
{kind=link}

lock jaw trismus Trismus, also known as lockjaw (lock jaw), is a painful condition characterized by restricted mouth opening. In this condition, the jaw muscles may become tight or go into spasm, and in some cases, joint restriction, fibrosis, or underlying disease processes may further limit movement. The most well-known cause of lockjaw is a life-threatening condition called Tetanus, caused by Clostridium tetani.
However, multiple factors can lead to long-term (chronic) tightening of the jaw muscles, including cancer (and cancer treatment), joint issues (TMJ disorder), infections, and trauma, etc. According to the latest studies, the prevalence of trismus in oral squamous cell carcinoma patients is around 28%, and it leads to a significant lowering of quality of life. Doctors manage the condition by providing symptomatic relief and addressing the underlying issue.
What Is Lock Jaw?: lock jaw trismus
A normal mouth opening ranges from 35 to 55 millimeters. For the layman, a rough estimate of normal opening is about the width of 2 or 3 fingers held together in the space. When this space becomes less due to muscle spasm, joint restriction, fibrosis, or space-occupying conditions, the condition is called lockjaw. Clinically, this condition is referred to as trismus, while the term “lockjaw” is commonly associated with Tetanus. Most of the time, this chronic condition is the outcome of some other problem and not the disorder itself. The inability to properly open your mouth lays the foundation for numerous secondary issues that need to be addressed.
Symptoms Of Lock Jaw
The condition can cause trouble in chewing and speaking. The most common symptoms associated with lockjaw include:
Jaw Tightness
Most patients feel symptoms like jaw tightness very frequently. Several individuals explain it as similar to a muscle cramp in the jaw. Many notice an increase in muscle tone that restricts jaw movement. Most of the time, it starts as an initial ache that progresses to muscle spasm and pain.
Jaw Pain And Restricted Movement
Pain associated with a locked jaw is not limited to movement (opening of the mouth). Numerous people across the globe say that they have to endure pain while opening the mouth and even when the mouth is stationary. The condition also reduces your ability to open your mouth wide. This may even interfere with the biting ability and may compromise proper brushing/flossing.
Causes Of Lock Jaw
A lot of health conditions can lay the foundation for a locked jaw. A locked jaw can present as a short-term (acute) or long-term disorder (chronic). Clinical data suggest that the following conditions are the most common culprits for jaw tightening:
Tetanus
It is a potentially life-threatening bacterial infection caused by the Clostridium tetani bacteria. These pathogens target the nervous system by releasing a toxin that induces severe muscle spasms in the head/neck region. The induction of jaw rigidity with the disease is so highly prevalent that the condition is also referred to as lockjaw. Reports show that trimus and swallowing difficulties (dysphagia) are early symptoms of the fatal bacterial infection.
Temporomandibular Joint (TMJ) disorder
The joint that connects your upper jaw to the lower jaw is called the temporomandibular joint. The junction is composed of numerous soft tissues, such as ligaments, tendons, and muscles, in addition to the hard bones. This particular joint allows you to open and close your mouth.
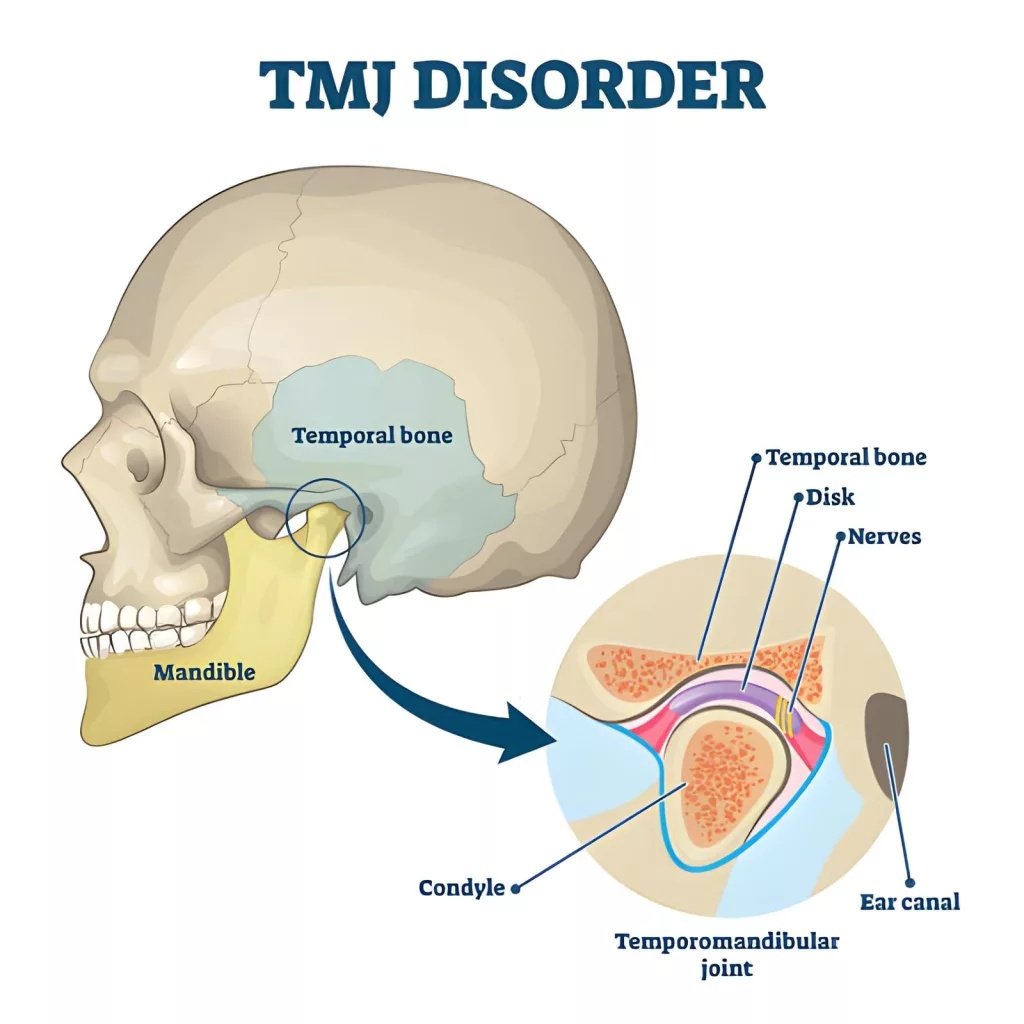
The TMJ is an important joint composed of different soft tissues. Disorder of the joint leads to tightening of the jaw.
Dysfunction or disorder of the joint potentially leads to a locked jaw. Many patients report limited mouth opening with periauricular pain (in the ear region). Jaw clicking can accompany pain in patients with TMD-induced trismus.
Infection
Dental infection is another problem that can lead to acute trismus. Tooth infections can cause maxillofacial abscesses (pus-filled cavities, usually attached to the tooth root). Very large abscesses can present with dysphagia and trismus.
Moreover, severe dental infections can extend beyond the tooth into neighboring head and neck spaces. This spread can hinder the normal opening of the jaw. Cervicalcellulitis (infection of deep tissues of the neck) and mediastinitis (infection of the middle chest cavity) are life-threatening complications arising from the space involvement of dental infections. Therefore, you must immediately visit a healthcare provider if experiencing jaw locking due to an underlying tooth infection.
Pericoronitis
The condition of infection and inflammation of the gum tissue covering a partially erupted tooth is called pericoronitis. This dental malady can directly contribute to jaw lock. In fact, trismus is a key feature of pericoronitis. When infection of the gum covering (operculum) progresses, it involves the surrounding soft tissues. This causes the jaw muscles to spasm and lock. Hence, cheek swelling (along the angle of the jaw) and trismus are evident symptoms.
Trauma
Injury and trauma to the head/neck region can induce limited mouth opening and jaw locking. We see lockjaw in cases ofmandibular (lower jaw) fractures. In rare instances, fractures of the upper jaw (zygomatic arch and zygomaticomaxillary complex) can impede the movement of the coronoid process (bony projection on the lower jaw). This eventually leads to trismus and locking of the jaw.
Dental Procedures
Getting a dental procedure can also trigger locking of the jaw. The chances of this happening are very less but still complications can arise from the simplest of procedures. The following steps/procedures can contribute to jaw locking:
Anesthesia Administration:
While giving local anesthesia for working on mandibular teeth, the dentist can mistakenly affect the masticatory muscles. In the administration of nerve block anesthesia to the inferior alveolar nerve, a doctor can penetrate the medial pterygoid muscle, which results in painful trismus. Such patients experience pain on opening the jaw due to stretching of the affected muscle. The pain stimulus immediately triggers a reflex contraction that limits mouth opening and results in jaw locking. Involuntary muscle spasms after an inferior nerve block can be managed with warm application, massaging, and TMJ exercises.
Another cause of trismus from local anesthetic is the formation of an intramuscular hematoma in the pterygomandibular space.
Dental Extraction:
Trismus, pain, and swelling are common complications of surgical extraction of lower wisdom teeth (mandibular third molars). These surgical complications are usually temporary and resolve without the need for intervention. However, in some cases, they may persist for longer periods (over 30 days). Symptoms of jaw tightening usually appear a couple of days after extraction. Doctors advise anti-inflammatory medications and incision and drainage therapy for severe cases.
Cancer
Oral cancers can restrict jaw movement due to tumor invasion, fibrosis, or pain-induced muscle guarding rather than direct muscle spasm. However, trismus can be a unique presentation of underlying malignancies. Due to the rarity, patients are often misdiagnosed. For example, a 62-year-old having severe trismus was diagnosed (and treated for) as TMD while she was suffering from adenocarcinoma of the temporal region. Cancer diagnosis was done a year later.
Therefore, experts advise general dentists to refer the patient to a specialist TMD clinic if the following features are present along with a lock jaw:
- No jaw clicking
- Mouth opening less than 15mm
- No neuralgia pain
- Lymphadenopathy (swelling of lymph nodes)
- Suspicious soft tissue lesions in the mouth
Cancer Treatment
Lockjaw is a common side effect of cancer therapy. Modalities like radiotherapy for head and neck cancer can induce fibrosis (excessive accumulation of fibrous tissue) of the masticatory muscles. The fibrosed muscles have a limited range of motion and less mobility. Reports suggest that radiotherapy-induced trismus is present in up to 40% of patients treated for head and neck cancer.
A clinical study found that the radiation dose and cancer location impact the extent of trismus in patients. Experts advocate early preventive physiotherapy programs in all such patients to prevent the development of trismus.
How Is Lockjaw Diagnosed?
Your healthcare provider will start by taking a history of your symptoms and any ailments in the recent past. He may ask you for details about TMJ clicking and cancer (or cancer therapy). This may be followed by a physical examination of the jaw and neck region to check for lumps and abscesses. Your dentist may also ask you to open and close your mouth as he listens to clicking from the TMJ. In addition to this, health professionals often use the following tests to reach a diagnosis:
Three-Finger Test
The clinician inserts three fingers (on top of each other) in the patient’s mouth to check the width of the opening. Generally, mouths open 40-60 millimeters. Doctors diagnose the condition as trismus if you are unable to open your mouth wider than 20-35 millimeters, or if the three fingers don’t fit.
Imaging Tests
Your doctor may order imaging tests to check damage to the temporomandibular joint and check for other causes. CT and MRI scans are modern imaging scans that provide detailed pictures of soft and hard tissues of the jaw.
How To Fix Lock Jaw?
Treatment is aimed at fixing the underlying cause of the lockjaw. Therefore, there are different strategies to treat trismus. The most commonly adopted locked jaw treatment modalities include:
Medications
Lockjaw is a painful condition; so, doctors usually advise medicines to treat the symptoms. Painkillers (analgesics) like non-steroidal anti-inflammatory drugs (ibuprofen, diclofenac, etc.) and muscle relaxants (diazepam, etc.) are usually prescribed in the acute phase of the disease. This modality works best for uncomplicated cases of transient lockjaw. However, you should be cautious with muscle relaxants because they directly impact your nervous system. Always take such medicines only according to a physician’s advice!
Heat Therapy
Therapists frequently use moist heat to ease muscular aches. Applying moist heat to the affected masticatory muscles can help improve symptoms. Most patients have noted improvements with the application of hot towels for 15-20 minutes.
Stretching And Exercise
In case of chronic disorders, doctors delay stretching exercises until the acute phase is over. After some alleviation of symptoms is achieved, healthcare providers guide the patients to do jaw stretches and exercises that reduce pain and improve jaw mobility.
It has proven to improve symptoms but not prevent trismus. Effective exercises in the matter include:
Passive Jaw Stretching:
This allows light stretching of your jaw muscles to relieve pain. To do this, you will need to place your thumb on the top teeth (in the middle of the jaw) while putting the index finger of your other hand on the bottom teeth (in the middle of the jaw). With moderate force from your fingers, open your mouth as wide as possible. Hold the stretch for 10 seconds. Repeat the stretch five times a day.
Note: Stop stretching and consult a doctor if you notice any pain!
Active Jaw Stretching:
For active stretching, you need to hold your head still (in a fixed position) and open your mouth wide (till it is comfortable) and hold this position for about 10 seconds. Then move your lower jaw (mandible) to the left and hold it there for 3 seconds. Then move it to the right and hold for 3 seconds. After this, move the lower jaw in a circle. Do 5 repetitions of the stretch in a day.
Note: You can only do this stretch if the process isn’t painful!
Chin Tucks:
Another exercise that strengthens your muscles and improves symptoms of lock jaw is chin tucks. You need to pull your chin close (or into) your chest while looking forward. Pull your head back (in a resting position). Hold the stretch for three seconds and repeat five times a day.
Physical Therapy
Physical therapists play a significant role in relaxing your taut muscles. Head and neck cancer patients are at a greater risk of developing lockjaw. Therefore, trials of physiotherapy have been performed on cancer patients with trismus. One study concluded that manual therapy for radiation-associated trismus significantly improved symptoms.

Such patients may also be treated with non-invasive therapies like low-intensity ultrasound therapy and therapist-guided exercise therapy. Studies show that the combination of exercise and ultrasound yields the best outcomes.
Dental Applicance
Another non-conservative method of dealing with this infirmity is by giving patients occlusal splints. It is a custom-made device made out of acrylic to treat trismus. The device is worn over the teeth to improve mouth opening and relieve muscle tension. Occlusal splints improve mouth opening and TMJ disorder, and thus aid in treating lockjaw.

Occlusal splints are effective in correcting lockjaw caused by TMJ disorder
Surgery
Surgical intervention is reserved for severe cases where the fibrosis in the masticatory muscles can not be corrected with conservative management. Surgeons remove the scar tissue in the jaw and reconstruct the tissues.
Complications Of Lock Jaw
Due to difficulty in opening the mouth, you can fall prey to complications like:
- Cavities (and infections) due to improper cleaning/brushing.
- Weight loss due to trouble eating.
- Aspiration of food into the airway due to the narrow passage of food.
Wrapping Up
Lock jaw is a painful condition of the jaw caused by spasm of the masticatory muscles. Patients experience jaw tightness and difficulty in moving the lower jaw. It commonly arises in tetanus (serious bacterial infection), head/neck cancer, and TMJ disorder. However, the disorder may develop transiently as a complication of dental infection (including pericoronitis), mistaken local anesthesia administration into the pterygoid muscle, or after third molar extraction. Mandibular fractures can also present with trismus.
Doctors diagnose the condition with physical examination, the three-finger test, and imaging scans (CT and MRI scans). Therapies are aimed at fixing the underlying causes leading to jaw locking. Painkiller medicines, physical therapy, and heat therapy are effective modalities. Stretching exercises help the patient in the long term but should only be done if not cause pain. Occlusal splints improve mouth opening and thus are beneficial. Surgical removal of scar tissue from masticatory (biting) muscles is reserved for severe cases.
References
[1] Mohanty, A., Dash, M., Chaturvedi, M., Dixit, H., Voulligonda, D., & Mathur, S. (2025). Prevalence of Trismus and its Effects on Quality of Life in Patients Treated for Oral Squamous Cell Carcinoma: A Prospective Study.Journal of Pharmacy and Bioallied Sciences,17(Suppl 5), S3491-S3493.
[2] Jang, S. H., Byun, J. S., Jung, J. K., & Choi, J. K. (2020). Case report of tetanus patient showing trismus and dysphagia as early symptoms.Journal of Oral Medicine and Pain,45(3), 79-82.
[3] Djody, A. F. S., Firdaus, M. Z., Alifta, V., Putri, I. I. U., Adysti, D. B., & Adji, I. S. (2024). Maxillofacial Abscess et Causa Odontogenic Infection: A Case Report.Sch J Med Case Rep,5, 577-586.
[4] Gaddipati, R. (2021). Fascial space infections. InOral and maxillofacial surgery for the clinician(pp. 441-459). Singapore: Springer Nature Singapore.
[5] Al Farabi Clinics, J., & Arabia, S. (2022). Etiology, Evaluation, and Treatment of Pericoronitis.
[6] Khalifeh, B., Simonian, K., Houmani, M., El-Outa, A., Khalil, W., & Houmani, M. (2024). Trismus following inferior alveolar nerve block: a case report.Cureus,16(11).
[7] Zhang, Y., Zhuang, P., Jia, B. O., Xu, J., Cui, Q., Nie, L., … & Zhang, Z. (2021). Persistent trismus following mandibular third molar extraction and its management: A case report and literature review.World Academy of Sciences Journal,3(1), 2.
[8] Honda, K., Natsumi, Y., Sakurai, K., Ishikura, R., & Urade, M. (2006). Mucinous adenocarcinoma of the temporal region initially diagnosed as temporomandibular disorders: a case report.Journal of oral pathology & medicine,35(9), 582-585.
[9] Aghajanzadeh, S., Karlsson, T., Tuomi, L., Engström, M., & Finizia, C. (2023). Trismus, health-related quality of life, and trismus-related symptoms up to 5 years post-radiotherapy for head and neck cancer treated between 2007 and 2012.Supportive Care in Cancer,31(3), 166.
[10] Faravel, K., Jarlier, M., Senesse, P., Huteau, M. E., Janiszewski, C., Stoebner, A., & Boisselier, P. (2023). Trismus occurrence and link with radiotherapy doses in head and neck cancer patients treated with chemoradiotherapy.Integrative Cancer Therapies,22, 15347354221147283.
[11] Scherpenhuizen, A., van Waes, A. M., Janssen, L. M., Van Cann, E. M., & Stegeman, I. (2015). The effect of exercise therapy in head and neck cancer patients in the treatment of radiotherapy-induced trismus: a systematic review.Oral oncology,51(8), 745-750.
[12] Shao, C. H., Chiang, C. C., & Huang, T. W. (2020). Exercise therapy for cancer treatment-induced trismus in patients with head and neck cancer: A systematic review and meta-analysis of randomized controlled trials.Radiotherapy and Oncology,151, 249-255.
[13] McMillan, H., Barbon, C. E., Cardoso, R., Sedory, A., Buoy, S., Porsche, C., … & Hutcheson, K. A. (2022). Manual therapy for patients with radiation-associated trismus after head and neck cancer.JAMA Otolaryngology–Head & Neck Surgery,148(5), 418-425.
[14] Elgohary, H. M., Eladl, H. M., Soliman, A. H., & Soliman, E. S. (2018). Effects of ultrasound, laser and exercises on temporomandibular joint pain and trismus following head and neck cancer.Annals of rehabilitation medicine,42(6), 846-853.
[15] Albagieh, H., Alomran, I., Binakresh, A., Alhatarisha, N., Almeteb, M., Khalaf, Y., … & Alqahatany, M. (2023). Occlusal splints-types and effectiveness in temporomandibular disorder management.The Saudi dental journal,35(1), 70-79.