
{kind=link}

Echinococcosis Echinococcus Eggs Echinococcosis, or hydatid disease, is a zoonotic parasitic infection caused by tapeworms of the genus Echinococcus. The illness places a significant burden on public health, particularly in areas of livestock production and proximity to dogs. Despite being a neglected tropical disease by the World Health Organization (WHO), echinococcosis affects millions of people worldwide.[1]
The disease is a result of the accidental ingestion of the tapeworm eggs that some animals (mainly dogs and wild canids) excrete into their feces. Once these eggs enter the human body, they form cysts that grow slowly over several years, and symptoms usually appear only when the enlarging cysts begin to interfere with organ function.
Causative Agent of Echinococcosis: Echinococcosis Echinococcus Eggs
The larval tapeworms of the genus Echinococcus cause the disease. The disease is categorized as cystic echinococcosis (CE) and alveolar echinococcosis (AE), with each species having different symptoms and modes of spreading.[2]
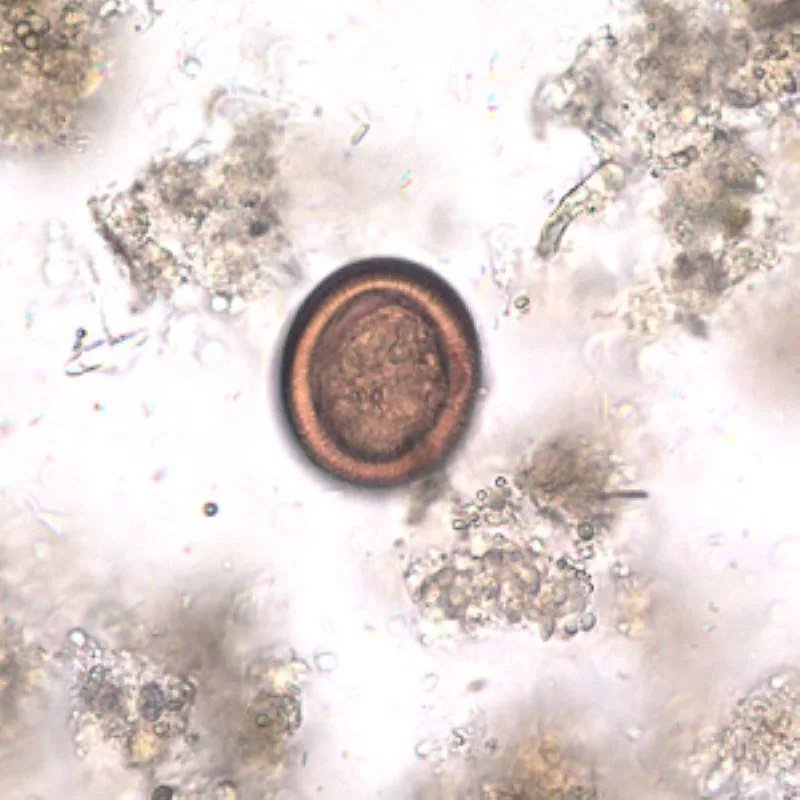
Echinococcus egg in feces. commons wikimedia, Public Domain
The predominant species that are causing human infections are:
- Echinococcus granulosus sensu lato: This is the most prevalent causative agent in the world. This worm measures between 2 and 7 millimeters in length, and it is present in dogs (definitive host) and sheep, cattle, goats, and pigs (intermediate host). It causes cystic echinococcosis (CE), also known as hydatid disease.
- Echinococcus multilocularis: It is 1 to 4 millimeters long; it inhabits foxes, coyotes, and dogs (definitive hosts). It leads to alveolar echinococcosis (AE), which is severe and fatal.
- Echinococcus vogeli and E. oligarthrus: These are tropical species, which cause neotropical polycystic and unicystic echinococcosis, respectively, but only in tropical regions of Central America and South America.
Modern molecular studies show that E. granulosus has multiple genotypes (G1–G10) that have different geographic localities, host preferences, and morphological differences. Such genotypes are becoming recognized as distinct species in current scientific literature, which indicates the complexity of this group of parasites.[3]
Life Cycle of Echinococcosis
The Echinococcus tapeworms have a two-host life cycle.
Definitive Hosts (Carnivores)
Definitive hosts, such as dogs and foxes, have infectious eggs in their intestines and which are shed in their feces. Such eggs are able to persist in the environment for months, polluting soil, water, and plants.[4]
[Image: Image showing the Life Cycle of Echinococcus tapeworms that are responsible for causing Echinococcosis]
The life cycle ofEchinococcustapeworms involves definitive hosts (like dogs and foxes) and intermediate hosts (like sheep or rodents). Humans are accidental hosts who ingest the parasite’s eggs, which can develop into harmful cysts in the liver, lungs, and other organs. This file was from: Echinococcus Life Cycle.png,Public Domain, https://commons.wikimedia.org/w/index.php?curid=99456756
Intermediate Hosts (Herbivores and Humans)
These eggs are ingested by intermediate hosts such as livestock and human beings through contaminated food, water, or soil. The eggs hatch in the intestine, and the larvae migrate to organs such as the liver or lungs, where they develop into cysts over months to years.[5]
Human Role in the Life Cycle
Man remains a dead-end host; we are infected by the accidental ingestion of eggs of contaminated soil, water, or dog hair, but through us, there can be no continuation of the cycle. The resultant cysts, however, may be associated with serious disease.
Echinococcosis Transmission
Humans are infected with echinococcosis by accidentally ingesting Echinococcus eggs in the faeces of infected animals, including dogs and foxes.[6]
The main modes of infection are:
- Direct Contact: Handling of infected dogs, the fur of which has eggs.
- Infected Water/Food: Consuming vegetables that have not been washed, and consuming infected feces in water.
- Environmental Exposure: This is through contact with the soil, which has been defecated by infected animals.
Certain jobs, such as farming and veterinary, are riskier. The disease is not person-to-person transmitted.[7]
Echinococcosis Epidemiology
Echinococcosis is unevenly distributed across the world. The endemic Cystic Echinococcosis (CE) occurs in pastoral regions of the world such as South America, Africa, Central, and the Mediterranean. Alveolar Echinococcosis (AE) is known in the Northern Hemisphere, with China carrying more than 90 percent of AE in the world.[8]
Incidence and Prevalence
Human incidence of CE in endemic regions can be more than 50 per 100,000/year, and prevalence up to 5-10% in some regions of Argentina, Peru, East Africa, and China. The disease is still a major health problem in the world, with an estimated 207,368 new cases of CE in 2019. China has a huge endemic burden as it alone reported more than 72,000 CE and 11,000 AE cases between 2004 and 2022.[9]
Echinococcosis Symptoms in Humans
The problem with echinococcosis is that it may take years or decades before patients develop symptoms. Cystic echinococcosis incubation can take several years, and most patients are not aware of the disease until the cysts have grown large enough to cause dysfunction.[10]
Cystic Echinococcosis Symptoms
The liver and then the lungs are the most frequent locations of hydatid cysts. The symptoms are different in relation to the location, size, and quantity of cysts:[11]
1. Liver Cysts (most common, ~75% of cases):
These cysts cause pain or discomfort in the upper right abdomen with a palpable mass. Other symptoms are nausea and vomiting. If this cyst compresses the bile duct, then jaundice also results. In case of rupture of such a cyst, you can suffer allergic reactions.
2. Lung Cysts (~15% of cases):
The common effects of lung cysts include chronic cough, chest pains, and dyspnea. Fever and allergic symptoms, as well as coughing up cyst fluid or membranes, are typical in the case of rupture.
3. Other Organ Involvement:
- Brain cysts: neurological losses, seizures, headache.
- Bone cysts: Fractures, nerve compression, pain.
- Kidney cysts: Flank pain, Blood in urine.
- Heart cysts: Chest pain, irregular heartbeat, heart failure (rare but serious)
Alveolar Echinococcosis Symptoms
AE closely mimics hepatic carcinoma or cirrhosis and is more commonly diagnosed in people of advanced age. Alveolar echinococcosis is characterised by parasitic tumours in the liver, lungs, brain, and other organs, and if left untreated, can be fatal.[12]
Symptoms include:
- Progressive liver enlargement
- Upper abdominal pain
- Weight loss
- Jaundice
- Fever
- Metastasis symptoms are experienced when the disease spreads to the lungs or the brain.
The tumor-like nature of aggressive growth in AE is vital in making early diagnosis the only way of enhancing outcomes.
Echinococcosis Diagnosis
The diagnosis of echinococcosis is done with the help of clinical examination, radiography, serological tests, and, in some cases, molecular tests. Imaging and serology are the basis of echinococcal infection diagnosis.
Clinical Assessment
The diagnosis of Echinococcosis must be considered in those patients with a history of exposure and positive clinical outcomes. The greatest risk factors are residence or traveling to an endemic region, occupation (as in farming, veterinary work), and contact with dogs in the endemic regions. A significant diagnostic hint is the presence of cystic foci in the organs, such as the liver or lungs, that are discovered on the imaging, though incidental.[13]
Imaging Studies
Ultrasound: The first imaging tool is ultrasound, which is very sensitive to cystic echinococcosis (CE). E. granulosus has a sensitivity of 90% to 95% by ultrasonography. It is portable, cheap, and good at screening and follow-up.[14]
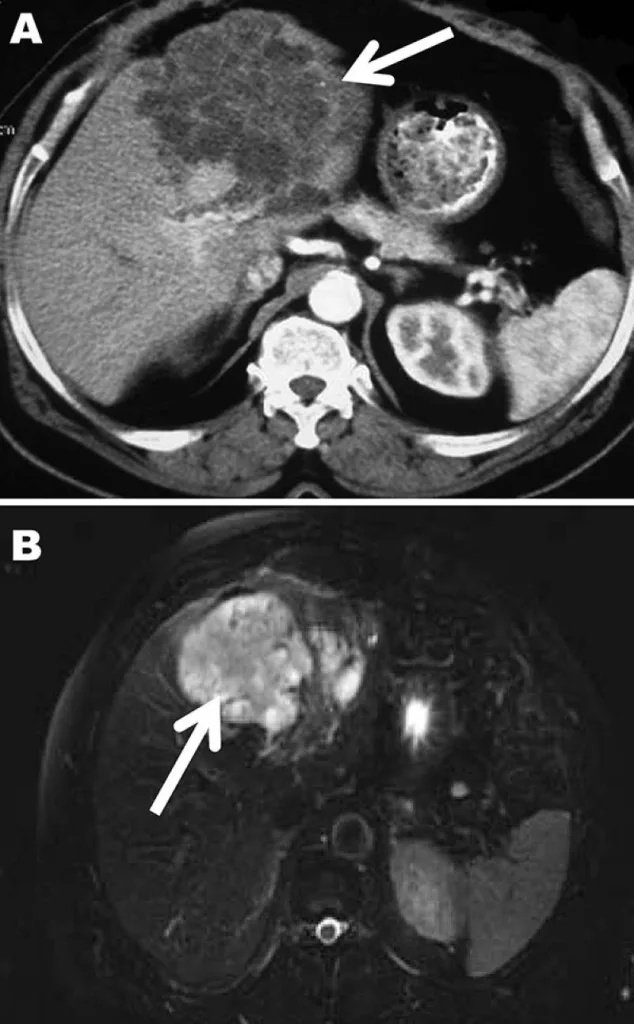
Computed tomography (A) and magnetic resonance (B) images of the liver of a 72-year-old man from French Guiana with polycystic echinococcosis affecting the left side of the liver. White arrows indicate the multicystic liver lesion.Public Domain
CT scans are better for lung cysts and preoperative planning, whereas MRI is superior in determining complications.[15]
WHO Classification System
A cyst classification system (CE1-CE5) by the WHO has been standardized to help identify the management of viability.[16]
| Cyst Stage | Classification | Characteristics | Viability |
|---|---|---|---|
| CE1 | Active | Unilocular fluid-filled cyst with double-wall sign | Active |
| CE2 | Active | Multivesicular cysts with daughter cysts | Active |
| CE3a | Transitional | Detached laminated membrane (water-lily sign) | Variable |
| CE3b | Transitional | Daughter cysts in a solid matrix | Active |
| CE4 | Inactive | Heterogeneous solid content with degenerative changes | Inactive |
| CE5 | Inactive | Solid content with a thick calcified wall | Inactive |
This classification system helps direct the treatment and monitoring strategies.
Echinococcosis Treatment
Treatment of echinococcosis depends on several factors such as the type of cyst, the location of location, size, stage, and the overall health of the patient.
Medical Treatment
Albendazole is the foundation of medical treatment of echinococcosis. It is mostly applied in inoperable, multiple, or small cysts (less than 5 cm) and as adjuvant therapy before and after surgery. The adult dosage is usually 400 mg twice a day, and the courses of treatment would occur over a period of 3-6 months in the case of cystic echinococcosis and at least two years in the alveolar form.[17]
To increase its effectiveness, add praziquantel with albendazole, which increases the protoscolicidal action of albendazole and can help to decrease the relapse rate. Closely monitor the patient with frequent liver testing and imaging to monitor cyst response. The most serious contraindication is pregnancy, especially in the first trimester, in terms of the possibility of teratogenic effects.
PAIR Procedure
PAIR procedure, which is the acronym of Puncture, Aspiration, Injection, and Re-aspiration, is a minimally invasive procedure used to treat certain forms of cystic echinococcosis, most commonly medium-sized CE1 and CE3a liver cysts. It is done under ultrasound or CT guidance, and it is performed by puncturing the cyst, then aspirating the fluid, and injecting a scolicidal agent such as hypertonic saline, and again re-aspirating the contents.[18]
This method has great benefits compared to surgery due to the reduced time of hospitalization and the reduction of complications. Nonetheless, it is not beneficial in cysts with biliary or lung cysts, as well as in complex cysts such as CE2 and CE3b. A modified version, MoCAT, involves the insertion of catheters with the potential to treat these more complex cases.
Surgical Treatment
The ultimate treatment of echinococcosis of a complex or complicated nature is surgical intervention. It is used when the patient has large cysts in the liver (greater than 10 cm), secondarily infected or ruptured cysts, and cysts in vital organs such as the brain, lungs, or kidneys.[19]
The main types of surgery include conservative ones that involve cyst removal with the retention of organ tissue and radical surgeries that totally remove the cyst and all surrounding fibrous capsule. In more severe conditions, especially alveolar echinococcosis, may require partial organ resection or even a liver transplant. The administration of albendazole is of great importance perioperatively to minimize the chances of recurrence due to spilled cyst contents.[20]
Watch-and-Wait Approach
For simple and asymptomatic cysts in the inactive stage of the CE4 and the CE5 phases, a recommended approach is watch-and-wait. It involves routine ultrasound follow-ups (6-12 months) and patient education because only in rare cases do these cysts progress.[21]
Treatment of Alveolar Echinococcosis
Alveolar echinococcosis has to be treated with chemotherapy and or surgery; radical surgery is the most preferable in appropriate cases. The diagnosis is, however, usually made late, making many cases inoperable. In such patients, the long-term, and in most cases, lifelong albendazole therapy is necessary to prevent disease progression. This is the fatal type of the disease, although long-term medical therapy has greatly enhanced the results.[22]
Alveolar Echinococcosis vs Cystic Echinococcosis
Understanding the differences between these two forms of echinococcosis is crucial for appropriate diagnosis and management:[23]
| Feature | Cystic Echinococcosis (CE) | Alveolar Echinococcosis (AE) |
|---|---|---|
| Causative agent | Echinococcus granulosuss.l. | Echinococcus multilocularis |
| Geographic distribution | Worldwide, especially in pastoral regions | Northern Hemisphere only |
| Definitive hosts | Dogs, wild canids | Foxes, coyotes, and rarely dogs |
| Intermediate hosts | Sheep, cattle, goats, pigs | Small rodents (voles, mice) |
| Cyst characteristics | Fluid-filled, well-defined cysts | Tumor-like, infiltrative growth |
| Growth pattern | Slow, expansive | Invasive, metastatic potential |
| Primary organ | Liver (75%), lungs (15%) | Liver (almost exclusively) |
| Natural history | Can remain stable or regress | Progressive without treatment |
| Severity | Generally less severe | More aggressive, often fatal if untreated |
| Incubation period | Years to decades | 5-15 years typically |
| Imaging appearance | Clear cystic lesions with distinct walls | Solid, heterogeneous mass with calcifications |
| Serological response | Variable, stage-dependent | Usually high titers |
| Treatment approach | Surgery, PAIR, or medical therapy | Radical surgery + long-term albendazole |
| Prognosis | Good with appropriate treatment | Poor without complete resection |
| Mortality (untreated) | Low to moderate | 50-75% within 10-15 years |
Prevention and Control
To minimize the risk of getting echinococcosis, advise the tourists to avoid contact with dogs and wild canids in endemic regions; not to drink untreated water in canals, lakes, rivers, and streams; and to follow food and water precautions. Moreover, passengers should observe good hand hygiene after touching dogs and whenever preparing food in the affected localities.[24]
Final Words
Echinococcosis is a serious but neglected health problem in the world. Although it is serious, modern methods are effective in diagnosis and treatment, and therefore, it is important to detect it at the earliest stage. Prevention plays a big role, especially in endemic areas; it is possible through proper washing of vegetables, avoidance of contact with stray dogs, and extensive hand washing. A successful long-term plan should be founded on a One Health approach, in which human and veterinary medicine, agriculture, and social health are harmonized. Reducing the burden of this disease is possible through long-term control programs, research, and the education of the people.
References
[1] Deplazes, P., et al. (2017).Global distribution of alveolar and cystic echinococcosis. Advances in Parasitology, 95, 315-493.
[2] Thompson, R.C.A., & McManus, D.P. (2002).Towards a taxonomic revision of the genus Echinococcus.
[3] Romig, T., et al. (2015). Ecology and life cycle patterns of Echinococcus species. Advances in Parasitology, 95, 213-314.
[4] Eckert, J., & Deplazes, P. (2004). Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clinical Microbiology Reviews, 17(1), 107-135.
[5] CDC. (2019). Echinococcosis Biology. Centers for Disease Control and Prevention.
[6] Moro, P., & Schantz, P.M. (2009). Echinococcosis: a review. International Journal of Infectious Diseases, 13(2), 125-133.
[7] Cardona, G.A., & Carmena, D. (2013). A review of the global prevalence, molecular epidemiology and economics of cystic echinococcosis in production animals. Veterinary Parasitology, 192(1-3), 10-32.
[8] Torgerson, P.R., et al. (2010). The global burden of alveolar echinococcosis. PLoS Neglected Tropical Diseases, 4(6), e722.
[9] Wu, W., et al. (2023). Epidemiological characteristics of human echinococcosis in China from 2004 to 2022. Chinese Journal of Parasitology and Parasitic Diseases.
[10] Brunetti, E., et al. (2010). Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Tropica, 114(1), 1-16.
[11] Pedrosa, I., et al. (2000). Hydatid disease: radiologic and pathologic features and complications. RadioGraphics, 20(3), 795-817.
[12] Kern, P., et al. (2017). The echinococcoses: diagnosis, clinical management and burden of disease. Advances in Parasitology, 96, 259-369.
[13] McManus, D.P., et al. (2012). Diagnosis, treatment, and management of echinococcosis. BMJ, 344, e3866.
[14] Tamarozzi, F., et al. (2014). Ultrasound and cystic echinococcosis. Ultrasound International Open, 1(1), E6-E12.
[15] Stojkovic, M., et al. (2012). Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound? PLoS Neglected Tropical Diseases, 6(10), e1880.
[16] WHO Informal Working Group. (2003). International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Tropica, 85(2), 253-261.
[17] Teggi, A., et al. (1993). Treatment of hydatid disease with mebendazole and albendazole. Antimicrobial Agents and Chemotherapy, 37(8), 1679-1684.
[18] Filice, C., et al. (1990). Percutaneous drainage of hydatid cysts: a new therapeutic approach. Transactions of the Royal Society of Tropical Medicine and Hygiene, 84(3), 457-459.
[19] Sayek, I., et al. (1980). Surgical treatment of hydatid disease of the liver. Archives of Surgery, 115(7), 847-850.
[20] Dziri, C., et al. (2009). Open surgery for hepatic hydatid disease. World Journal of Surgery, 33(7), 1377-1381.
[21] Caremani, M., et al. (1997). Echographic epidemiology of cystic hydatid disease in Italy. European Journal of Epidemiology, 13(4), 455-460.
[22] Brunetti, E., et al. (2010). Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Tropica, 114(1), 1-16.
[23] Gottstein, B., et al. (2015). Immunology of alveolar and cystic echinococcosis (AE and CE). Trends in Parasitology, 31(3), 99-109.
[24] Craig, P.S., & Larrieu, E. (2006). Control of cystic echinococcosis/hydatidosis: 1863-2002. Advances in Parasitology, 61, 443-508.