
, also known as desmoid-type fibromatosis or aggressive fibromatosis, is a rare tumor of the...){kind=link}

Desmoid Tumor Diagnosis Desmoid Tumor (DT), also known as desmoid-type fibromatosis or aggressive fibromatosis, is a rare tumor of the connective tissues. Unlike cancers, desmoid tumors do not spread (metastasize) to other parts of the body. However, they can behave aggressively where they start, growing into nearby tissues and sometimes causing serious problems depending on their size and location. The incidence of this particular tumor lies between 2 and 4 patients per million individuals. This benign tumor primarily affects the soft tissues (connective tissues) of the limbs (arms and legs) and abdomen, but can also be found in other areas. These tumors account for approximately 3% of all soft tissue tumors and contribute to 0.03% of all neoplasms. The average age of diagnosis is between 20 and 40 years.
Desmoid tumors generally grow slowly but can grow quickly and affect nearby organs. Conventionally, oncologists have managed tumors with surgical removal, but now advanced targeted therapies are showing promising results. They can be treated without much difficulty, but there is a high chance of recurrence.
Desmoid Tumor Types
Abdominal Wall Desmoid Tumors:
These aggressive tumors of the connective tissues most frequently arise in the abdomen, involving the abdominal walls. In a clinical study, researchers found that desmoid tumors of the anterolateral abdominal wall are locally aggressive and infiltrating, and tend to affect vital organs. Several female patients present with a lower abdominal wall tumor after cesarean section. They may develop or enlarge during pregnancy, thus becoming noticeable.
Intra-Abdominal Tumors:
This type arises in the mesentery, which is a structure that connects the posterior wall of the abdomen to the intestine. These tumors can rapidly grow to large sizes (locally) and have a high rate of recurrence after treatment.
Extra-Abdominal Desmoid Tumors:
As the name indicates, these types of tumors are present in areas other than the abdomen.
Arms
Upper extremity desmoid tumors are relatively common. The most common location in the region is the shoulder, where you can find 52% of tumors. This is followed by the upper arm, which contributes to 31% of desmoid-type fibromatosis growths.
Legs
Tumors may also develop in the lower extremities. The rare neoplasms are predominantly found in women aged 15 to 60. Occurrence in the leg is low, but they may develop in the thighs and the leg. Large intramuscular tumors of the leg can imitate external popliteal sciatic neuropathy by impinging on neighboring structures.
Doctors have found extra-abdominal desmoid tumors in:
- Neck
- Chest
- Buttocks
- Back
Desmoid Tumor Symptoms
There are no tumor symptoms in numerous cases. Patients start feeling symptoms only when the tumor becomes large enough to press on nearby organs. In most cases, symptoms of nerve impingement are experienced by people. When present, patients report the following symptoms:
Lump/Soft Tissue Mass:
Several patients report to the ER with the complaint of a growing lump. A 45-year-old female presented with a gradually progressive lump that had been growing for 6 months. She reported having pain along with overgrowth. CT and MRI scans revealed abdominal wall desmoid tumors. A giant desmoid tumor of the anterior abdominal wall may also be felt as a lump in the belly.
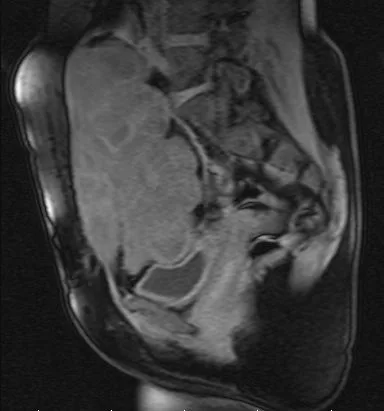
MRI scan of a patient shows a desmoid tumor. Image courtesy of By Historik – Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=2778067
Note: In general, any lumps greater than 2 inches (in any part of the body) must be evaluated by a doctor!
Very large and aggressive soft tissue masses, like abdominal desmoid tumors, can even impact the quality of life in patients.
Nerve Symptoms:
The fibromatous growths can become very large and put pressure on the nerve structures. They may involve neurovascular bundles leading to typical nerve symptoms. This occurs mostly in extra-abdominal cancers involving the extremities. Patients with nerve involvement report symptoms like pain, burning, tingling, and loss of function. Sufferers may also encounter paraesthesias/anesthesias (altered sensations). Functional disability, especially of the lower limbs, can be attributed to nerve damage caused by the cancer.
Nausea & Vomiting:
The vast majority of cancer patients experience nausea and vomiting due to the underlying abnormal growths. Thus, desmoid tumor patients may also experience episodes of nausea and associated vomiting due to the disease.
Desmoid Tumor Causes
The soft tissue tumor is a myofibroblastic neoplasm, meaning it originates from myofibroblasts, connective tissue cells that normally help repair wounds. It develops when there is a mutation in the connective tissue cells, which leads to uncontrolled division.
Genetic Mutation:
Experts are unaware of the exact cause of desmoid tumors. However, many believe that dysregulation of the Wnt pathway plays an important role in leading to tumor development. This pathway regulates processes like cell differentiation and proliferation. When this group of signal transduction pathways is blocked, there is a shift from the normal homeostatic and developmental processes.
The Wnt pathway dysregulation is attributed to a mutation in the β-catenin gene (CTNNB1 gene) or a germline mutation in the adenomatous polyposis coli (APC) gene. It is seen in 85% of cases. With this mutation, there is an accumulation of the β-catenin protein, which gets translocated to the nucleus (nuclear β-catenin expression). Research shows that the CTNNB1 gene mutation is directly linked to desmoid tumor formation, which can be easily detected due to the expression of nuclear β-catenin
Further subclassification of the CTNNB1 gene mutation reveals that T41A and T41I mutations are more common in men, while S45F and S45P mutations are frequently associated with abdominal wall tumors. Moreover, different proteins such as the cyclo-oxygenase 1 (COX-1) and vascular endothelial growth factor can contribute to the growth of the tumor. Desmoid tumors may even develop sporadically without any underlying gene mutations.
Risk Factors:
Certain conditions increase your chances of falling prey to soft tissue tumors. The risk factors for desmoid tumors include:
Young age
Most patients with DT are diagnosed at an early age, i.e., between 30 and 40 years.
Female
Being a woman predisposes you to these tumors (more than men). As mentioned, numerous women get the diagnosis after pregnancy and/or childbirth. Pregnancy-associated desmoid tumors contribute to 8-18% of all reported desmoid tumors. Some believe that the high estrogen levels during pregnancy may also be linked to DTs.
Familial Adenomatous Polyposis (FAP)
FAP is a genetic disorder characterized by the development of multiple polyps in the large intestine. Patients suffering from FAP tend to develop desmoid tumors due to gene mutations. Reports show that DTs are found in around 10-25% of familial adenomatous polyposis patients.
Studies have identified FAP-induced DTs in different regions of the body, including:
- Mesenteric or retroperitoneal region (58%)
- Abdominal wall (25%)
- Extremities (6%)
- Breast (6%)
- Back (4.5%)
These tumorous growths were easy to manage, and only about 27% patients experienced significant morbidity.
Due to the high prevalence of intra-abdominal desmoid tumors and colorectal cancers in FAP patients, doctors sometimes opt for prophylactic surgery.
Trauma/Injury Or Surgery
It is believed that trauma can induce the development of desmoid tumors. Blunt trauma, fracture, implant placement, and surgery can prove to be triggers for the disorder. According to a study, a significant group of patients suffer from trauma-associated desmoid tumors. The most common occurrences are seen in prior surgical sites for breast or groin implants. This may be a reason why some women develop desmoid tumors post-casarean surgery. There have also been cases where pregnant ladies have noted aggressive growth and proliferation of the tumor during pregnancy.
Desmoid Tumor Diagnosis
In many cases, desmoid tumors go undiagnosed for a long period because of a lack of symptoms. Most patients visit a healthcare facility only when they have issues, such as lumps. At the facility, healthcare providers begin by taking a history of the disease, followed by a physical examination of the lumps/growths.
Imaging Tests:
To visualize and analyze the growth, your doctor may order different imaging tests for diagnosis. Radiologists prefer using multimodality imaging techniques to better analyze DTs. The most prevalent imaging strategies include ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) scans. These techniques not only help diagnose the benign tumor but also aid doctors in performing minimally invasive treatments.
Computed Tomography (CT scans)
Health professionals are capable of diagnosing soft tissue pathologies with the help of CT scans. According to a case report, doctors diagnosed a patient’s abdominal wall desmoid tumor using a CT scan.
Magnetic Resonance Imaging (MRI) scans
MRIs provide a great amount of detail regarding soft tissues. Therefore, they are preferred for most anatomic locations of DT. Oncologists frequently advise MRI scans for desmoid tumor patients. It helps in analyzing the size of the tumor and devising a treatment plan accordingly.
Biopsy:
Sometimes, doctors go for a tumor biopsy to know more about the growth. Mostly, a biopsy is done using a fine needle that withdraws a small sample of the tumor. The sample is then sent to a lab where pathologists examine it under a microscope.
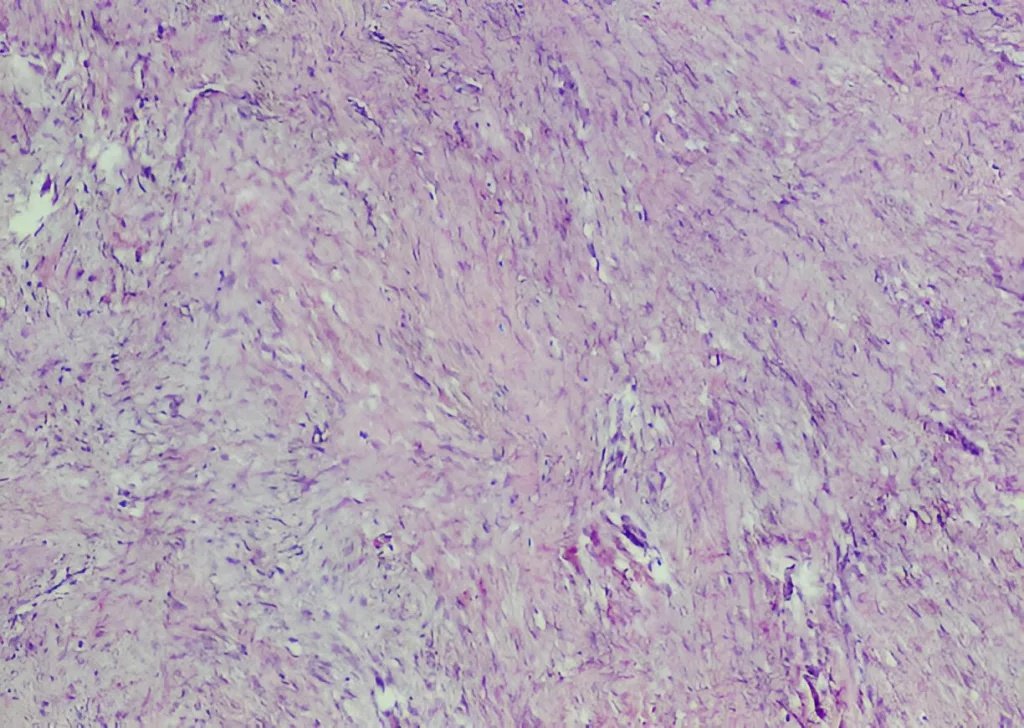
The picture shows microscopic analysis (histopathology) of a desmoid tumor.
Other tests for diagnosis include:
- Colonoscopy
- Immunostaining
- Next-generation sequencing
- Genetic testing
Differential Diagnosis:
Multiple conditions fall under the differential diagnosis for desmoid tumors.
Desmoid Tumor Vs Sarcoma
Fibrosarcoma:
Like a desmoid tumor, a fibrosarcoma arises from the fibrous (soft tissues) of the body and can occur in various locations, like the lower extremities. However, unlike benign desmoid tumors, fibrosarcomas are malignant cancers that can metastasize to different healthy organs.
Fibromyxoid Sarcoma:
Another type of malignant soft tissue cancer is the fibromyxoid sarcoma, which has presentations similar to a desmoid tumor. Differentiation between the pathologies is done using a microscopic (histological) analysis. A study concluded that in 29% (94/320 surgical specimens) of cases, a soft tissue lesion was wrongly classified as a desmoid tumor. The actual diagnoses in these cases were low-grade fibromyxoid sarcoma, myofibroma, and collagenous fibroma, etc.
Desmoid Tumor Vs Gastrointestinal Stromal Tumors (GIST):
The locally aggressive desmoid tumors can resemble another pathology, i.e., the gastrointestinal stromal tumor. Both are mesenchymal tumors of the mesenchyme that mostly develop in the GI tract. However, desmoid tumors arise from the myofibroblast cells, and GISTs arise from the specialized interstitial cells of Cajal in the GI tract. While desmoid tumors never metastasize, GISTs can spread to different organs. GIST formation is attributed to mutations in the KIT or PDGFRA gene. On the other hand, desmoid tumors form due to abruption of the Wnt pathway.
Desmoid Tumor Treatment
In several cases, the desmoid tumors disappear without any treatment. Therefore, doctors prioritize observing (monitoring) the tumor over intervention. Only symptomatic cases or cases with complications require treatment. The different treatment strategies adopted depend on factors like the size, growth rate, and location of the tumor.
Monitoring (Active Surveillance):
In cases of asymptomatic, slow-growing tumors, doctors do not perform any procedures. Usually, such growths are diagnosed during routine check-ups, and doctors place the patient under active surveillance instead of recommending medications or surgery. As this tumor is benign, treatment is only needed when symptoms appear. Your doctor will advise you to have routine imaging tests to observe the growth of the desmoid tumor.
Studies show that it is a feasible option for desmoid tumors because around 80% of tumors undergo spontaneous regression during active surveillance.
When symptoms are present, Doctors can adopt a variety of strategies to manage a desmoid tumor. Conventionally, oncologists relied on surgical excision of the tumor only, but fortunately, now multiple modalities can save you from going under the knife and kill the tumor.
Chemotherapy:
Low-dose chemotherapeutic drugs in combination with methotrexate can be effective, but have significant toxic effects. The current standard of care for DTs includes low-dose vinblastine and methotrexate for prolonged periods.
Targeted Therapy:
It is an advanced type of therapy for cancer patients that serves as a feasible alternative to conventional chemotherapy. Unlike chemotherapy, drugs used in targeted therapy have an impact only on the tumors/cancers and spare healthy cells. Drugs like tyrosine kinase inhibitors (TKIs) are showing remarkable effects in desmoid tumors.
Sorafenib & Pazopanib
New generation TKIs like sorafenib and pazopanib are commonly used drugs for this purpose. These drugs have shown noticeable regression in tumor size. Oncologists carefully determine the optimal duration of treatment. However, side effects can make patients discontinue therapy.
Gamm-Secretase & Anthracycline
Anthracycline-based therapy may also be adopted. When compared to sorafenib, anthracycline-containing drugs showed better 1-year response rates, but were also linked to a higher incidence of serious side effects.
Gamma-secretase inhibitors (nirogacestat) demonstrate good responses but are associated with severe toxic effects, which is why doctors mostly stick to TKIs. c
Your doctor may advise a beta-catenin inhibitor like Tegavivint. It is a selective inhibitor of nuclear β-catenin. Its use leads to a reduction in the nuclear β-catenin. Therefore, this drug proves to be a novel therapeutic strategy for desmoid tumor treatment.
Cryoablation:
Cryo- means cold, and ablation means destruction of the tissues. Cryoablation is a therapeutic procedure that uses extreme cold to destroy cancerous cells. Doctors perform cryoablation with a fine needle-like instrument called the cryprobe. Percutaneous cryoablation has proven to be a safe and effective modality for extra-abdominal desmoid tumors.
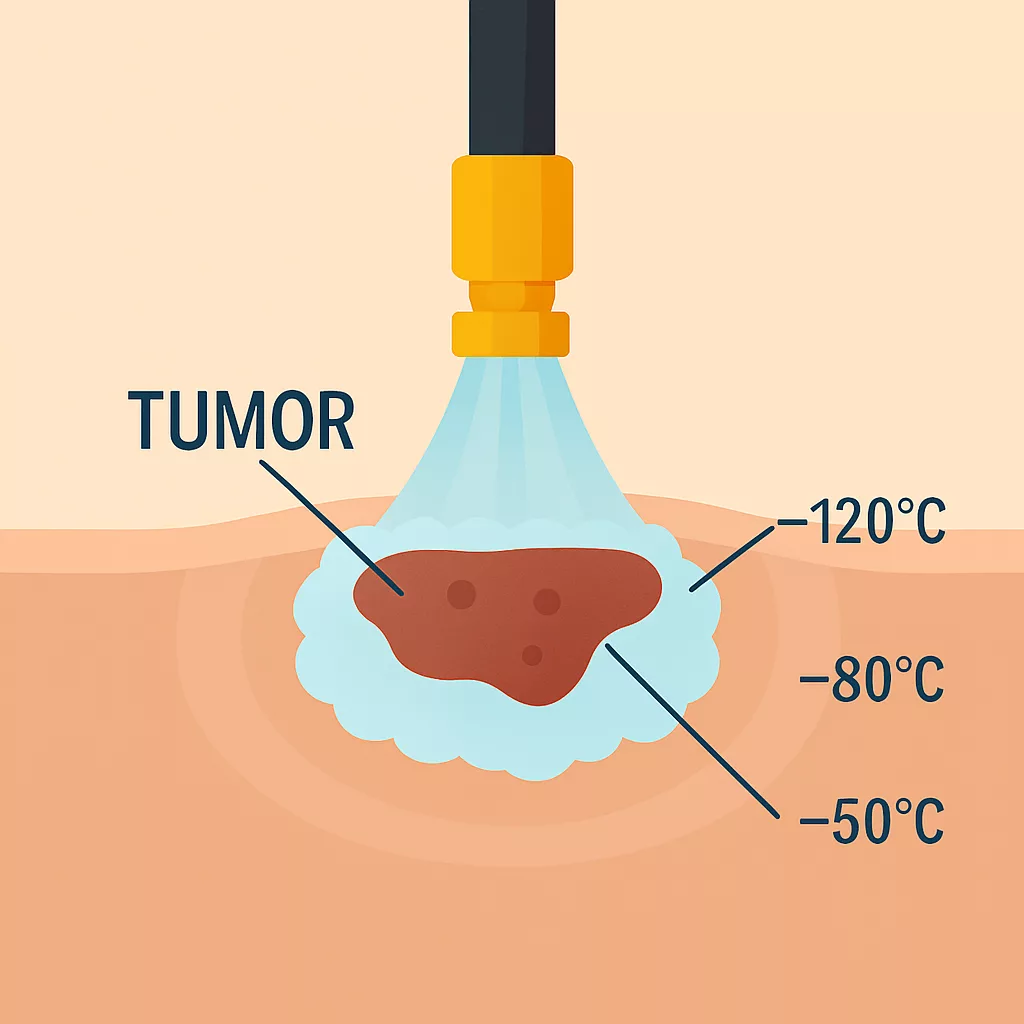
The process of cryoablation freezes the tumor to shrink it in size.
Moreover, it is safe, convenient, and effective in the management of pediatric patients with DTs. This type of treatment not only removes tumors but has also shown superb results in managing them. A clinical study concluded that cryoablation is effective in the analgesic management of inoperable desmoid tumors. Thus, patients can notice evident reductions in tumor-induced pain even when surgical excision is risky or not possible.
Hormone Therapy:
Systemic therapy with hormones is known to halt the progression of the tumor. Doctors often advise tamoxifen with a non-steroidal anti-inflammatory drug like sulindac to treat desmoid tumors. Evidence suggests that the combination of tamoxifen and sulindac plays a positive role in DT management.
Radiotherapy:
Radiation therapy is not used as frequently as other modalities. In most cases, it is used in conjunction with other strategies to shrink or eliminate the tumor.
Surgery:
For fast-growing, symptomatic tumors, doctors prefer surgical removal. Most surgeons prefer surgical intervention when the patient is experiencing severe symptoms or serious complications like intestinal obstruction.
Desmoid Tumor Prognosis:
The 5-year recurrence-free survival rate for desmoid tumor patients is:
- 23% for patients with the 45F mutation
- 577% for patients with the 41A mutation
- 65% with no mutations
Final Word
Desmoid tumors are rare and benign soft tissue tumors that can grow to large sizes. They mainly develop on the abdominal wall but can also arise in the extra-abdominal locations like arms, legs, and back, etc. In most cases, fibromatous growths are asymptomatic, but large tumors can cause symptoms like a lump/mass in the abdomen, nausea/vomiting, and nerve symptoms (pain, burning, tingling) due to nearby nerve impingement.
These aggressive fibromatous growths develop as a result of the Wnt pathway dysregulation, which leads to the buildup of nuclear beta-catenin proteins. In several cases, the protein accumulation is attributed to the CTNNB1 gene mutation. Women of childbearing age and patients with familial adenomatous polyposis are at greatest risk. Many tumors disappear without treatment, and several do not have any symptoms. Doctors treat only when the cancer is symptomatic or causing complications.
Modern-day treatment involves chemotherapy and targeted therapy with drugs like tyrosine kinase inhibitors (sorafenib and pazopanib), anthracycline-based drugs, beta-catenin inhibitors, and gamma-secretase inhibitors, etc. Other strategies to shrink and eliminate desmoid tumors include cryoablation, hormone therapy, and radiotherapy. Conventionally, surgery was the mainstay of the treatment. However, now surgery is reserved only for cases with severe symptoms or serious complications.
References
[1] Master, S. R., Mangla, A., & Shah, C. (2024). Desmoid tumor. InStatPearls [Internet]. StatPearls Publishing.
[2] Arzoo, S., Akter, M. S., Afroz, S., Rahman, M. A., & Akther, M. (2022). Desmoid Tumor of the Abdominal Wall: A Case Report.Eastern Medical College Journal,7(2), 28-31.
[3] Mabrouk, M. Y., Bouzayan, L., Malki, S., Jabi, R., Bennani, A., & Bouziane, M. (2021). Desmoid tumor of the anterolateral abdominal wall: a rare case report.Annals of Medicine and Surgery,70, 102804.
[4] Fujita, M., Yamamoto, M., Kaizaki, Y., Kato, M., & Tsuchida, T. (2022). Treatment of a desmoid tumor that enlarged during pregnancy: a case report and literature review.The Kurume Medical Journal,69(1.2), 99-102.
[5] Kim, S. J., Han, J. W., Yoon, T., Choi, H., & Han, Y. D. (2023). A giant, rapidly growing intra‑abdominal desmoid tumor of mesenteric origin in an adolescent male: A case report and literature review.Experimental and Therapeutic Medicine,26(4), 490.
[6] Boushabi, A., Ait Benali, H., & Shimi, M. (2024). Intramuscular desmoid tumor of the leg leading to external popliteal sciatic neuropathy: A case study and literature review.International Journal of Surgery Case Reports,116, 109333.
[7] Varma, A., Dhande, R. P., & Pattabiraman, S. (2021). Abdominal Wall Desmoid Tumor Diagnosis On Computed Tomography Scan.Journal of Datta Meghe Institute of Medical Sciences University,16(2), 382-383.
[8] Nandu, V., Ghag, G., Sanjanwala, S., Parmeshwar, T., & Gadapaga, V. (2022). Large Recurrent Desmoid Tumour over Anterior Abdominal Wall: A Case Report.Asian Journal of Case Reports in Surgery,15(1).
[9] Ghaddou, Y., Bouziane, M., Nouri, A., Sair, K., & Fadil, A. (2024). Management of a large abdominal desmoid tumor complicated by lymphedema of the lower limb: a case report.Cureus,16(7).
[10] Yin, J. Q., Fu, Y. W., Gao, Z. H., Zou, C. Y., Xie, X. B., Wang, B., … & Shen, J. N. (2021). A novel method to treat progressive desmoid tumors involving neurovascular bundles: a retrospective cohort study.Neurosurgery,88(6), 1095-1102.
[11] An, J., Woo, H. Y., Lee, Y., Kim, H. S., Jeong, J., & Kim, S. K. (2021). Clinicopathological features of 70 desmoid-type fibromatoses confirmed by β-catenin immunohistochemical staining and CTNNB1 mutation analysis.PLoS One,16(4), e0250619.
[12] Robinson, W. A., McMillan, C., Kendall, A., & Pearlman, N. (2012). Desmoid tumors in pregnant and postpartum women.Cancers,4(1), 184-192.
[13] Kumamoto, K., Ishida, H., & Tomita, N. (2023). Recent advances and current management for desmoid tumor associated with familial adenomatous polyposis.Journal of the Anus, Rectum and Colon,7(2), 38-51.
[14] Al-Sukhni, E., Shapiro, J., Suraweera, H., Semotiuk, K., Swallow, C. J., Brar, S., … & Gladdy, R. A. (2023). Desmoid tumors in familial adenomatous polyposis patients: favorable outcomes with multidisciplinary management.Annals of Surgical Oncology,30(8), 5142-5149.
[15] Campos, F. G., Martinez, C. A. R., Bustamante-Lopez, L. A., Mendonça, R. L. D. S., & Kanno, D. T. (2023). Intra-abdominal desmoid tumors in familial adenomatous polyposis: How much do clinical and surgical variables interfere with their development?.Clinics,78, 100144.
[16] Hohenberger, P., Menge, F., Hohenberger, R., Kasper, B., Marx, A., Haller, F., … & Jakob, J. (2024). Trauma and sporadic desmoid tumor development: an approach toward real incidence and aspects of causality.Cancer,130(1), 51-59.
[17] Varma, A. D., Dhande, R. P., & Pattabiraman, S. (2021). Abdominal Wall Desmoid Tumour Diagnosis on CT Scan–A Case Report.Journal of Evolution of Medical and Dental Sciences,10(3), 153-156.
[18] Riedel, R. F., & Agulnik, M. (2022). Evolving strategies for management of desmoid tumor.Cancer,128(16), 3027-3040.
[19] Goldstein, J. A., & Cates, J. M. (2015). Differential diagnostic considerations of desmoid-type fibromatosis.Advances in anatomic pathology,22(4), 260-266.
[20] Tsukamoto, S., Takahama, T., Mavrogenis, A. F., Tanaka, Y., Tanaka, Y., & Errani, C. (2023). Clinical outcomes of medical treatments for progressive desmoid tumors following active surveillance: a systematic review.Musculoskeletal surgery,107(1), 7-18.
[21] Sparber-Sauer, M., Orbach, D., Navid, F., Hettmer, S., Skapek, S., Corradini, N., … & Ferrari, A. (2021). Rationale for the use of tyrosine kinase inhibitors in the treatment of paediatric desmoid-type fibromatosis.British journal of cancer,124(10), 1637-1646.
[22] Noujaim, J., Gupta, A. A., Holloway, C. L., Saleh, R., Srikanthan, A., Lemieux, C., … & Costa, P. (2024). Real-word experience of pazopanib and sorafenib in patients with desmoid tumors: A CanSaRCC multi-center study.European Journal of Cancer,205, 114119.
[23] Costa, P. A., Arora, A., Fernandez, Y., Yi, I., Bakkila, B., Tan, H., … & Trent, J. (2025). Sorafenib or anthracycline‐based chemotherapy for progressive desmoid tumors.Cancer,131(1), e35647.
[24] Ou, J., Su, D., Guan, Y., Ge, L., Deng, S., Yan, Y., … & Xie, R. (2024). Efficacy and safety of systemic treatment for progressive and refractory desmoid tumor: a systematic review and Bayesian network meta-analysis.Discover Oncology,15(1), 619.
[25] Braggio, D. A., Costas C. de Faria, F., Koller, D., Jin, F., Zewdu, A., Lopez, G., … & Pollock, R. E. (2022). Preclinical efficacy of the Wnt/β-catenin pathway inhibitor BC2059 for the treatment of desmoid tumors.PLoS One,17(10), e0276047.
[26] Saltiel, S., Bize, P. E., Goetti, P., Gallusser, N., Cherix, S., Denys, A., … & Tsoumakidou, G. (2020). Cryoablation of extra-abdominal desmoid tumors: a single-center experience with literature review.Diagnostics,10(8), 556.
[27] Shaikh, R., Shashi, K. K., & Shahin, M. M. (2024). Cryoablation in extra-abdominal desmoid tumors: a 10-year experience in pediatric and young adult patients.CardioVascular and Interventional Radiology,47(12), 1776-1783.
[28] Bouhamama, A., Lame, F., Mastier, C., Cuinet, M., Thibaut, A., Beji, H., … & Pilleul, F. (2020). Local control and analgesic efficacy of percutaneous cryoablation for desmoid tumors.CardioVascular and Interventional Radiology,43(1), 110-119.
[29] Choudhury, H., & Abidoye, O. (2023). A Desmoid Tumor Responding to Systemic Therapy With Tamoxifen and Sulindac.Cureus,15(3).
[30] Master, S. R., Mangla, A., & Shah, C. (2024). Desmoid tumor. InStatPearls [Internet]. StatPearls Publishing.