right collarbone and the second under the armpit on the left chest) on the bare skin of the unconscious person. A fully automatic defibrillator will automatically deliver a shock on not detecting a pulse, while a semi-automatic defibrillator will need you to press the shock button after clearance. AEDs provide audio-visual instructions for the layperson.
AEDs have multiple therapeutic advantages over conventional manual devices. They are easy to use, have simple interfaces (for laymen), can be time-saving (anyone can manage an AED and not wait for paramedics to arrive), and are completely safe for everyone. You might need to perform cardiopulmonary resuscitation (CPR) along with defibrillation to revive a person. Most advanced AEDs guide you on how to perform chest compressions and breaths.
References
[1] Nojima, T., Obara, T., Hongo, T., Yumoto, T., Naito, H., & Nakao, A. (2025). Differences in the Usability of Fully Automated External Defibrillators between Medical and Nonmedical Professionals.Internal Medicine,64(13), 1952-1954.
[2] Tung, D. (2024). Design and Development of Microneedle Pads for Automated External Defibrillators (AEDs).
[3] Coldewey, B., Klausen, A., Otto-Sobotka, F., Röhrig, R., & Lipprandt, M. (2024). Usability of automated external defibrillators: a randomized, comparative simulator study.International Journal of Human–Computer Interaction,40(22), 6972-6983.
[4] Zijlstra, J. A., Bekkers, L. E., Hulleman, M., Beesems, S. G., & Koster, R. W. (2017). Automated external defibrillator and operator performance in out-of-hospital cardiac arrest.Resuscitation,118, 140-146.
[5] Yu, J., Yu, Y., Liang, H., Zhang, Y., Yuan, D., Sun, T., … & Gao, Y. (2024). Defibrillation strategies for patients with refractory ventricular fibrillation: A systematic review and meta-analysis.The American Journal of Emergency Medicine,84, 149-157.
[6] Yin, R. T., Taylor, T. G., de Graaf, C., Ekkel, M. M., Chapman, F. W., & Koster, R. W. (2023). Automated external defibrillator electrode size and termination of ventricular fibrillation in out-of-hospital cardiac arrest.Resuscitation,185, 109754.
[7] Ruiz, J. M., de Gauna, S. R., González-Otero, D. M., Saiz, P., Gutiérrez, J. J., Veintemillas, J. F., … & Alonso, D. (2018). Circulation assessment by automated external defibrillators during cardiopulmonary resuscitation.Resuscitation,128, 158-163.
[8] Esibov, A., Chapman, F. W., Melnick, S. B., Sullivan, J. L., & Walcott, G. P. (2016). Minor variations in electrode pad placement impact defibrillation success.Prehospital Emergency Care,20(2), 292-298.
[9] Hawkes, C. A., Brown, T. P., Booth, S., Fothergill, R. T., Siriwardena, N., Zakaria, S., … & Perkins, G. D. (2019). Attitudes to cardiopulmonary resuscitation and defibrillator use: a survey of UK adults in 2017.Journal of the American Heart Association,8(7), e008267.
[10] U.S. Food and Drug Administration. (2023).AED adverse event reporting system: Safety and efficacy summary. https://www.fda.gov
[11] Josephson, M. E. (2014). Sudden cardiac arrest.Indian heart journal,66(Suppl 1), S2.
[12] Rees, N., Howitt, J., Breyley, N., Geoghegan, P., & Powel, C. (2021). A simulation study of drone delivery of Automated External Defibrillator (AED) in Out of Hospital Cardiac Arrest (OHCA) in the UK.Plos one,16(11), e0259555.
[13] Cheskes, S., McLeod, S. L., Nolan, M., Snobelen, P., Vaillancourt, C., Brooks, S. C., … & Drennan, I. R. (2020). Improving access to automated external defibrillators in rural and remote settings: a drone delivery feasibility study.Journal of the American Heart Association,9(14), e016687.