
 is caused by the formation of fibrous strands (amniotic bands) within the amniotic sac that entangle and constrict...){kind=link}

Amniotic band syndrome (ABS) is caused by the formation of fibrous strands (amniotic bands) within the amniotic sac that entangle and constrict fetal body parts during development. The amniotic sac is the protective membrane that surrounds the fetus in the uterus, consisting of two layers: the outer chorion and the inner amnion. It also contains amniotic fluid, which cushions and protects the developing fetus. In ABS, fibrous strands from a disrupted amnion wrap around fetal limbs or other structures, restricting blood flow and causing a variety of congenital anomalies.[1]
These anomalies include constriction rings around fingers or toes, fusion of digits (syndactyly), or even limb amputation, etc. The degree of severity of BS depends on the degree of constriction and the affected body parts of the neonate. In extreme cases, it can even lead to intrauterine fetal death. Other names for this condition include amniotic band sequence, constriction band syndrome, and amniotic disruption complex. The estimated incidence of ABS ranges from 1 in 1,200 to 1 in 15,000 live births.[2] According to the Amniotic Band Syndrome ICD-10 classification (Q79.8), this condition is categorized under congenital malformations of the musculoskeletal system.
Amniotic Band Syndrome Causes
The exact etiology of the condition is not known, but researchers have proposed two main theories: the Extrinsic and intrinsic theories. The most accepted one is the extrinsic theory.
Extrinsic Theory:
This theory suggests that ABS results from early rupture of the amnion, which allows fibrous strands to float freely in the amniotic fluid. These strands can entangle the fetus and cause constrictions around developing body parts. The rupture may occur due to trauma, infection, or polyhydramnios (excess amniotic fluid). Not all cases that result from membrane disruption are often visualized on prenatal ultrasound.[3]
Intrinsic Theory:
This theory proposes that ABS arises from vascular disruptions within the fetus. Impaired blood flow in certain developing regions leads to tissue injury, hemorrhage, and necrosis, resulting in malformations that resemble amniotic band effects. For instance, in areas where tissue perfusion is low, inflammation or injury occurs to the blood vessel walls of the fetus. This results in hemorrhage and subsequent tissue damage and tissue loss in affected areas.
Hence, the underlying cause can be heterogeneous, so the ABS is generally not inherited or genetic. However, certain factors may increase the risk, such as:
- Pre-mature births
- First pregnancy
- Genetic females of African American descent
- Taking a prostaglandin analog during pregnancy
- Prenatal tests such as amniocentesis or chorionic villus sampling. These tests puncture the amniotic sac with a needle to get tissue or fluid from the fetus. However, damage can occur very rarely.
- Fetoscopic laser surgery in monozygotic twin pregnancies or thoracoamniotic shunt placement
- Maternal smoking, drug use, or connective tissue disorders such as vascular Ehlers–Danlos syndrome
In many cases, however, no clear cause or risk factor is identified.
Symptoms of Amniotic Band Syndrome
The symptoms of ABS depend on which body part is affected and how tightly the band constricts it. Mostly, the cases involve damage to the hands and feet, but the bands can also tighten around the head, neck, or abdomen. In mild cases, the newborn may present with superficial constriction rings or mild limb deformities. In severe cases, the bands may cut off blood circulation, leading to amputation, severe swelling, or even life-threatening complications.
Some other major symptoms of ABS can include:
- Clubfoot
- Missing fingers and toes
- Absent or shortened limbs
- Syndactyly (fusion or webbing between fingers or toes)
- Cleft lip
- Cleft palate[4]
- Choanal atresia (underdeveloped nasal passage)
- Bone deformities (scoliosis)
- Micropthalmia (underdeveloped eyes)
Diagnosis of Amniotic Band Syndrome
The diagnosis of ABS involves a combination of clinical, ultrasonographic, and sometimes advanced imaging techniques. These methods help in identifying the characteristic anomalies resulting from the constricting bands.
Clinical Features & Physical Examination:
This condition commonly affects the distal parts of the limbs, where soft tissue constriction or amputation may be visible. Upper limbs tend to be more frequently affected than lower limbs. Craniofacial abnormalities and trunk abnormalities can present severe forms of ABS.[5] Trunk abnormalities can include spinal deformities, abdominal wall defects, herniation of intestine, or organs.
Prenatal Diagnosis:
Early diagnosis typically relies on a detailed prenatal ultrasound examination. Direct visualization of the amniotic bands is difficult. Diagnosis often depends on indirect signs such as limb deformities, amputations, and distal edema observed on ultrasound. The healthcare providers use these methods to assess the condition further:
- Three-dimensional ultrasound and fetal magnetic resonance imaging (MRI) for detailed and accurate assessment of the extent and severity of band-related anomalies.
- Color Doppler ultrasound can aid in differentiating bands from lymphatic and vascular complications.
- Frequent ultrasound evaluations after every two to three weeks can also monitor evolving fetal well-being and fetal deformities.
Postnatal Examination:
Postnatally, the healthcare providers perform a detailed examination of the placenta in suspected ABS newborns with visible constrictions and other defects. The placenta may show areas where the amnion is absent, which can help confirm ABS, though such tests are not routinely performed.
Amniotic Band Syndrome Treatment
There are no established guidelines for managing ABS. Treatment varies for each patient, and the exact treatment depends on the location of the bands and how tightly they were wrapped. In mild cases, when shallow bands do not interfere significantly with the limb or digit function and do not involve the umbilical cord, no treatment is usually required. While in the case of prenatal diagnosis of deeper amniotic bands that affect the limb appearance or concern regarding the involvement of the umbilical cord, fetal surgery may be necessary.
Fetal Surgery for ABS:
The goal of the fetal surgery is to release the constrictions resulting from the amniotic bands before they can cause any further damage. Surgeons use fetoscopic techniques to visualize and cut the bands, restoring normal blood flow.[6]
The success of the fetal surgery lies in the degree of damage caused by amniotic bands. If the constriction is more severe, then the release of the band can stop further damage and prevent amputation of the affected extremity.
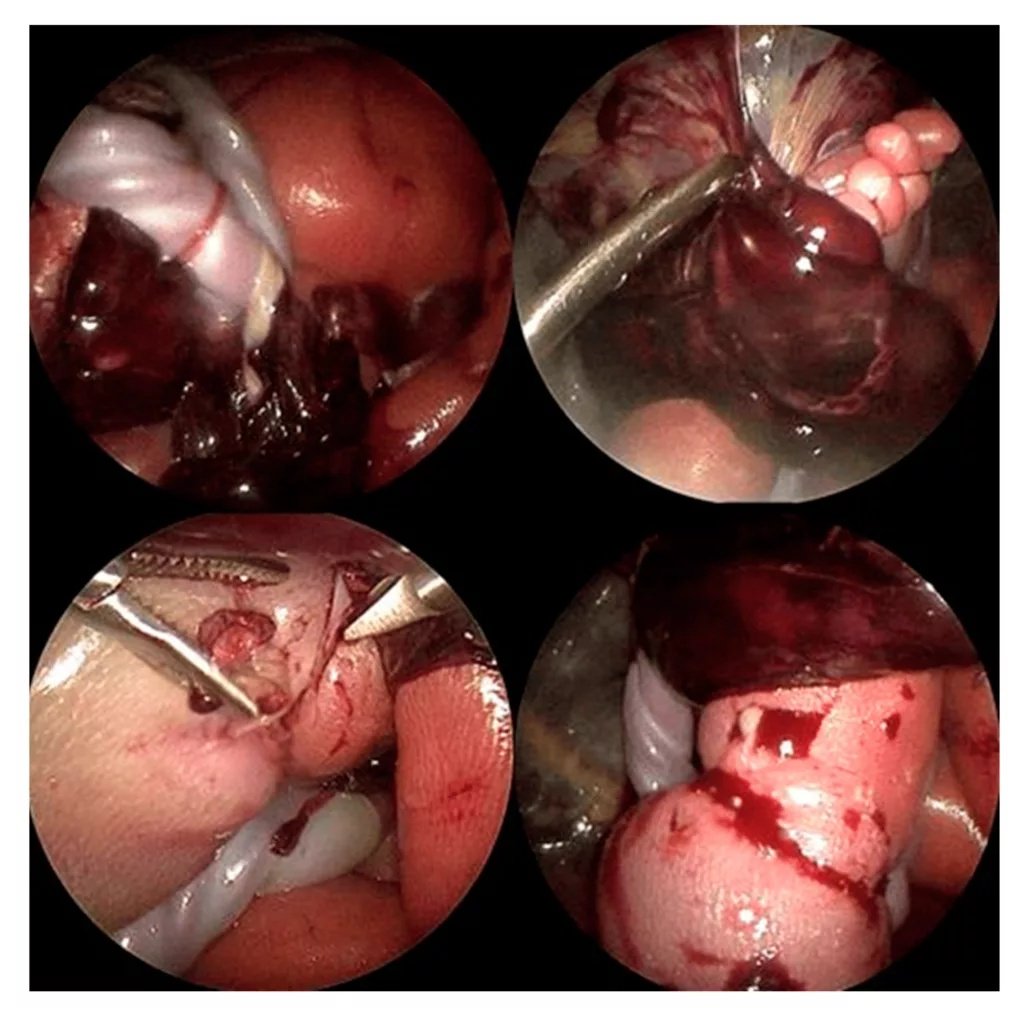
Top left: Multiple annular amniotic bands were entangling the umbilical cord and placental tissues.Top right: The fetal left foot was stuck within a part of the placenta, both restricting fetal movement and placing the mother and fetus at high risk of hemorrhage.Bottom left: A tight amniotic band encircling the right fetal calf caused severe strangulation, which would have led to partial limb autoamputation if left unresolved.Bottom right: After dissection of the right leg constriction due to the amniotic band, blood flow to the calf and foot improved immediately. Image Courtesy: Minimally Invasive Fetoscopic Resection of Life-Threatening Amniotic Band Constrictions in a Human Fetus at 22 + 2 Weeks of Gestation Complicated by Subtotal Chorioamniotic Separation and Partial Placental Abruption by Riehle et al. 2025, available viaMDPIunder license CC BY 4.0.
However, the risks associated with fetoscopic band release include:
- Pre-mature rupture of membranes
- Preterm delivery
- Fetal injury
- Infection
- Intrauterine bleeding
Postnatal Management & Treatment:
Postnatal management includes thorough physical examination and consultation with multidisciplinary teams if needed. Treatment after birth consists of:
Plastic & Reconstructive Surgery
Surgery can correct issues like club foot, cleft palate, or lip or webbing. Children with missing or shortened limbs may benefit from a prosthesis (artificial body parts). Advances in three-dimensional printing have led to the creation of more functional prostheses for such patients.
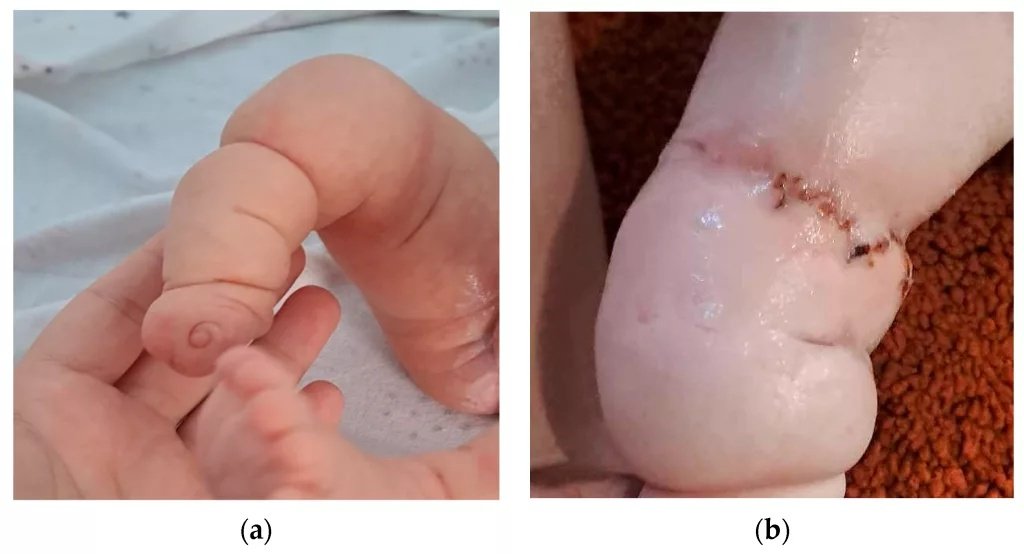
a) Postnatal aspect of the right lower limb. (b) Right lower limb after surgery.Image Courtesy: Amniotic Band Syndrome—Prenatal Diagnosis by Gica et al. 2024,doi.org/10.3390/diagnostics14010034, available via: https://www.mdpi.com/2075-4418/14/1/34, CC BY 4.0.
Physical & Occupational Therapy
After plastic or reconstructive surgery, physical and occupational therapies can help patients train them to use the prostheses and improve their overall function.[7]
Differential Diagnosis of ABS
Several congenital and structural conditions can mimic amniotic band syndrome (ABS), including anencephaly, cleft lip or palate, gastroschisis, omphalocele, and trisomy 18. However, the most important differential diagnoses to consider are:[8]
- Amniotic sheets: Benign intrauterine membranes that do not cause fetal entanglement or constriction.
- Transverse limb deficiency: Limb loss due to vascular disruption rather than amniotic entrapment.
- Body stalk anomaly: Characterized by a short or absent umbilical cord with severe body wall defects.
- Chorioamniotic separation: Detachment between the chorion and amnion that can appear similar on ultrasound.
- Skeletal dysplasia: Genetic bone disorders that cause limb shortening or deformities.
Prognosis of Amniotic Band Syndrome
The prognosis for infants with ABS depends on the extent and location of the deformities. While isolated limb constrictions usually have an excellent outcome, cases involving vital organs or the umbilical cord carry a poorer prognosis and may result in fetal loss. The healthcare providers should provide individualized counseling to parents. They should tailor the counselling according to the fetal and neonatal clinical presentation resulting from ABS. It can involve discussion of the termination of the pregnancy and neonatal palliative care.
Amniotic Band Syndrome Complications
Complications rely on the extent of the fetal anomalies. Obstetric complications are
- Low birth weight of the newborn
- Pre-mature membrane ruptures
- Stillbirths
- Preterm births[9]
Final Remarks
Females probably have a lot of questions and concerns when their baby is diagnosed with amniotic band syndrome. The healthcare team must support the lady with counselling. The exact situation will depend on the severity of the condition. The female might have to go through more ultrasounds during pregnancy. Management of the condition requires a collaborative, patient-centered approach. These involve physicians, advanced practitioners, social workers, nurses, and other healthcare professionals. The baby might need surgery at birth, rehabilitation, or a prosthesis to restore the function of their limbs in severe cases. Females must prepare their mind for consequences of ABS.
References
[1] Niu, Z., Meng, H., Zhang, X., Ouyang, Y., Zhang, Y., & Wu, X. (2019). Two case reports: early detection of amniotic band syndrome by adhesion between hand and umbilical cord at 11 to 14 weeks’ gestation.Medicine,98(50), e18302.
[2] Muhumad, S. H. H., Ali, A. O., Moumin, H. E., Egge, A. A. A., Nour, R. M., & Muhumed, M. A. (2025). Amniotic band syndrome: Insights from first documented case report in Somalia’s low-resource setting.International Journal of Surgery Case Reports,129, 111135.
[3] Inglesby, D. C., Janssen, P. L., Graziano, F. D., Gopman, J. M., Rutland, J. W., & Taub, P. J. (2023). Amniotic band syndrome: head-to-toe manifestations and clinical management guidelines.Plastic and Reconstructive Surgery,152(2), 338e-346e.
[4] Pape, K., & Gorla, S. R. (2025). Amniotic band syndrome. InStatPearls [Internet]. StatPearls Publishing.
[5] Iqbal, C. W., Derderian, S. C., Cheng, Y., Lee, H., & Hirose, S. (2015). Amniotic band syndrome: a single-institutional experience.Fetal Diagnosis and Therapy,37(1), 1-5.
[6] Minella, C., Costantino, B., Ruano, R., Koch, A., Weingertner, A. S., Favre, R., & Sananes, N. (2021). Fetoscopic release of amniotic band syndrome: an update.Journal of Ultrasound in Medicine,40(5), 1039-1048.
[7] Sarwark, J. F., & Carl, R. L. (2022). Amniotic Band Syndrome.Orthopaedics for the Newborn and Young Child: A Practical Clinical Guide, 183.
[8] Werakkody, Y., & Campos, A. (2024, August 22). Amniotic band syndrome.Radiopaedia. https://radiopaedia.org/articles/amniotic-band-syndrome?lang=us
[9] Iqbal, C. W., Derderian, S. C., Cheng, Y., Lee, H., & Hirose, S. (2015). Amniotic band syndrome: a single-institutional experience.Fetal Diagnosis and Therapy,37(1), 1-5.