
, also known as vanishing bone disease, is a rare disorder in which progressive osteolysis...){kind=link}

Gorham Stout Disease Gorham-Stout Disease (GSD), also known as vanishing bone disease, is a rare disorder in which progressive osteolysis occurs in association with proliferation of abnormal lymphatic and vascular channels; affected bone is progressively resorbed and replaced by angiomatous/lymphatic tissue. Other names used are phantom bone disease or massive osteolysis.osteolysis.”Journal of Bone and Joint Surgery, 36-A(4), 802-803.” style=”position:relative;color:#309b65;cursor:help;border-bottom:1px dotted #309b65;font-weight:bold”>[1]
What Exactly Is Gorham-Stout Disease?: Gorham Stout Disease
Gorham-Stout Disease is a rare disorder involving the progressive disappearance of bone due to abnormal proliferation of vascular and lymphatic channels. Over time, these channels invade normal bone and replace it with fibrous connective tissue, a process known as osteolysis. This may occur in any bone of the body, but in most cases involves ribs, spine, pelvis, skull, and shoulder girdle.[2]
Gorham-Stout Disease Prevalence
This is a sporadic bone disease that has been baffling medical practitioners since it was first described in 1955. Gorham Stout disease has a prevalence of 1 case per 1-2 million people, and less than 300 cases have been reported in the medical literature worldwide. [3]
There is no gender discrimination in the disease, and it may appear at any age, but it most commonly appears in children and young adults below 40 years of age.[4] No genetic pattern, racial predisposition, or lifestyle factor has been known to cause or prevent this condition. The cases seem to be randomly and spontaneously occurring.
What Causes Bones to Vanish?
The precise pathophysiology of the Gorham-Stout disease is still not known, but various theories have surfaced as a result of decades of study. The most popular theory is the anomalous angiogenesis, which is the formation of new vessels and the lymphangiogenesis, or the creation of new lymphatic vessels. . These abnormal vessels grow within the bone and are thought to release factors that increase bone resorption by activating osteoclasts (cells that break down bone). The imbalance between bone formation and resorption results in progressive osteolysis.[5] Other researchers think that the following conditions can provoke the disease:
- Microtraumas of the affected area (most patients do not remember any particular injury)
- Any changes in blood flow or oxygen levels in the bone
- Unusual bone cell signaling with the blood vessels.
- Possible genetic mutations of vascular growth factors (no genetic marker has been found)
Recognizing the Symptoms: What Does Vanishing Bone Disease Look Like?
The symptoms of the Gorham-Stout disease differ significantly based on what types of bones are affected, the rate of osteolysis, or the development of complications.
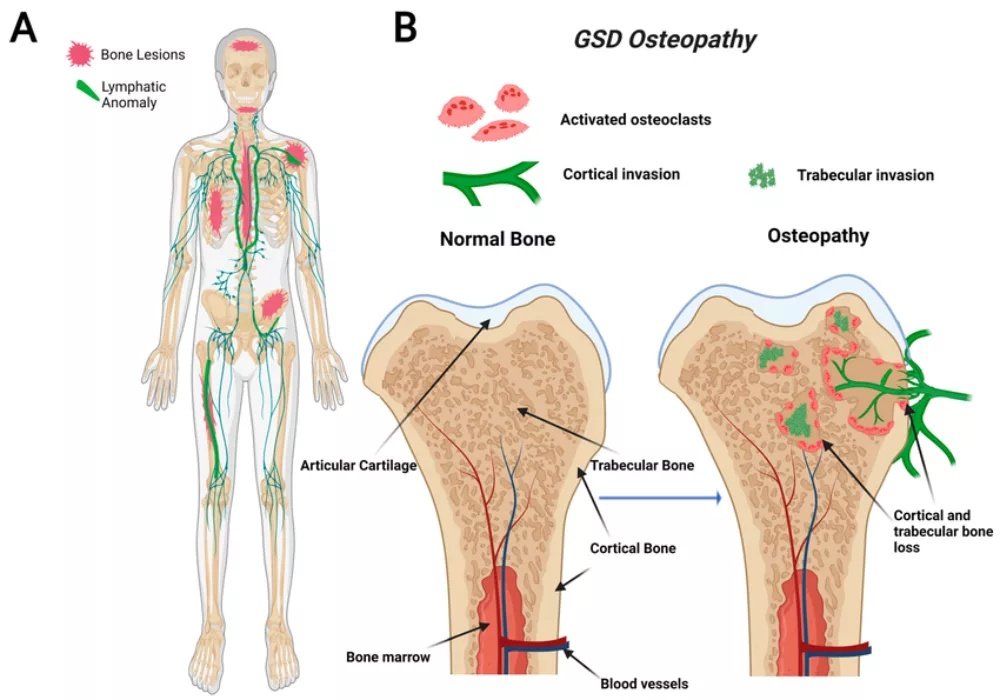
Symptoms associated with Gorham–Stout disease (GSD): panel A shows regionally aggressive bone loss due to abnormal lymphatic invasion, panel B depicts resorption of both cortical and trabecular bone. From Solórzano-Zepeda E. et al., Osteopathy in Complex Lymphatic Anomalies, International Journal of Molecular Sciences 23:8258 (2022). Licensed under CC BY 4.0.
Symptoms that are common at early stages include:
- Pain in the affected area: The pain in the affected body part is normally an aching, chronic pain that may worsen as the individual increases activities.
- Diffuse swelling or mass of the soft tissues: This may be caused by the absence of bone, which makes it swell or change the contour on touch.
- Restricted movement: This is especially true when the joints are close to the affected bone.
- Weakness or instability: The impaired bone cannot sufficiently support the structures in place.
- Pathological fractures: Bones can either fracture with a slight injury or, in some cases, they can also break on their own due to weakness.
Most patients ignore such symptoms altogether as sports injuries, growing pains, or arthritis, resulting in delayed diagnosis. The disorder can either be accidentally identified in an imaging procedure done to rule out another condition, or a fracture happens.[6]
Symptoms according to Location:
In some locations, being affected by this rare bone disorder, more severe complications may arise:
- Spinal involvement may result in neurological symptoms in case of vertebral collapse and may consequently result in nerve compression, pain along the arms or legs, numbness, tingling, or, in extreme instances, paralysis.[7]
- Skull involvement may present with headaches, facial asymmetry, dental problems, or vision changes if bones around the eye socket are affected.
- The most perilous is the involvement of the ribs and the chest wall. In case of the GSD of the ribs or thoracic spine, there are life-threatening complications such as chylothorax, or lymphatic fluid accumulation in the chest cavity. This is so because the abnormal lymphatic vessels may overflow or burst, releasing the space around the lungs with chyle (a milky fluid with the fats that are digested). Chylothorax leads to dyspnea, chest pains, and may severely impair the functions of the lungs.[8]
The Diagnosis to Identify Vanishing Bone Disease
It is hard to diagnose Gorham-Stout Disease, as the majority of physicians will never see such a case in their career. The knowledge of how the Gorham-Stout disease diagnosis process occurs will make the patient aware of what to expect and the reason why several tests are essential.[9]
Imaging Studies:
The basis of diagnosis lies in the imaging studies.
- Plain X-rays can also be used to demonstrate bone loss, and sometimes referred to as the sucked candy appearance, which shows the edge of the bone dissolved.
- The CT scans enable detailed 3-dimensional views of the bone destruction, and the extent of the involvement can be established.
- MRI scans are especially useful as they can detect the changes in soft tissues and vascular growth, and early bone marrow alterations in advance, before bone loss would be evident under an X-ray.[10]
Bone Biopsy:
A bone biopsy is normally necessary to give a definitive diagnosis. A biopsy refers to a small sample of the affected tissue and bone that is put under the microscope. Biopsy shows several thin-walled vascular and lymphatic channels rather than normal bone tissue.[11]
Laboratory Findings:
In GSD, blood tests are usually normal, which in fact aids in making a difference with other disorders. Levels of calcium, alkaline phosphatase (a bone formation marker), and inflammatory markers are typically within the normal range. These tests are mainly done to rule out other conditions such as cancer, infection, or metabolic bone diseases.[12]
Differential Diagnosis:
The doctors need to exclude the diseases that could be similar to GSD, such as bone cancers, infections, such asosteomyelitis, vascular malformations, and other rare bone diseases, such asfibrous dysplasiaor Paget disease.
Gorham-Stout Disease Prognosis
The prognosis of the Gorham Stout disease is immense and different in every patient, and so, doctors are not in a position to give a confirmed prognosis during diagnosis. Nevertheless, it is possible to prepare and plan by knowing the factors affecting the outcomes.[13]
Some patients experience spontaneous stabilization or remission. The bone loss merely ceases its progression due to unknown reasons, and with proper support and supervision, the patients can lead rather normal lives. It has been estimated that in about 40-50 percent of patients, spontaneous stabilization of the disease is attained. Lucky people can experience some bone loss that is confined to a small region that does not have a great effect on functionality.[14]
Others have progressive disease, where osteolysis persists for years and may involve more than one bone. This progressive variant needs constant treatment and care to ensure the quality of life and avoid complications.
The most severe type of the disease is thoracic and is associated with chylothorax, which should be treated aggressively.
Life Expectancy & Long-Term Results
The main aspects that influence the life expectancy of Gorham-Stout disease are:[15]
Location of Bone Involvement:
In the past, thoracic (chest) involvement with chylothorax was fatal (30-50%). Modern aggressive management using medications, surgical procedures, and nutrition support has, however, lowered these numbers largely. When the thoracic involvement is absent, the survival rates of patients are usually excellent in the long run.
Age at Diagnosis:
Younger patients often have better regenerative capacity and longer treatment windows, though the disease can be successfully managed at any age.
Response to Treatment:
Near-normal life expectancy is seen in patients who have attained disease control using medication – especially bisphosphonates or newer agents such as sirolimus. A good quality of life is enjoyed by many patients even decades after diagnosis.
No Complications:
In cases where the disease attacks extremities as compared to vital structures, patients tend to overcome the illness and live normal lives.
Availability of Specialized Care:
A patient should be treated at a center that has experience with rare bone disorders because teams can engage in multimodal approaches to treatment within a short period of time.
It should also be mentioned that though the Ghonham-Stout Disease may be severe and life-altering, most patients have been able to stabilize the disease through treatment and lead healthy lives. Tackling the medical community has assisted in the increased recognition and the early diagnosis of this condition, and the outcomes of the same are expected to improve in the future.
Treatment Approaches: Managing Vanishing Bone Disease
Since the Gorham-Stout Disease is extremely rare and the cause is still unknown, there is no cure or standard treatment procedure approved by the FDA. The GSD needs a multidisciplinary team of:
- Orthopedic surgeons
- Medical oncologists
- Interventional radiologists
- Thoracic surgeons, and
- Other experts based on the location of the disease.
Medical Therapies:
The most popular drugs used in the treatment of GSD are bisphosphonates.[16] Drugs such as zoledronic acid or pamidronate have been promising in reducing or preventing bone loss in most patients with Gorham-Stout Disease. Treatment can be carried out over months and years, and monitored frequently to determine response.
- Interferon alfa-2b is an anti-inflammatory drug. It acts by suppressing the growth factors, which are stimulated to develop abnormal blood vessels.[17]
- Some Immunosuppressive drugs, such as sirolimus (Rapamycin), have a remarkable response in several cases that do not respond to other treatments and stabilize.[18]
Radiation Therapy:
Selective cases have been treated with radiation therapy. Radiation of low dose may have the potential to slow down the vascular growth, which is responsible for bone loss, but it is restricted by the effects of long-term radiation exposure, especially in children.[19]
Surgical & Interventional Procedures:
When bone loss causes structural predominance or instability, reconstructive surgery might be required, and this involves bone grafting, but it is sometimes dependent on the course of the disease.[20] To stabilize the affected areas, some patients require joint replacement or spinal fusion surgery.
Management of chylothorax is critical for thoracic involvement. The following interventions are involved:
- Thoracic duct ligation[21]
- Sclerotherapy to seal leaking lymphatic vessels, or
- Repeated thoracentesis (drainage of fluid from the chest) to relieve symptoms.
During treatment, patients usually need to be put on a specific low-fat diet (Medium Chain Triglyceride diet) to lower the chyle production.
Supportive Care Strategies:
- Physical therapy is used to keep affected areas strong and functional, as well as instruct patients on how to treat weakened bones and also aid in mobility in case bone loss occurs in weight-bearing bones.
- Management of pain can be done with the use of medications, nerve blocks, or the use of complementary methods to manage pain, such as acupuncture, to enhance quality of living without necessarily using opioid drugs.
- Nutritional support is crucial, especially for patients with chylothorax, who require adjustments to their diet. Collaboration with a registered dietitian helps to maintain proper nutrition as well as treat symptoms.
- The psychological support should not be disregarded. Having a rare and unpredictable disease is not easy to live with. Emotional support and effective coping techniques are helpful with mental health professionals, support groups, or even other GSD patients.[22]
Conclusion
Gorham-Stout Disease is a rare and unpredictable disease; however, with the knowledge about it, patients and caregivers can make informed decisions and take an active role in their care. A combination of better diagnostic methods, increased treatment methods, and increasing medical awareness is a real hope.[23]
It is worth remembering that modern medicine has gone a long way in treating rare bone diseases. With full-time provision and access to learned experts, a good number of patients live to enjoy worthwhile active lives. Your bones might be fading away, but your power, your heart, your faith is tough–and you are not going this round single-handedly.
References
[1] Gorham, L. W. (1954). “A most unusual syndrome of bone destruction: Progressive osteolysis.”Journal of Bone and Joint Surgery, 36-A(4), 802-803.
[2] Rohacek, R. et al. “Current concepts from diagnosis to management in Gorham–Stout disease: a systematic narrative review of about 350 cases.”Eur Orthop Relat Res.2022;7(1):0083.
[3] Javid, F. et al. “Clinical features and current management experience in Gorham-Stout disease.”Orphanet J Rare Dis.2025;20(1):
[4] Dickson, J. H., Camp, J. F., & Tillman, B. P. (1972). “Gorham’s disease in females.”The Journal of Bone and Joint Surgery, 54(2), 289-297.
[5] Mangham, D. C., Gelezo, H. J., & Grimer, R. J. (1998). “Gorham’s disease: Osteoclastic hemangiomatosis of bone.”British Journal of Radiology, 71(849), 968-971.
[6] Devereaux, M. D., McLatchie, G. R., & Ramet, M. (1993). “Gorham’s disease of the lower limb: A case report with review of the literature.”The Knee Journal, 8(1), 45-50.
[7] Boriani, S., Bacchini, P., & Bertoni, F. (1992). “Gorham’s disease of the spine: Report of four cases.”Spine, 17(10), 1205-1212.
[8] Ohba, T., Ebata, S., & Shibata, M. (2009). “Chylothorax as a complication of Gorham’s disease affecting the ribs and spine.”European Spine Journal, 18(2), 247-253.
[9] Rohacek, R. et al. “Current concepts from diagnosis to management in Gorham–Stout disease: a systematic narrative review of about 350 cases.”Eur Orthop Relat Res.2022;7(1):0083.
[10] De Backer, T. L., Vanhoenacker, F. M., & Vandamme, M. (2006). “Imaging of Gorham’s disease: The role of MRI in disease assessment.”Radiology Review, 41(3), 312-325.
[11] Heffez L., Doku H.C., Carter B.L., Feeney J.E. “Perspectives on massive osteolysis: Report of a case and review of the literature.”Oral Surg Oral Med Oral Pathol.1983;55(4):331-43.
[12] Rubin, R., & Cassarino, D. S. (2003). “Gorham’s disease: Pathologic findings and diagnostic biopsy criteria.”Archives of Pathology & Laboratory Medicine, 127(4), 420-425.
[13] Pons-Estel, G. J., Massardo, L., & Catoggio, L. J. (2003). “Gorham’s disease with progressive osteolysis: Impact on quality of life and psychological outcomes.”Orphanet Journal of Rare Diseases, 8(1), 124.
[14] Hu, X. et al. “Gorham–Stout syndrome: a chylothorax disease with bony destruction.”Medicine (Baltimore).2022;101(21)
[15] Lala, S., James, S. L., & Carrasco, C. H. (1998). “Gorham’s disease: Long-term outcome in 28 patients.”American Journal of Orthopedic Surgery, 27(2), 116-123.
[16] Kannan, R. Y., Freeman, T. A., & Reeves, R. H. (2006). “Bisphosphonates in the management of Gorham’s disease: A case series.”Journal of Bone and Mineral Metabolism, 24(6), 458-465.
[17] Özcan, C., Rimondi, E., & Cebesoy, O. (2012). “Interferon alpha-2b in the treatment of Gorham’s disease: Results from an international multicenter trial.”Bone, 50(1), 279-285.
[18] Li, Y. et al. “Gorham–Stout disease successfully treated with sirolimus (rapamycin): a case report and review of the literature.”BMC Musculoskelet Disord.2020;21:577.
[19] Heyd R., Micke O., Surholt C., Berger B., Martini C., Füller J. “Radiation therapy for Gorham‐Stout syndrome: results of a national patterns-of-care study and literature review.”Int J Radiat Oncol Biol Phys.2011;81(3):e179-85.
[20] Heithold, R. S., Lacey, J. A., & Lougheed, T. E. (1995). “Management of chylothorax in Gorham’s disease: Surgical and medical approaches.”Chest Surgery Clinics of North America, 5(3), 519-531.
[21] Boles, C. A., Chen, S., & Loevner, L. A. (2004). “Thoracic duct embolization for chylothorax associated with Gorham’s disease.”Journal of Vascular and Interventional Radiology, 15(10), 1151-1155.
[22] Floter, M. C., Hölzle, F., & Kessler, P. (2013). “International registry of Gorham’s disease: Preliminary data from 156 patients.”Orphanet Journal of Rare Diseases, 8(1), 61.
[23] (Momanu A., Caba L., et al.)Medicina.2021;57(7):681.