
{kind=link}

Ameloblastoma Rare Jaw Ameloblastoma, a benign but aggressive tumor of the jaw, is defined as: “A rare tumor that begins in the odontogenic epithelium (cells involved in tooth development, including enamel-forming tissues) and most often occurs in the jaw near the molars. Ameloblastomas are usually not cancerous, but they can grow significantly, typically present as painless swelling, and damage nearby tissue. Rarely, they may come back or spread to other parts of the body. They usually occur in adults.”[1] It occurs in various clinical presentations and histological types. They are primarily treated by surgical removal, followed by rehabilitation of the jaw in progressive lesions needing significant tissue removal and reconstruction.
Prevalence and Incidence of Ameloblastoma: Ameloblastoma Rare Jaw
Ameloblastoma is the second most common tumor with an odontogenic origin, and accounts for about 1% of all oral tumors. Conventional (solid/multicystic) ameloblastoma is the most common form. It usually affects people aged 20-40, with the mean age being 34 years old. It affects males and females equally, with a slight predisposition towards males (53%).[2]
Ameloblastoma most commonly occurs in the mandible (lower jaw), in almost 80-90% of the cases[3], but it can also affect the maxilla (upper jaw). Additionally, malignant transformation and metastasizing ameloblastoma are extremely rare, and incidence data are limited and variable.[4].
Causes of Ameloblastoma
Its exact cause is unknown, but it is linked to genetic mutations. Ameloblastoma, as the name suggests, arises from “Ameloblasts,” which are cells responsible for developing enamel. Once the enamel is formed, the ameloblastomas disappear, but some cells from the developing enamel organ can be left behind in the form of “epithelial rests.” These cells undergo genetic mutations that activate certain cell signalling pathways (MAPK).[5] Mutations involving the BRAF V600E gene (most common, especially in mandibular tumors) and the SMO gene (more common in maxillary lesions) are common in ameloblastomas.[6]
Symptoms of Ameloblastoma
Ameloblastomas are primarily tumors of the jaws. They are slow-growing, but locally invasive and destroy the tissues in their path. It can present as follows:
- Usually occur in the posterior mandible (lower jaw), but can also occur in the upper jaw.
- Painless swelling in the jaw that is slow-growing.
- Limited to one side of the jaw, causing facial asymmetry.
- Teeth may shift in that region or become loose and fall off, leading to malocclusion.
- Difficulty in opening the mouth or chewing.
- If a nerve is involved, it can cause an abnormal tingling feeling (paresthesia) in the area.

Ameloblastoma of the mandible presenting as a large facial swelling in an adult patient. Image source:Camazine, 2007.Licensed underCC-BY 3.0viaWikimedia Commons
Classification of Ameloblastoma
Ameloblastoma has many different types that can be classified based on clinical appearance, their malignant nature, and histological (cellular) patterns. It is classified by the WHO in the following manner:[7]
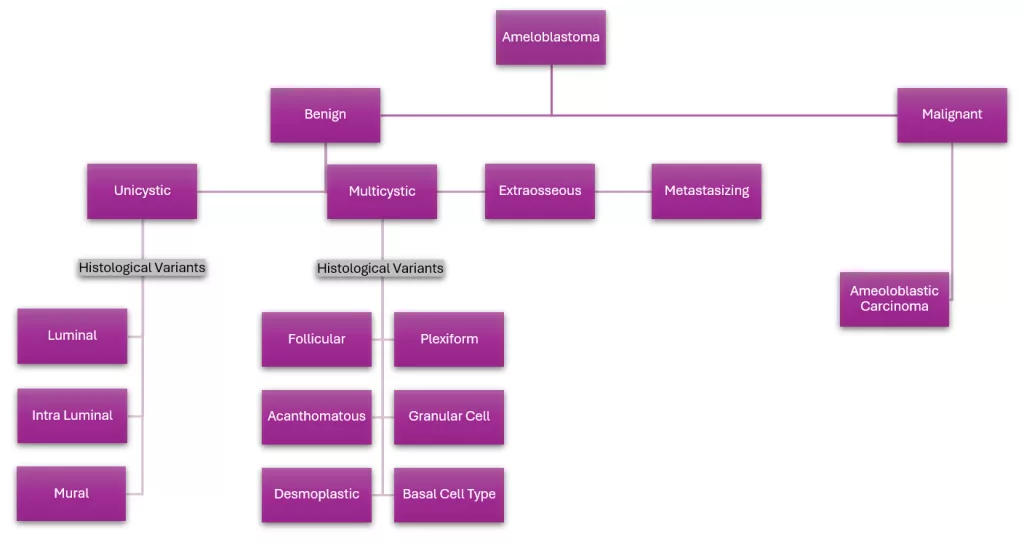
Classification of ameloblastoma showing benign and malignant types, with subtypes including unicystic, multicystic, extraosseous, and metastasizing forms, along with their histological variants.
Benign Ameloblastoma
There are four subtypes of benign ameloblastoma based on clinical and radiographic presentation:
1. Unicystic Ameloblastoma
As the name suggests, this type of ameloblastoma consists of a single cystic cavity. It is less aggressive than multicystic ameloblastoma. Subsequently, it shows a single cystic radiolucency on the radiograph, often around an impacted or unerupted tooth, mimicking a dentigerous cyst. Since it occurs in correspondence with unerupted teeth, it is usually seen in young patients aged 16 to 35 years of age, with no gender predisposition. It can be classified into three types based on histological patterns discussed in the next section.
2. Conventional (solid/multicystic) ameloblastoma
This is the most common type of ameloblastoma and accounts for 10% of all odontogenic tumors and 85% of all ameloblastic lesions. It is also called “conventional” or “solid” ameloblastoma. The lesions more often progress slowly, but are locally invasive and erode cortical bone. If left untreated, they resorb the cortical plate and extend into adjacent tissue. Radiographically, they show cortical expansion, a radiolucent, multiloculated cystic lesion, with a characteristic “soap bubble-like” appearance.[8] They have six distinct histological variants discussed in the next section.
3. Extraosseous Ameloblastoma
Also known as peripheral ameloblastoma, it does not occur in the bone but rather in the gums. Hence the name “extraosseous.” The mandibular premolar region is the most common site. Since it does not involve the bone and is an exophytic growth of the soft tissues, it is usually mistaken for epithelial lesions such as fibroma, papilloma, etc. It has a good prognosis with a low recurrence rate.
4. Metastasizing Ameloblama
It is a type of benign ameloblastoma that metastasizes to other regions, primarily the lungs. Under the microscope, the cells appear benign and do not show any malignant changes. It is currently classified as a distinct entity that is histologically benign but clinically behaves in a malignant manner.
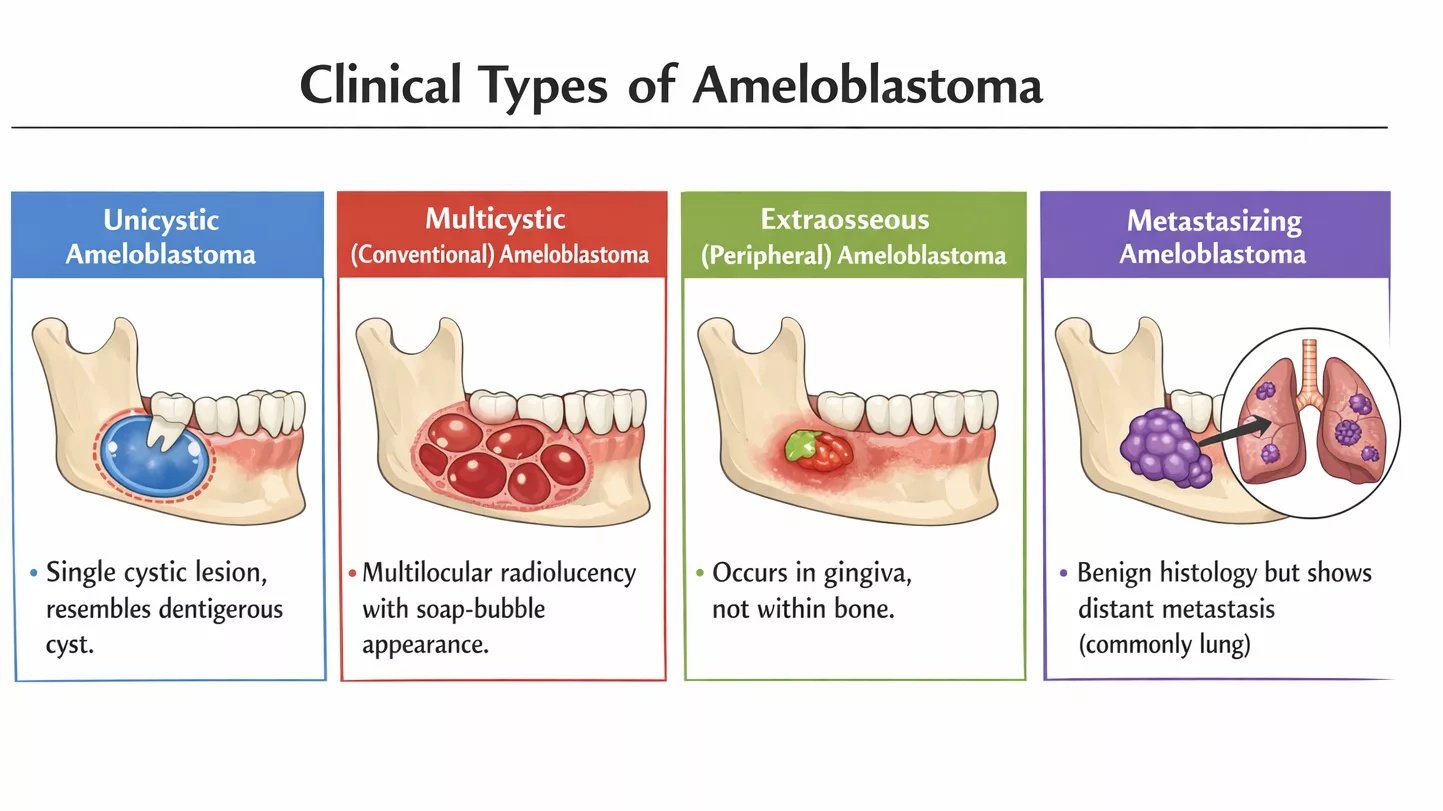
Clinical comparison of different types of ameloblastoma: unicystic, multicystic, extraosseous, and metastasizing. (Ai-generated)
Malignant Ameloblastoma
Ameloblastic Carcinoma[9] is the only malignant variant of ameloblastoma. They are rare, rapidly progressive, and may occur spontaneously or via malignant transformation of existing lesions. Being malignant in nature, they have a high recurrence rate and a poor prognosis.
Histopathology of Ameloblastoma
Since Ameloblastoma is a tumor of odontogenic origin, it primarily consists of islands of epithelial cells, the same kind seen in the developing enamel organ. Tall columnar basal cells make up the outer layer of these islands, and they resemble ameloblasts. This arrangement is referred to as “peripheral palisading of cells.” These peripheral palisading basal cells have reverse polarity, i.e., their nuclei are placed away from the membrane. Subnuclear vacuolization may also be present. In the middle of these islands, star-shaped cells are present that resemble the stellate reticulum of the developing enamel organ. These are the basic cells present in an Ameloblastoma, but the configuration of these cells can differ.
Unicystic Ameloblastoma
A “cyst” has two components: a capsule lining and a cystic cavity called “lumen.” It is classified into three histological categories based on its different invasion patterns:[10]
1. Luminal
When the extension of the tumor remains limited to the connective tissue present in the capsule’s luminal surface, lined by epithelium, this variant is called luminal.
2. Intraluminal
When the tumor grows and expands its nodular extensions into the cyst lumen, but does not invade the capsule wall, it is called intraluminal.
3. Mural
The islands of epithelium cells invade the capsule lining, and infiltrate the connective tissue wall, it’s called mural or intramural. It is the most aggressive variant and behaves like aggressive ameloblastoma.
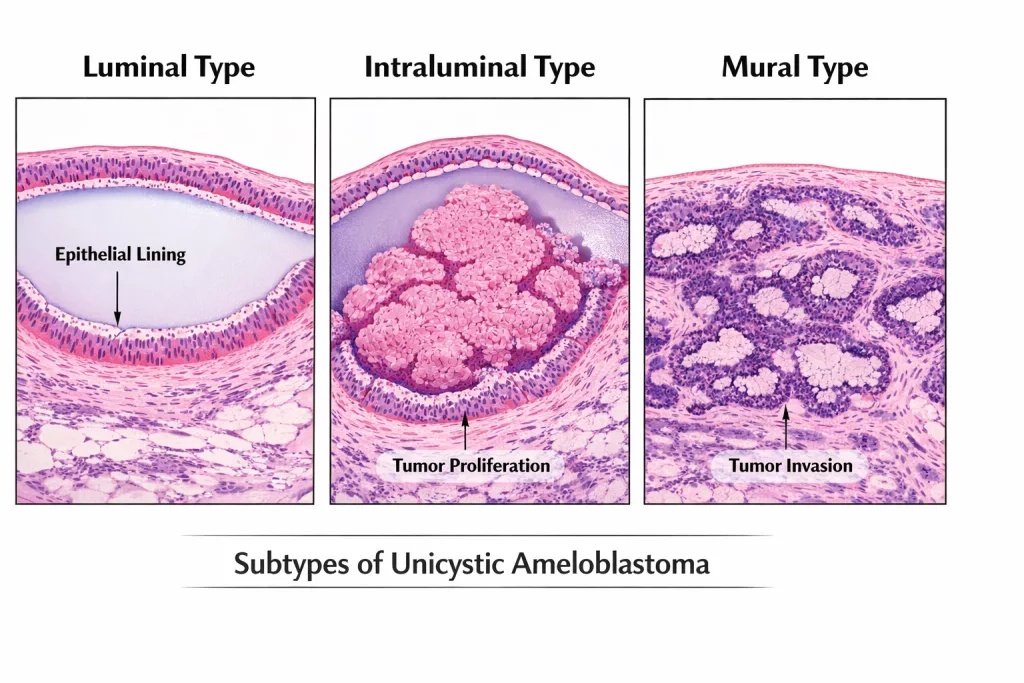
Histological comparison of unicystic ameloblastoma showing luminal, intraluminal, and mural subtypes.
Solid/Multicystic Ameloblastoma
It is classified into six categories based on its different histological patterns:
1. Follicular pattern:
This is the most common histological pattern of multicystic ameloblastoma. The pattern is evident by its name, “follicular.” Hence, the cells are arranged in small follicles or islands surrounded by connective tissue. The centre of the islands contains epithelial cells, and they are lined on the outside by peripheral palisading basal cells.
2. Plexiform pattern:
Plexiform means having a continuous interlacing network. The epithelial cells form a complex network, each island communicating with the next. Basal cells line these interconnected cords, and connective tissue is present on the outside of these strands.
3. Acanthomatous pattern:11Singh G, Agarwal R, Kumar V, Passi D. Acanthomatous Ameloblastoma- A Case Report. Journal of International Oral Health : JIOH [Internet]. 2013 Apr 21 [cited 2026 Mar 19];5(2):54.
The arrangement of the cells is similar to the follicular pattern, with individual islands of epithelial cells lined by basal cells and surrounded by connective tissue. However, the star-shaped stellate reticulum-like cells present in the middle of the epithelial islands undergo squamous metaplasia and convert into squamous cells. These squamous cells produce keratin and are hence characterized by the excessive formation of keratin.
4. Granular pattern:12Nikitakis NG, Tzerbos F, Triantafyllou K, Papadimas C, Sklavounou A. Granular Cell Ameloblastoma: an Unusual Histological Subtype Report and Review of Literature. Journal of Oral and Maxillofacial Research. 2010 Oct 27;1(4).
This subtype is characterized by the presence of large granular cells in the centre of the epithelial islands. These granular cells have a lot of eosinophilic granules that are believed to be lysosomes, often linked to metabolic dysfunction, degenerative changes, or increased apoptosis (cell death) within the tumor. Usually located in the posterior mandible, they are more aggressive and have a higher chance of recurrence after surgery.
5. Desmoplastic pattern:13Sun ZJ, Wu YR, Cheng N, Zwahlen RA, Zhao YF. Desmoplastic ameloblastoma – A review. Oral Oncology. 2009 Sep;45(9):752–9.
“Desmoplasia” refers to the growth of connective tissue. Hence, as the name suggests, this subtype is characterized by increased growth of the collagen matrix and connective tissue, making it dense, thick, and hypocellular. Consequently, this connective tissue growth results in the epithelial islands becoming condensed and squashed, resulting in an irregular shape. On radiographs, it has a mixed radiolucent-radioopaque lesion. Additionally, it is locally aggressive and has a tendency to recur.
6. Basal cell pattern:14Sridhar M, Bhaskar Reddy Lr, Kharat S, Mahesh B, Gandi L, Mahendra A, et al. Basal cell ameloblastoma: A rare histological variant of an uncommon tumor. Nigerian Journal of Surgery. 2015;21(1):66.
The islands consist of tightly packed polyhedral basaloid cells that are deeply basophilic (stained dark purple). Correspondingly, they histologically resemble basal cell carcinoma and need to be differentiated via immunohistochemistry and clinical presentation.

Comparison of the main histopathological types of solid/multicystic ameloblastoma and how they look under the microscope. (AI-generated)
Radiology of Ameloblastoma
OPG is the first line radiograph for initial viewing, followed by CBCT for more detailed imaging. The radiographic features of ameloblastoma are as follows:
- It is a radiolucent lesion, predominantly present in the posterior mandible.
- It is well-demarcated with corticated or scalloped borders, showing expansion of the bony cortices.
- It is often multilocular, giving a “soap-bubble” appearance on the OPG; however, it can also be a single unicystic cavity.
- Roots of the surrounding teeth are often resorbed due to the tumor’s aggressive nature.

CT scan showing an ameloblastoma arising from the left mandibular third molar region. Image Source:Berto1286, 2008 viaWikimedia Commons
Diagnosis of Ameloblastoma
Your doctor will diagnose your condition based on clinical examination, radiographic findings, and a biopsy. The clinical examination and history will confirm its slow-growing expansile nature, and the radiographs will express radiolucent unicystic or multicystic lesions. After performing these preliminary examinations, a biopsy will be mandatory to see the cells under the microscope and diagnose the lesion. Differential diagnoses include dentigerous cyst, odontogenic keratocyst, central giant cell granuloma, and odontogenic myxoma.
Treatment of Ameloblastoma
Ameloblastomas are primarily treated via surgery. Different types of surgeries can be performed based on the type of lesion and its location. Radiotherapy and chemotherapy generally have limited effectiveness in benign ameloblastoma but may be considered in unresectable or malignant cases.
Radical Surgery
Complete surgical removal of the lesion, along with a wide margin (1-1.5cm) of healthy bone, is done in aggressive multicystic lesions. The wide margin of healthy bone removed prevents recurrence. The surgery includes a complete en bloc resection and can be a segmental or marginal removal. However, despite providing a margin of safety, conventional therapy results in increased removal of bony tissue and facial deformity.
Conservative Surgery
To prevent excessive removal of healthy bone, conservative methods have been tried to preserve facial anatomy and aesthetics. This method is usually done in unicystic ameloblastoma and include:[11]
- Marsupialization: The lesion is first decompressed, reducing its size. This protects the surrounding vital structures and preventsfractures of the jaw. It is then followed by enucleation or currettage.
- Enucleation: The tumor is carefully removed with its lining intact. It can be combined with marginal osteotomy or Carnoy’s solution to reduce recurrence.
- Curretage: The lesion is removed from within the bony cavity, followed by removal of 5-10mm of surrounding healthy bone. This can be combined with marsupialization and enucleation, but this method has a high recurrence rate and needs to be monitored carefully.
Rehabilitation and Post-operative care
Once the lesion and surrounding bone are removed, the area needs to be filled immediately to improve function and aesthetics. To achieve that, bone grafting (usually from the leg) is the gold standard. After healing of the grafts, functional rehabilitation is provided via dental implants.[12] In addition, a screw-retained hybrid prosthesis can be used to position the dental implants better.
After surgery and reconstruction, follow-up for up to 5 years is mandatory to check for recurrence. The significant changes to facial aesthetics may necessitate mental health support to manage emotional impact. Speech therapists and nutritionists help patients regain jaw function and adjust to dietary changes.
Conclusion
Ameloblastomas are rare, slow-growing, locally invasive tumors of odontogenic origin. Despite being benign in nature, they can cause significant bone and tissue damage, leading to facial deformity. Its aggressive nature calls for an early and accurate diagnosis. It occurs in various clinical presentations and histological variants, each with a different treatment and prognosis. Hence, accurate diagnosis is crucial for treatment planning. It has a high recurrence rate if not properly treated. Comprehensive management, including timely intervention and proper post-operative rehabilitation, is key to minimizing complications and improving patient outcomes.
References
[1] NCI Dictionary of Cancer Terms [Internet]. Cancer.gov. 2025.
[2] Hendra FN, Van Cann EM, Helder MN, Ruslin M, de Visscher JG, Forouzanfar T, et al. Global incidence and profile of ameloblastoma: A systematic review and meta‐analysis. Oral Diseases. 2019 Jan 25;26(1):12–21.
[3] França LJ de L, Curioni OA, Paiva DL, Vianna DM, Dedivitis RA, Rapoport A. Estudo demográfico, clínico e terapêutico do ameloblastoma: análise de 40 casos. Brazilian Journal of Otorhinolaryngology [Internet]. 2012 Jun 1 [cited 2023 Sep 26];78:38–41.
[4] Palanisamy JC, Jenzer AC. Cancer, Ameloblastoma [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020.
[5] Palanisamy JC, Jenzer AC. Cancer, Ameloblastoma [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020.
[6] Ameloblastoma: What it is, Histology and Radiology [Internet]. Cleveland Clinic.
[7] Soluk-tekkesin M, Wright JM. The World Health Organization classification of odontogenic lesions: a summary of the changes of the 2022 (5th) edition. Turkish Journal of Pathology. 2022;
[8] Manikkam S, Masthan KMK, Anitha N, Krupaa J. Ameloblastoma. Journal of Pharmacy and Bioallied Sciences. 2015;7(5):169.
[9] Ram H, Mohammad S, Husain N, Gupta PN. Ameloblastic Carcinoma. Journal of Maxillofacial & Oral Surgery [Internet]. 2010 Dec 1;9(4):415–9.
[10] Chaudhary Z, Sangwan V, Pal US, Sharma P. Unicystic ameloblastoma: A diagnostic dilemma. National Journal of Maxillofacial Surgery [Internet]. 2011;2(1):89–92.
[11] Singh G, Agarwal R, Kumar V, Passi D. Acanthomatous Ameloblastoma- A Case Report. Journal of International Oral Health : JIOH [Internet]. 2013 Apr 21 [cited 2026 Mar 19];5(2):54.
[12] Nikitakis NG, Tzerbos F, Triantafyllou K, Papadimas C, Sklavounou A. Granular Cell Ameloblastoma: an Unusual Histological Subtype Report and Review of Literature. Journal of Oral and Maxillofacial Research. 2010 Oct 27;1(4).
[13] Sun ZJ, Wu YR, Cheng N, Zwahlen RA, Zhao YF. Desmoplastic ameloblastoma – A review. Oral Oncology. 2009 Sep;45(9):752–9.
[14] Sridhar M, Bhaskar Reddy Lr, Kharat S, Mahesh B, Gandi L, Mahendra A, et al. Basal cell ameloblastoma: A rare histological variant of an uncommon tumor. Nigerian Journal of Surgery. 2015;21(1):66.
[15] Ghai S. Ameloblastoma: An Updated Narrative Review of an Enigmatic Tumor. Cureus. 2022 Aug 6;14(8).
[16] Kalavathy N, Premnath K, Jayanthi N, Jadav V. Prosthetic Rehabilitation of Patient with Ameloblastoma: A Case Report. The Journal of Indian Prosthodontic Society [Internet]. 2011 Jun 21;11(4):238–41.