
{kind=link}

Fecal Incontinence Symptoms Fecal incontinence is when the ability to control one’s bowel movement or gas is lost. It is one of the more distressing but closeted disorders in medicine. Patients are understandably reluctant to bring it up, and many physicians are uncomfortable asking about it.
The psychological impact of this disease on a patient can be catastrophic. Feelings of low self-worth and social isolation can even lead to clinical depression. Yet it is one of the most stigmatized gastrointestinal disorders. Previously believed to be an inevitable consequence of aging, studies now show that fecal incontinence is often preventable, manageable, and sometimes reversible.
Clinician training to be more aware of the condition and proactive questioning when a patient presents to them could change outcomes quite drastically.
How Common is Fecal Incontinence?: Fecal Incontinence Symptoms
Fecal incontinence is not as uncommon as one probably thinks. Real numbers are even higher because it is often unreported, but estimates from worldwide studies are somewhere around 7-8% prevalence in adults.[1]
It affects both sexes, but it’s slightly more common in women (9%). In fact, it affects up to 10% women over 65[2], especially those who have had a history of obstetric or pelvic surgeries, suffer from birth-related injuries, or have chronic bowel disorders.
In the elderly, it may exceed even 10–15% in prevalence because of immobility, cognitive decline, and polypharmacy.
Mechanism of Fecal Incontinence
Normal continence is a balance between four different systems, and it’s the exact cooperation among these four that normally prevents incontinence:
- The internal sphincter maintains a baseline resting tone, while the external sphincter allows voluntary control.
- The rectum acts as a reservoir, stretches to store fecal content, and signals the urge to defecate.
- If stool is too loose (as in diarrhea) or too hard (in impaction), control can become difficult.
- The sacral and pudendal nerves are needed to control both sensory and motor information related to the pelvic floor.
If one or more of these four systems fail (either the structural, functional, or neural aspect), incontinence can result.
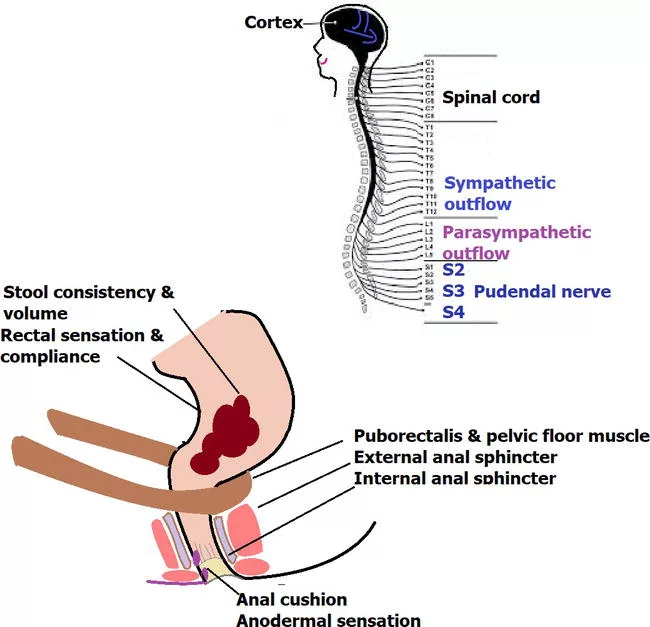
Anatomical and neural pathways involved in fecal continence control. Together, these structures form an integrated system that regulates rectal filling, detects stool consistency, and triggers voluntary or reflexive control during defecation. (Image Courtesy: Tantiphlachiva, K. (2020). Comprehensive Clinical Approach to Fecal Incontinence. IntechOpen. Available fromintechopenand licensed under CC by 3.0)
Causes and Risk Factors of Fecal Incontinence
The risk of acquiring incontinence in one’s lifetime can increase because of numerous factors; however, recognising them can make us better equipped at seeking an early diagnosis.
- Age > 65 years
- Females with a history of obstetric surgeries (childbirth-related trauma or episiotomy)
- Any pelvic or anorectal surgery
- Radiation therapy, e.g., after rectal cancer
- Diabetes, stroke, spinal cord injury, multiple sclerosis
- Chronic bowel dysfunction disorder
- Secondary factors leading to increased intra-abdominal pressure (e.g., obesity, chronic caffeine consumption, chronic laxation use)
1. Obstetric injury:
In women, the condition is the most prevalent with a history of obstetric trauma. Trauma to the anal sphincter complex during vaginal childbirth, particularly when forceps or episiotomy have been used, often leads to weakness or damage of the external anal sphincter and muscles of the pelvic floor. Resultingly, women lose the ability to coordinate these muscles to control defecation.
2. Anorectal Surgery or Injury:
Surgical operations (haemorrhoidectomy, fistulotomy, sphincterotomy) can lead to unintended injury to the innervation of the anal sphincter muscles. Similarly, pelvic fractures or direct injuries to the perineum can injure the continence mechanisms.
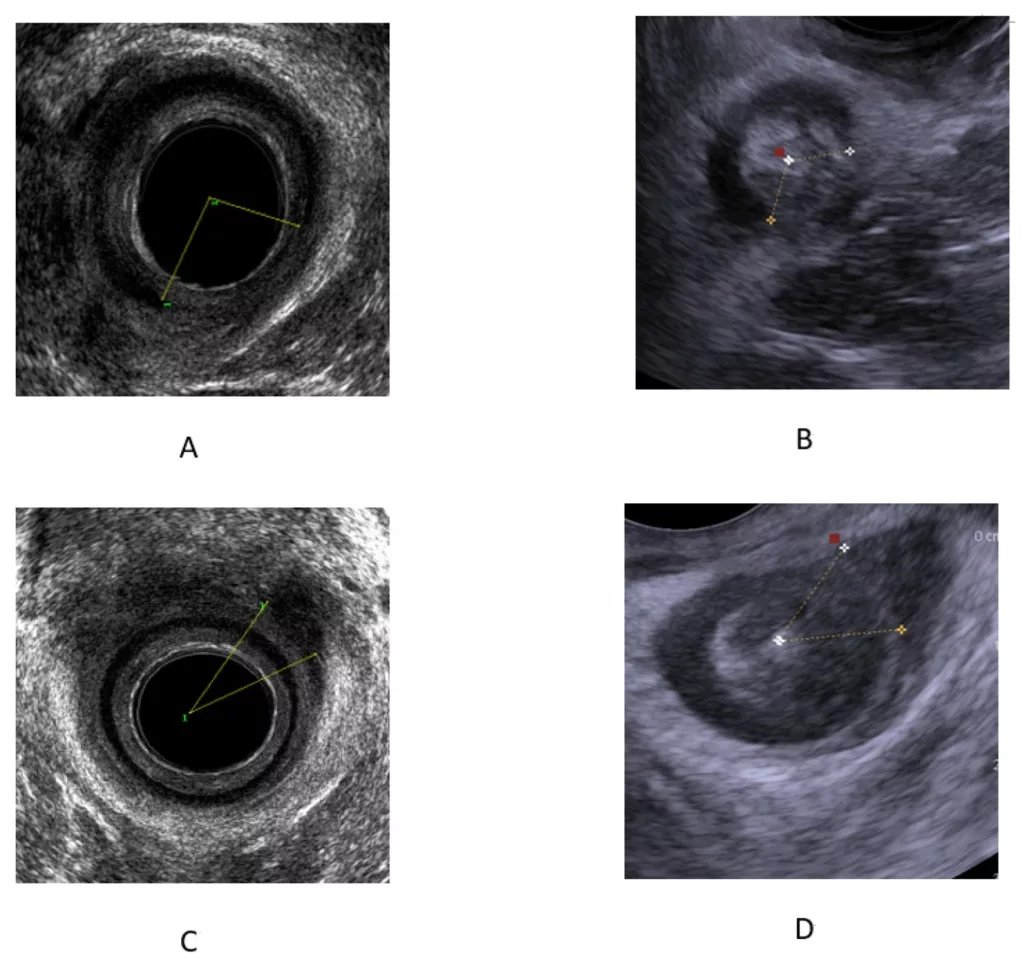
Internal and external anal sphincter tears demonstrated on EAUS and PUS imaging. (A) EAUS showing an IAS tear, (B) PUS showing an IAS tear, (C) EAUS showing an EAS tear, and (D) PUS showing an EAS tear.IAS = internal anal sphincter; EAS = external anal sphincter.(Image Courtesy: Carter, D., Ram, E., & Engel, T. (2022). Combined 3D Endoanal Ultrasound and Transperineal Ultrasound Improves the Detection of Anal Sphincter Defects.Diagnostics,13(4), 682. Available fromMDPIand licensed under CC by 4.0)
3. Post-radiation Fibrosis:
Radiation to the pelvis (for prostate, cervical, or rectal cancer) results in submucosal scarring and loss of elasticity, as well as inflammation of the mucosa (radiation proctitis).[3] The rectum cannot stretch enough to accommodate faecal material, and small volumes result in a sensation of urgency and faecal leakage.
4. Neurological injury:
Damage to the sacral nerves (S2-S4) cuts the communication between the brain, rectum, and anal sphincters. This can occur with a spinal cord injury, sacral plexus being compressed by a tumor, multiple sclerosis, diabetic neuropathy, or surgery. This is called neurogenic incontinence, or autonomic incontinence.[4]
5. Chronic Diarrhea:
When stools are watery and persistent, lasting more than a few days (from IBD, IBS, infections, etc.), the rectum cannot withhold the liquid stool, and the overflow leads to incontinence. It is often seen in neuropathy or a weak rectal sphincter.
6. Fecal Impaction:
On the other hand, when stools are retained for too long in the colon or rectum due to fecal loading, in chronic constipation, the rectum gets blocked with hard stool. Loose, watery stools can then flow around the impacted stool and leak. More common and overlooked in elderly or bedridden patients.
7. Loss of Tone with Age:
As patients grow older, the sphincter muscle tone may decrease, and the rectum may become less compliant and less able to sense if it has become full. This normal aging process may cause incontinence or exacerbate it due to other minor conditions that have arisen.[5]
Types of Fecal Incontinence
| Type | Description | Typical Causes |
|---|---|---|
| Urge incontinence | Strong need to defecate with inability to hold | Diarrhea, reduced external sphincter strength |
| Passive incontinence | Leakage without awareness or urge | Internal sphincter damage, neuropathy |
| Overflow incontinence | Leakage of liquid stool around fecal impaction | Severe constipation, rectal obstruction |
| Mixed incontinence | Combination of urge and passive symptoms | Multifactorial causes, elderly patients |
Symptoms of Fecal Incontinence
Patients are often reluctant to explain the symptoms. They might describe symptoms like soiling their underwear or inability to hold gas. The clinician needs to probe gently, without judgment, to understand the full condition.
Symptoms include:
- Unintentional passage of stool (solid or liquid) or gas
- Urgency or inability to delay defecation
- Sensation of incomplete evacuation
- Perianal irritation or itching
- Emotional distress, embarrassment, and social isolation
Associated features such as rectal pain, bleeding, or mucus discharge should prompt evaluation for inflammatory or structural disease.
Diagnosis of Fecal Incontinence
Diagnosis should aim to find the affected structure, whether the anal sphincter itself, or the rectum, its nerve supply, or the consistency of the stool. So it has to move in a stepwise manner, going from simple clinical evaluation to functional investigations. Proper evaluation of fecal incontinence includes identifying the underlying cause, documenting symptoms, and assigning the fecal incontinence ICD-10 code to ensure accurate medical records and treatment follow-up. The fecal incontinence ICD-10 code is R15.
To rule out other conditions, basic investigations often include stool analysis, colonoscopy (for bleeding or chronic diarrhea), and thyroid or glucose testing if systemic factors are suspected.
1. Clinical Evaluation
- First and foremost is clinical history. It needs a very careful and empathetic history. Main elements of history include the onset and duration of symptoms, consistency of stool, frequency and quantity of leakage, aggravating and relieving factors, obstetric or surgical history, neurological symptoms, and about patient’s routine bowel habits.
- Physical examination includes perianal inspection and digital rectal exam (DRE) to assess sphincter tone, voluntary squeeze, and detect masses.[6]
2. Scoring Assessment
- In most cases, the history and examination of the patient are more than enough for the diagnosis. But in certain cases, symptoms need to be quantified and documented in a proper way for the purpose of guiding treatment and to follow up on decline or improvement.
- For this, there are well-established scores like the Wexner (Cleveland Clinic) Incontinence Score and St. Mark’s score that help record frequency, stool type, and lifestyle impact. These measure frequency, stool type, pad use, and lifestyle impact.
| Type of incontinence | Frequency | ||||
|---|---|---|---|---|---|
| Never | Rarely | Sometimes | Usually | Always | |
| Solid | 0 | 1 | 2 | 3 | 4 |
| Liquid | 0 | 1 | 2 | 3 | 4 |
| Gas | 0 | 1 | 2 | 3 | 4 |
| Wears pad | 0 | 1 | 2 | 3 | 4 |
| Lifestyle alteration | 0 | 1 | 2 | 3 | 4 |
The Jorge-Wexner (Cleveland Clinic) Incontinence Score7Jorge, J. M., & Wexner, S. D. (1993). Etiology and management of fecal incontinence. Diseases of the colon and rectum, 36(1), 77–97. https://doi.org/10.1007/BF02050307Never = 0; Rarely = <1/month; Sometimes = <1/week but >1/month; Usually = <1/day but >1/week; Always = >1/day.
3. Functional Investigations
These are a great way of testing the function of the anal sphincters and rectum under normal and stressed conditions.[7]
- Anorectal Manometry: Measures resting pressure, squeeze pressure, sensation, and compliance. In general, a low resting pressure implies a weak internal sphincter, and a low squeeze pressure implies a weak external sphincter.
- Defecography: Shows dynamic evacuation and pelvic floor motion (for prolapse).
- Electromyography: This evaluates the integrity of the pelvic floor and nerve supply to the sphincters.
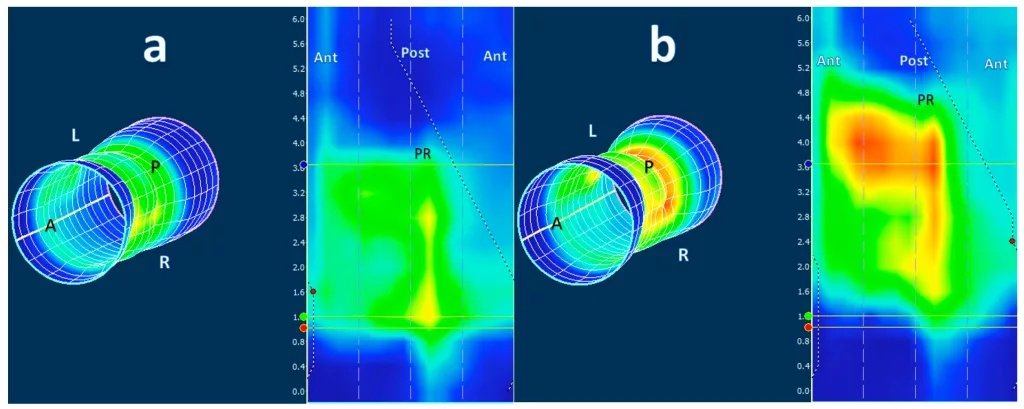
2D and 3D anorectal manometry images from a 45-year-old man with fecal incontinence: (a) Shows low resting anal pressure, while (b) shows reduced squeeze strength, especially in the anterior segment (blue).PR = puborectal muscle; ATN = anterior; POST = posterior; L = left; R = right.The cylindrical pressure map is “unrolled” into a 2D image, which is why the anterior section appears on both sides (Image Courtesy: Van Oostendorp, J. Y., Van Hagen, P., H., G. J., & M., I. J. (2022). Study on 3D High-Resolution Anorectal Manometry Interrater Agreement in the Evaluation of Dyssynergic Defecation Disorders.Diagnostics,13(16), 2657. Available fromMDPIand licensed under CC by 4.0)
4. Structural Imaging
Imaging studies of the pelvis help clinicians better identify if a component of pelvic anatomy is causing the symptoms (because anatomical defects indicate that surgical correction is needed).
- Endoanal ultrasound shows anal muscles in motion and can highlight areas of tears, thinning, or defects (especially postpartum or post-surgical).
- MRI defecography allows a look at pelvic floor descent, rectocele, intussusception, or prolapse.
- Pelvic MRI is useful for complex or recurrent cases when soft-tissue details are needed.
Treatment of Fecal Incontinence
For the treatment of fecal incontinence, the approach is to start with the least invasive treatment, going up in aggressiveness if that fails. In current practice, most providers are going to offer conservative treatments before anyone broaches the subject of surgery.
A. Conservative Measures and Behavioral Therapy
Most people are going to be started on conservative measures, especially those with mild to moderate severity. These could include:
- Bowel habit training is getting the patient to follow a schedule of regular, predictable bowel movements and train them to go after meals when the gastrocolic reflex is strongest. This training helps them learn to “feel” and “time” rectal filling.
- Somewhat surprisingly, much of the time you need to only fix the stool consistency:
- For pelvic floor muscle training, Kegel exercises for fecal incontinence, and biofeedback therapy[8] (by trained physiotherapists) improves the strength of the external sphincter, rectal sensation, and coordination. Biofeedback is one of those underappreciated solutions that really help, as long as the patient is motivated to get better.
- In fact, when combined with cognitive behavioural therapy (CBT), it can improve the symptoms in motivated individuals up to 70%.
B. Diet for Fecal Incontinence
Minor changes to diet can make a big difference, such as food spacing and avoiding eating late at night. These are likely to be different for different patients, but the usual advice on diet is as follows:
- Soluble fiber to increase stool bulk (10–20 g/day) (oats, psyllium, bananas)
- Stay hydrated, but spread fluid intake evenly through the day, at least 1.5-2L water daily.
- Avoid trigger foods: caffeine, alcohol, spicy meals, fatty foods.
- Identify and remove individual triggers and intolerances like lactose, artificial sweeteners, and high-FODMAP foods.
C. Pharmacologic Therapy
When conservative measures don’t seem to work, the clinician might move to pharmacological options. For example
- Antidiarrheals like loperamide and codeine reduce bowel motility.
- Barrier creams (zinc oxide, petroleum jelly) prevent skin irritation.
- Bile acid sequestrants might help with bile acid–related diarrhea after cholecystectomy.[9]
- Antibiotics or probiotics may help in small intestinal bacterial overgrowth (SIBO)-related cases.
- Phenylephrine gel or adrenergic agonists as topical agents may increase sphincter tone.
D. Supportive Measures and Fecal Incontinence Products
In addition to medical and behavioral therapies, fecal incontinence products play an important role in improving daily comfort and quality of life. These include adult diapers for fecal incontinence, fecal incontinence pads, and specially designed fecal incontinence underwear. Using these products can help patients maintain dignity, prevent skin irritation, and manage accidents while they continue medical or behavioral treatments.
E. Surgical Options
For those who are not responding to conservative treatment and have gross anatomical defects, surgery is one of the only options.
- Sphincteroplasty (repair of the anal sphincter) is advised for obstetric and traumatic tears. Best results are seen if done early.
- Sacral nerve stimulation is a minimally invasive treatment involving insertion of a small implant (a pacemaker) device, which provides low-voltage stimulation to the sacral nerves. This treatment can improve the movement and strength of the sphincter muscles and also rectal sensation. It’s one of the most effective modern treatments, with up to 70–80% long-term improvement.[10]
- Injectable bulking agents provide extra support to the walls of the anal canal in cases of mild incontinence.
- Artificial bowel sphincters are very rarely used, reserved for severe, refractory cases only.
- Stoma creation (colostomy) is the last-resort option in severe, unmanageable incontinence when all other options fail.
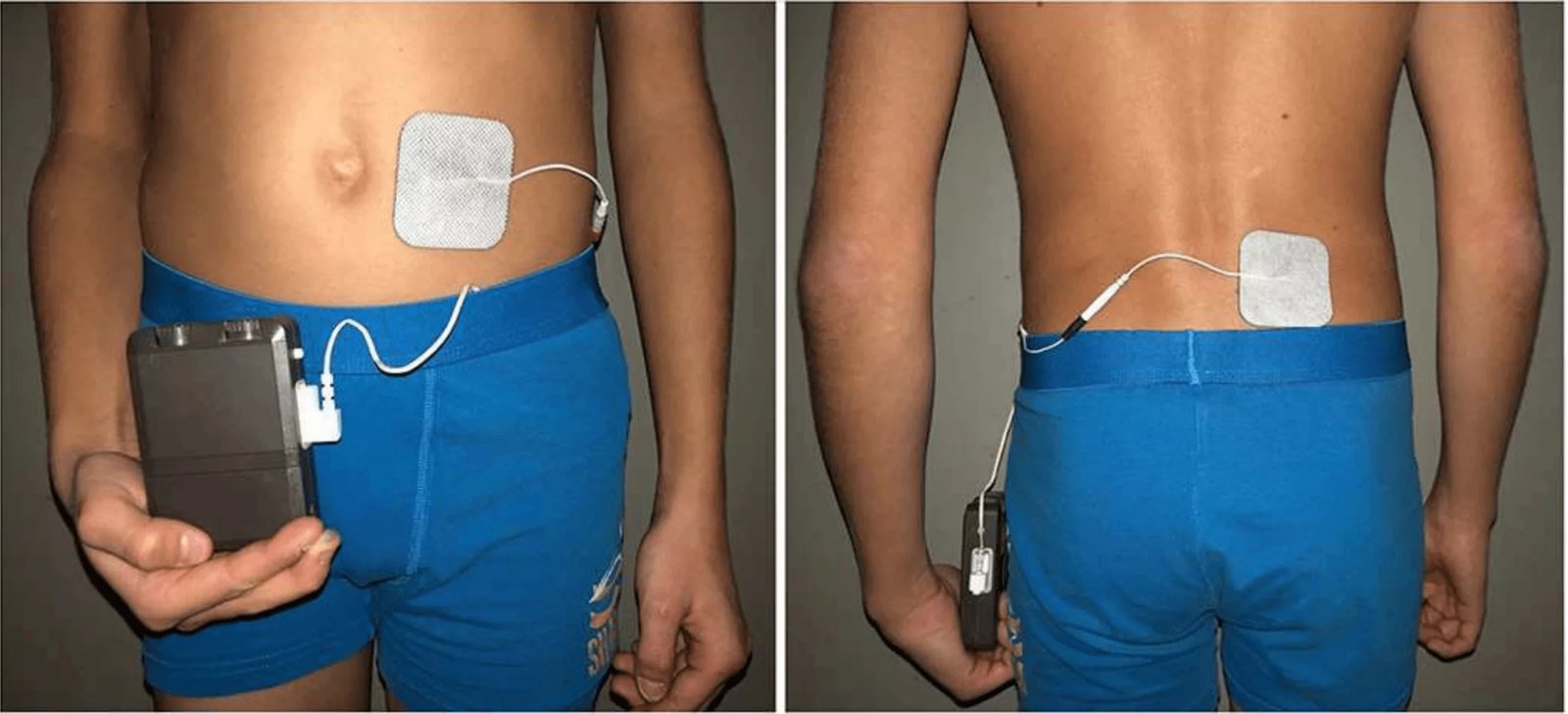
Sacral nerve stimulation in a patient with a pacemaker. The ventral electrode is placed on the left side near the umbilicus, while the dorsal electrode sits on the right paravertebral area. Together, these positions deliver targeted stimulation to support continence control. (Image Courtesy: Besendörfer, M., Kohl, M., Schellerer, V., Carbon, R., & Diez, S. (2020) A Pilot Study of Non-invasive Sacral Nerve Stimulation in Treatment of Constipation in Childhood and Adolescence.Frontiers in Pediatrics,8, 529947. Available fromFrontiersand licensed under CC by 4.0)
Complications of Fecal Incontinence
With it being such a social taboo, the implications are both physical and psychological. Physical complications include perianal dermatitis, recurrent urinary tract infections, rectal prolapse, and poor pelvic floor function. Psychological effects include clinical depression, anxiety, social isolation, and sexual dysfunction.
In many cases, the psychological sequelae outweigh the physical problems.
Prognosis and Quality of Life
While it is difficult to guarantee a 100% cure, in most cases, symptoms can be reduced to a great extent, and the lifelong prognosis can be improved. If diagnosed early, put on the best available therapy as per the cause, and regular follow-up is ensured, the best outcomes can be guaranteed.
Psychological support and patient education are really important as several patients suffer for years but avoid going to a healthcare provider. By addressing the social taboo, we can definitely encourage people to reach out with early symptoms and adhere to the management plan.
Final Word
Fecal incontinence is more common than we realize, but a lot of people are too embarrassed to discuss it with a healthcare provider. It is a pathological condition that can result from the failure of one or more of the systems that normally control continence (i.e., motor, sensory, and behavioral components). It is both a physiological and psychological disorder. For most patients, it’s a fight to regain control over their lives.
The options available today in terms of pelvic floor therapy and neuromodulation are more encouraging than ever before. The prognosis is good, as long as patients can be identified early and counselled through the plan.
References
[1] Mack, I., Hahn, H., Gödel, C., Enck, P., & Bharucha, A. E. (2023). Global Prevalence of Fecal Incontinence in Community-Dwelling Adults: A Systematic Review and Meta-analysis. Clinical Gastroenterology and Hepatology: The Official Clinical Practice Journal of the American Gastroenterological Association, 22(4), 712. https://doi.org/10.1016/j.cgh.2023.09.004
[2] Mack, I., Hahn, H., Gödel, C., Enck, P., & Bharucha, A. E. (2023). Global Prevalence of Fecal Incontinence in Community-Dwelling Adults: A Systematic Review and Meta-analysis. Clinical Gastroenterology and Hepatology : The Official Clinical Practice Journal of the American Gastroenterological Association, 22(4), 712. https://doi.org/10.1016/j.cgh.2023.09.004
[3] Putta, S., & Andreyev, H. J. (2005). Faecal incontinence: A late side-effect of pelvic radiotherapy.Clinical oncology (Royal College of Radiologists (Great Britain)),17(6), 469–477. https://doi.org/10.1016/j.clon.2005.02.008
[4] Emmanuel A. (2019). Neurogenic bowel dysfunction.F1000Research,8, F1000 Faculty Rev-1800. https://doi.org/10.12688/f1000research.20529.1
[5] Goodman, C., Malone, J. R., Norton, C., Harari, D., Harwood, R., Roe, B., Russell, B., Fader, M., Buswell, M., Drennan, V. M., & Bunn, F. (2015). Reducing and managing faecal incontinence in people with advanced dementia who are resident in care homes: Protocol for a realist synthesis. BMJ Open, 5(7), e007728. https://doi.org/10.1136/bmjopen-2015-007728
[6] Shah R, Villanueva Herrero JA. Fecal Incontinence. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459128/
[7] Jorge, J. M., & Wexner, S. D. (1993). Etiology and management of fecal incontinence. Diseases of the colon and rectum, 36(1), 77–97. https://doi.org/10.1007/BF02050307
[8] Rao, S. S. (2010). Advances in Diagnostic Assessment of Fecal Incontinence and Dyssynergic Defecation. Clinical Gastroenterology and Hepatology, 8(11), 910-919.e2. https://doi.org/10.1016/j.cgh.2010.06.004
[9] Lee, D., & Arora, G. (2014). Medical Management of Fecal Incontinence in Challenging Populations: A Review. Clinics in Colon and Rectal Surgery, 27(3), 91. https://doi.org/10.1055/s-0034-1384661
[10] Hite, M., & Curran, T. (2021). Biofeedback for Pelvic Floor Disorders. Clinics in colon and rectal surgery, 34(1), 56–61. https://doi.org/10.1055/s-0040-1714287
[11] Huang, R. L., Huang, W. K., Xiao, X. Y., Ma, L. F., Gu, H. Z., & Yang, G. P. (2023). Diagnosis and treatment of post-cholecystectomy diarrhoea. World journal of gastrointestinal surgery, 15(11), 2398–2405. https://doi.org/10.4240/wjgs.v15.i11.2398
[12] Brill, S. A., & Margolin, D. A. (2005). Sacral nerve stimulation for the treatment of fecal incontinence. Clinics in colon and rectal surgery, 18(1), 38–41. https://doi.org/10.1055/s-2005-864079