
, also known as hereditary enamel dysplasia, hereditary brown opalescent teeth, or...){kind=link}

Amelogenesis Imperfecta Complete Amelogenesis imperfecta (AI), also known as hereditary enamel dysplasia, hereditary brown opalescent teeth, or hereditary brown enamel, is a rare dental disorder characterized by the formation of weak and discolored teeth (having brown-yellow coloration). The genetic disorder arises due to developmental defects in the outer hard layer of the tooth, i.e., enamel. Weakening of the enamel leads to aesthetic issues, functional problems, and frequent tooth decay. The disorder is very rare, having a prevalence of 1:700 to 1:14,000.[1] AI can affect both deciduous (milk teeth) and permanent dentitions. Thus, patients require extensive dental treatments throughout their lives. Dentists treat the condition with restorative and cosmetic therapies.
What Is Amelogenesis Imperfecta?: Amelogenesis Imperfecta Complete
“Amelogenesis” means the biological process of enamel formation, and “imperfecta” means faulty or damaged. So, amelogenesis imperfecta means faulty biological development of tooth enamel. It is a genetic disorder that affects the normal development of the hardest, outer tooth layer. The ultimate result of altered tooth development is the formation of milk and permanent teeth that are weak, unaesthetic, and prone to breakage. Defects can take place at different levels of amelogenesis. Hence, it is important to learn about enamel formation first!
Amelogenesis: The Process Of Enamel Formation
Ameloblasts are specialized cells that create enamel (the hardest substance in the human body). Experts divide amelogenesis into three stages.
In the pre-secretory stage, the epithelial cells (a fundamental tissue covering all bodily surfaces) differentiate into the specialized cells, i.e., ameloblasts. The next stage is called the secretory stage and is characterized by the secretion of an organic matrix by the ameloblasts. This matrix contains proteins like amelogenin and enamelin that constitute the structure of enamel. In the third stage/maturation stage, ameloblasts carry out the degradation/removal of the organic materials, which is followed by the final mineralization of enamel. Errors at the different stages of enamel development and mineralization lead to AI.
Amelogenesis Imperfecta Types
Based on the underlying cause of weak enamel, experts divide amelogenesis imperfecta into 4 main types:
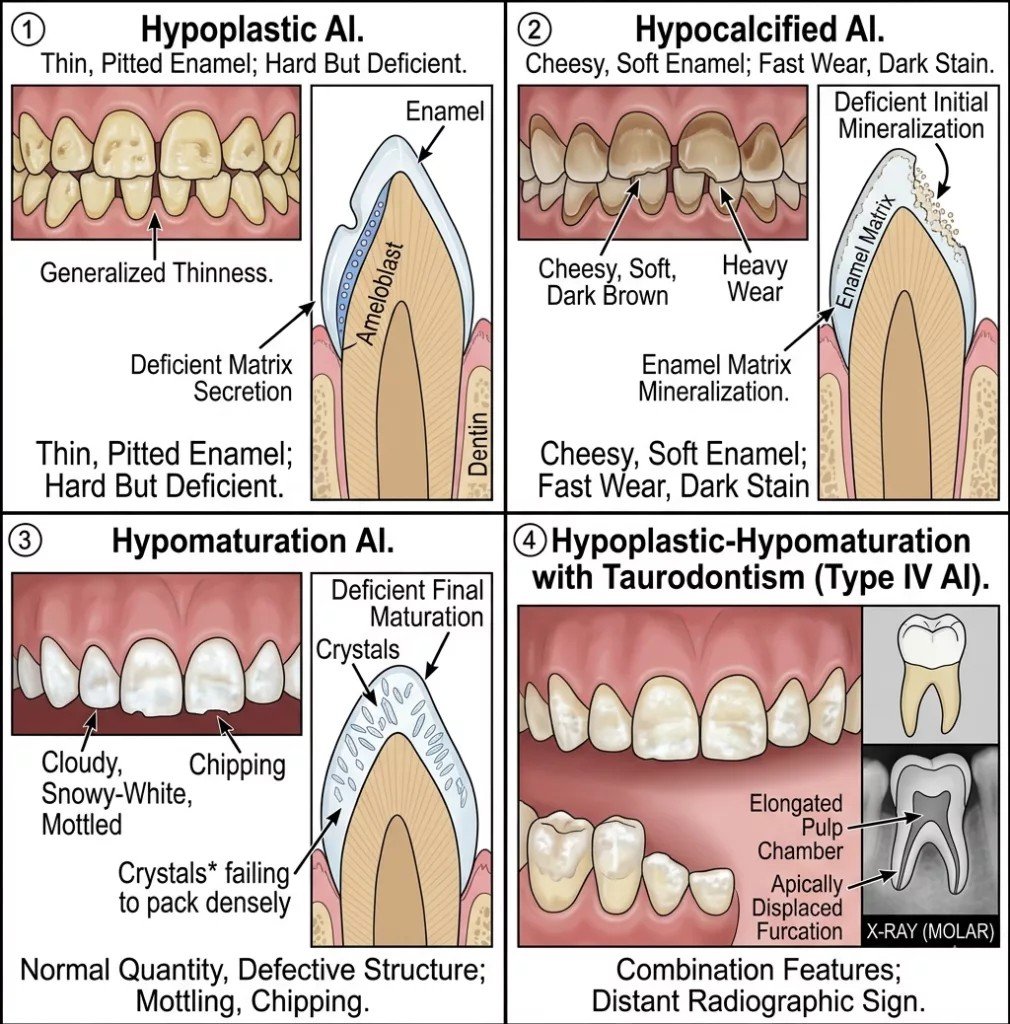
The different types of amelogenesis imperfecta. 1st image shows a hypoplastic type with a thin enamel layer, 2nd image shows a hypocalcified type with deficient mineralization, 3rd image shows a hypomaturation type with an immature enamel layer, and 4th image shows an enamel defect with an elongated tooth and enlarged chamber (taurodontism)
Type Ⅰ: Hypolastic AI
Hypoplasia refers to defective enamel matrix formation (or underdeveloped cells), leading to amelogenesis imperfecta. Individuals with AI type Ⅰ have a thin layer of enamel. You can also notice smaller-than-average teeth with rough surfaces. In a study, hypoplastic type was found to be the most common type of AI (54%), followed by hypomaturation type (36%) and hypocalcified type (10%).[2]
Type Ⅱ: Hypomaturation AI
In this type, sufficient enamel cells are produced, and the enamel layer may be of normal (or near normal) thickness. However, this type arises due to maturation failure. A lack of proper maturation results in a softer outer layer, prone tochipping despite appearing normal in thickness.
Type Ⅲ: Hypocalcified AI
The third type arises when an error occurs in the mineralization stage. As already discussed, in the final stage, the enamel structure is made robust with the addition of minerals like calcium. When insufficient calcium is added to the structure, the final enamel layer is prone to wearing/chipping despite having a normal thickness.
Type Ⅳ: Hypomaturation/Hypoplastic With Taurodontism
In this particular type, you will see a combination of both types Ⅰ and Ⅱ, which means that the enamel layer is thin and immature. Moreover, the patient usually suffers from a condition called taurodontism. In this disease, abnormal development of enamel results in a very large tooth body with very short roots.
Cases of type Ⅳ amelogenesis imperfecta associated with taurodontism present with pyramidal maxillary first molars. Pyramidal molars are cone-shaped teeth having completely fused roots (into a single root) with an enlarged root canal. Moreover, taurodontism patients are also prone to developing cardiac complications (heart diseases).[3] The unusual tooth proportions with enamel weakness make treatment even more difficult.
Amelogenesis Imperfecta Symptoms
Enamel is meant to protect the tooth against wear/tear and microbial invasion, while imparting an esthetic appearance. Thus, abnormal enamel not only gives you functional impairments but also affects esthetics.
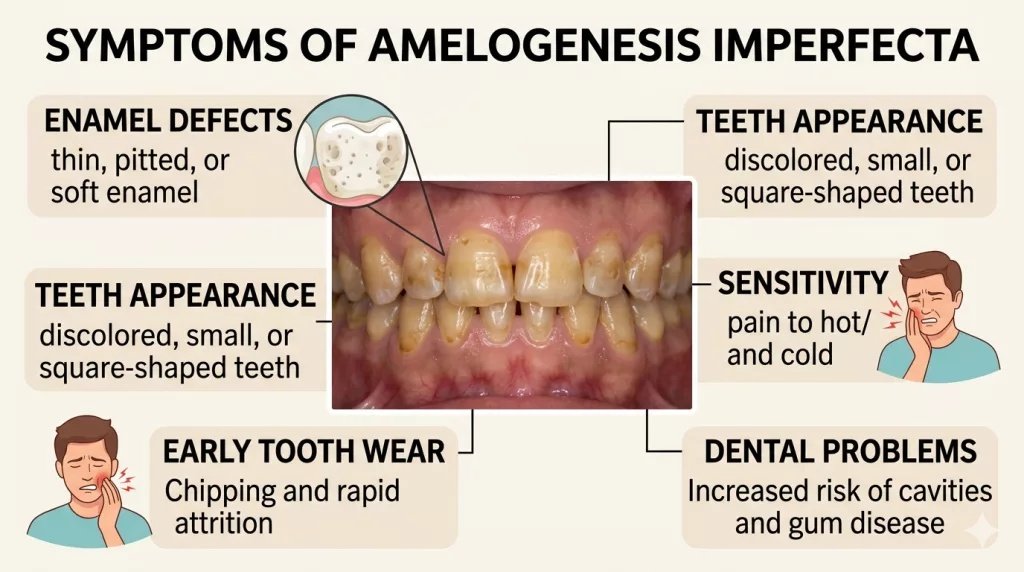
The most common symptoms reported by patients include:
Discolored Teeth
The vast majority of patients are concerned about the altered coloration of their teeth. The shade of your teeth can vary from chalky white to yellow and even brown. Yellow-brown teeth with thin enamel are frequently seen in the hypoplastic type. On the other hand, the teeth of individuals with hypomaturation type exhibit opaque to brown coloration. In type 3 AI, enamel color can range from white to creamy yellow.[4]
MalocclusionMalocclusion
The disorder is also characterized by the formation of atypically small teeth. While natural teeth align perfectly in all dimensions, teeth with faulty enamel lack the normal height and width. A lesser width of teeth means visible gaps between the teeth. For many people, multiple interdental gaps (between two teeth) are a major reason to get dental reconstruction.[5]
On the other hand, the inability of a tooth to gain height potentially leads to an open bite. An open bite is a condition in which your top and bottom teeth do not meet properly when you close your mouth. AI patients usually present with a dental anterior open bite (open bite in front teeth due to tooth issues).[6] Hence, malocclusion is a salient feature of the disorder, which causes esthetic and functional issues.
Rough And Pitted Teeth
The abnormally formed enamel usually has pitting and a rough texture. Patients notice abnormal grooves running through their teeth. Studies show that the majority of patients have a generalized thin enamel with defective grooves and pits in teeth that negatively affect the appearance.[7]
Psychological Impact
Most amelogenesis imperfecta patients are conscious about their smile profiles. Discolored, weak teeth with interdental gaps make patients conscious of their dental display. This is why many individuals avoid smiling in gatherings. Studies show that young children are disturbed more by the functional issues, but youngsters experience significant psychosocial distress.[8]
AI has a direct and evident impact on oral health-related quality of life (OHRQoL).[9]
Tooth Sensitivity
Sensitivity to hot/cold food items is also a frequent complaint of patients. In a normal tooth, enamel covers the sensitive dentin layer. The thin and weak enamel exposes the underlying dentin, which presents with hot/cold sensitivity. In numerous cases, dentists adopt restorative therapy just to alleviate hypersensitivity and pain.[10]
Weak Teeth
The weakened enamel offers no resistance against masticatory forces and trauma. The poorly formed, short/thin teeth are prone to chipping and wearing away. Clinicians frequently note attrition of occlusal surfaces of molars andchipping of incisal edges of incisors (front teeth) in such patients. Malformed enamel increases your probability of enamel chipping, eventually leading to dentin and pulp exposure.[11]
{kind=link}
Complications Of Amelogenesis Imperfecta
A lack of proper protective covering exposes your teeth to numerous complications. Most AI patients require dental treatments throughout their lives. The most common complications arising from imperfect enamel include:
Tooth Decay
Patients have a higher propensity to develop cavities and consequent tooth decay than people with normal enamel. Therefore, tooth decay is frequently seen in AI, and doctors try to restore the decayed teeth as early as possible.[12]
Tooth Erosion
The weak enamel is unable to bear the wear and tear of mastication. Clinicians notice early and excessive erosion of teeth (especially in the molars). Erosion further leads to other complications like increased chances of infection, pain, and TMJ disorders.
Dental Pain
Several factors associated with hereditary enamel dysplasia cause tooth pain. Exposed dentin and pulp due to thin/missing enamel contribute to pain (on consuming hot/cold items). An ache in the tooth can cause a lot of trouble in pediatric patients.
Out of fear of dental issues, many patients are hesitant to maintain good oral hygiene, which also makes them prone to gum disease.
Amelogenesis Imperfecta Causes
This disorder arises when there is a mutation of one (or more) genes that regulate the production of tooth enamel. Genes are part of your DNA structure that perform/oversee specific functions. AI-related gene mutations can affect both primary and permanent teeth. Thus, the disorder can be observed in children and adults.
Genetic Mutations
Mutations can be of two types, i.e., hereditary or acquired. A hereditary mutation means you get the faulty (mutated) gene from your biological parents. In the acquired type, you receive a normal gene but develop a mutation later in life.
Genes Involved:
Several genes govern the process of amelogenesis. Some genes control enamel maturation, and others oversee mineralization. Researchers have noticed the following genes in amelogenesis imperfecta:
- FAM83H
- ENAM
- MMP20
- AMELX
- ACP4
- FAM20A
- WDR72
Inheritance Pattern:
There are specific patterns of transmission of the mutated genes from parents to the offspring. You can fall prey to enamel dysplasia in the following patterns:
Autosomal Dominant:
Inheritance experts notice that most cases of AI are autosomal dominant. In this pattern, a mutated gene from one parent is passed on to the child and causes the disease.
Latest research shows that the FAM83H gene mutation is a common cause of amelogenesis issues that is inherited in an autosomal dominant pattern.[13] Variants of the AMELX gene can also contribute to the disorder.[14]
Autosomal Recessive:
In the autosomal recessive type of inheritance, you get a mutated gene from both parents. As the gene is recessive, you need a copy from both parents for the disease to develop. The acid phosphatase 4 (ACP4) gene is a recessive gene that, when mutated, leads to hypolastic AI.[15]
It was concluded in a study on the Pakistani population that the WDR72 and FAM20A genes are responsible for autosomal recessive amelogenesis imperfecta.[16]
Sex Chromosome:
Sometimes, you can inherit the mutation on the X chromosome (sex chromosome). X-linked amelogenosis issues are more noticeable in male children than female children. This is attributed to the fact that two X chromosomes mitigate the disease effects. Men have only one X chromosome (and a Y chromosome), thus, more complications.
Amelogenesis Imperfecta Diagnosis
In the vast majority of cases, the disease is diagnosed at a young age. Your dentist will identify the condition during a dental examination. After observing the discolored/pitted teeth, your dentist will ask about your family history of similar dental problems. For better diagnosis, your dental surgeon will order imaging studies.
Imaging Scans
Conventional dental radiographs (X-rays) provide sufficient details about the hypoplastic/hypomineralized enamel to reach the diagnosis of amelogenesis imperfecta.
Genetic Testing
Once a diagnosis of AI is made, doctors may advise genetic testing to identify the specific mutation that has led to the dental deformity.
Differential Diagnosis
This tooth developmental disorder can have presentations similar to other dental maladies. Clinicians need to know the difference between similar infirmities to provide better healthcare and treatment options.
Amelogenesis Imperfecta (AI) Vs Dentinogenesis Imperfecta (DI)
Both are hereditary disorders that impact the development of a tooth. While AI affects the outer layer (enamel), DI disrupts the development of the inner layer (dentin). AI presents with yellow/hypocalcified teeth. On the other hand, DI is characterized by opalescent teeth and early enamel loss due to defective dentin support.
Amelogenesis Imperfecta Treatment
Usually, treatment starts at a young age (milk teeth in pediatric patients) and continues in adulthood. The main aim of the modalities offered is to save the teeth from further degradation and restore function and aesthetics. Commonly adopted treatment options include:
Restorative Treatment
Covering up, restoring the weak teeth with solid dental materials, is a widely adopted therapy for AI patients. In children and young adults, doctors go for strong ceramic restorations to restore function.[17]
In most cases, dentists place dental crowns over the fragile teeth to protect them from wearing out (due to masticatory forces). For severely damaged teeth, doctors go for the extraction of the teeth that are replaced by prosthetics like dentures, bridges, or implants, etc.
Cosmetic Treatments
Doctors offer this modality to individuals looking to improve their appearance. Dental veneers are minimally designed artificial teeth that cover up your teeth without the need for extensive tooth preparation (as required in crowns). Thus, your teeth no longer appear chipped, worn out, and discolored.

Dental veneers efficiently cover the defective teeth and change your appearance.
Teeth whitening can help convert the shade from yellow-brown to whiter. However, the results are not long-lasting. It can only improve the color but not offer any protection against the disintegration of the tooth. Teeth whitening is often limited in effectiveness and may increase sensitivity in AI patients.
Orthodontic Treatment
Malocclusion is common in AI. So, orthodontists fix the misaligned teeth and bites with braces and aligners.
Final Word
Amelogenesis imperfecta (AI) is a rare, hereditary disorder characterized by weak, discolored (yellow), hypersensitive, and easily chipped teeth. The disorder arises due to problems in the process of enamel formation, i.e., amelogenesis. Genetic mutations in any of the genes (ENAM, FAM83H, AMELX, etc.) lead to the disorder. AI can follow autosomal dominant, autosomal recessive, or X-linked inheritance patterns.
The enamel disorder is categorized into 4 types, i.e., hypoplastic, hypomaturation, hypocalcified, and AI with taurodontism. Patients present with thin enamel, having a yellow-brown color, and pits/grooves that are prone to chipping/fracturing. Due to the weak outer layer, several patients experience hypersensitivity to hot/cold (due to dentin exposure) and consequent tooth pain. Such individuals are at a greater risk of tooth decay, infection, and psychosocial distress (due to their appearance).
Doctors treat the condition with restorative options like crowns and prosthetics, such as implants and dentures (in cases where teeth can not be saved). A ceramic restoration is the go-to treatment option for pediatric patients. Adults concerned about the appearance of their front teeth may opt for dental veneers and whitening procedures. Orthodontic treatment (with fixed braces, aligners) is needed in most cases due to the high prevalence of malocclusion in AI cases.
References
[1] Crawford, P. J., Aldred, M., & Bloch-Zupan, A. (2007). Amelogenesis imperfecta.Orphanet journal of rare diseases,2(1), 17.
[2] Saleh, S. S. B. (2023). Etiology, classification, and restorative management of amelogenesis imperfecta among children and young adults: a scoping review.Cureus,15(12).
[3] Ozgur, O. M., Seyma, M., Aynur, K., & Nazan, K. T. (2025). Taurodontism and related dental anomalies: influence of maternal, prenatal, and postnatal factors in pediatric patients.BMC Oral Health,25(1), 1526.
[4] Bloch-Zupan, A., Rey, T., Jimenez-Armijo, A., Kawczynski, M., Kharouf, N., Dure-Molla, M. D. L., … & International Consortium. (2023). Amelogenesis imperfecta: Next-generation sequencing sheds light on Witkop’s classification.Frontiers in Physiology,14, 1130175.
[5] Marghalani, A. A. (2026). Full-Mouth Reconstruction in Amelogenesis Imperfecta: A Case Report.The American Journal of Case Reports,27, e951835.
[6] Messaoudi, Y., Kiliaridis, S., & Antonarakis, G. S. (2023). Craniofacial cephalometric characteristics and open bite deformity in individuals with amelogenesis imperfecta—a systematic review and meta-analysis.Journal of clinical medicine,12(11), 3826.
[7] Wang, S. K., Zhang, H., Wang, Y. L., Seymen, F., Koruyucu, M., Simmer, J. P., & Hu, J. C. C. (2023). Phenotypic variability in LAMA3‐associated amelogenesis imperfecta.Oral diseases,29(8), 3514-3524.
[8] Altaher, J. (2025).Exploring the impact of amelogenesis imperfecta on oral health related quality of life in children and young persons(Doctoral dissertation, UCL (University College London)).
[9] Appelstrand, S. B., Robertson, A., & Sabel, N. (2022). Patient-reported outcome measures in individuals with amelogenesis imperfecta: a systematic review.European Archives of Paediatric Dentistry,23(6), 885-895.
[10] Lundgren, G. P., & Dahllöf, G. (2024). Advances in clinical diagnosis and management of amelogenesis imperfecta in children and adolescents.Journal of Dentistry,147, 105149.
[11] Jha, K., Adhikari, M., Shrestha, S., & Pandey, A. (2024). Orthodontic management of amelogenesis imperfecta: A case report.Clinical Case Reports,12(8), e9329.
[12] Jha, K., Adhikari, M., Shrestha, S., & Pandey, A. (2024). Orthodontic management of amelogenesis imperfecta: A case report.Clinical Case Reports,12(8), e9329.
[13] Kamps, R., Martens, H., de Koning, B., Smeets, B., & van Geel, M. (2025). Identifying a Novel Causal FAM83H Variant for Autosomal Dominant Amelogenesis Imperfecta Using Exome‐Sequencing.Molecular genetics & genomic medicine,13(6), e70108.
[14] Yang, S., Wan, M., & Zheng, L. (2025). Amelogenesis Imperfecta: AMELX Novel Variant And Management.International Dental Journal,75, 104974.
[15] Kim, Y. J., Lee, Y., Kasimoglu, Y., Seymen, F., Simmer, J. P., Hu, J. C., … & Kim, J. W. (2022). Recessive mutations in ACP4 cause amelogenesis imperfecta.Journal of Dental Research,101(1), 37-45.
[16] Ullah, S., Khan, S. A., Jan, S., Din, S. U., Muhammad, N., Rehman, Z. U., … & Khan, S. (2026). Truncated Variants in FAM20A and WDR72 Genes Underlie Autosomal Recessive Amelogenesis Imperfecta in Four Pakistani Families.Biochemical Genetics,64(1), 1311-1323.
[17] Rhaiem, M., Chalbi, M., Bousaid, S., Zouaoui, W., & Chemli, M. A. (2024). Dental treatment approaches of amelogenesis imperfecta in children and young adults: A systematic review of the literature.Journal of Esthetic and Restorative Dentistry,36(6), 881-891.