
{kind=link}

Hepatomegaly Enlarged Liver The liver is the body’s metabolic powerhouse. It is responsible for several vital functions, from filtering toxins to producing vital proteins, as well as regulating blood sugar. Despite doing this heavy lifting all the time, it is a resilient organ, so early disease is usually silent and goes undiagnosed.
One of the most common anomalies with the liver is hepatomegaly, which is the clinical term for an enlarged liver, and while it is not a disease in itself, it is a clinical sign of an underlying condition. In modern times, with the sheer amount of processed food and metabolic stress we face, mild hepatomegaly has become the most common incidental finding in clinical practice.
What is Hepatomegaly?: Hepatomegaly Enlarged Liver
Hepatomegaly is the medical term for a liver that is larger than it should be. Now, the normal liver size varies based on age, sex, and body size. However, clinicians generally use the liver span: the distance between the top and bottom edges of the liver, to determine if it is enlarged.
For a typical adult, a liver span of over 12.5 to 13cm in the midclavicular line is generally considered enlarged.
When a doctor performs a physical exam, they use palpation (pressing with the fingers) and percussion (tapping to hear the change in density) to find the liver’s edge. Usually, the edge of the liver is not felt significantly below the rib cage. If it’s felt more than 2 cm below the ribs, it suggests enlargement.
Common Causes of Enlarged Liver
Hepatomegaly is a physiological response to one of four processes: storage, inflammation, congestion, or rarely, space-occupying lesions.
1. Storage
In modern clinical practice, this is the most frequent cause we see. The liver enlarges because it can no longer process the substances it is supposed to store.
- The primary culprit is hepatomegaly with steatosis (fatty liver). We see this in MASLD, formerly called NAFLD (non-alcoholic fatty acid disease), where droplets of triglycerides accumulate inside liver cells.
- Other less common storage disorders include amyloidosis, where rare proteins build up in the tissue, or Hemochromatosis, which is because of iron overload. In hemochromatosis, the iron often manifests externally as a bronze-colored skin tint.
- In pediatric cases, we also look for Glycogen Storage Diseases, where genetic defects prevent the liver from breaking down glycogen, leading to massive, visible enlargement.
2. Inflammation
When the liver is attacked, it becomes inflamed, swollen, and tender to the touch. This is an acute defense mechanism. Viral infections like Hepatitis cause rapid swelling that is often painful to the touch.
However, inflammation isn’t always viral. Drug-Induced Liver Injury is a rising concern, often triggered by high-dose acetaminophen, excessive alcohol consumption, or unregulated herbal detox supplements. In some cases, the body’s own immune system mistakenly attacks the liver, a condition known as Autoimmune Hepatitis. While acute inflammation is reversible, chronic swelling eventually leads to the permanent scarring we call cirrhosis.
3. Congestion
The liver is one of the most vascular organs in the body. If blood cannot flow out of the liver and back toward the heart, the organ becomes engorged with blood. This is most often seen in Congestive Heart Failure, where the right side of the heart is weak, so blood backs up into the hepatic veins. A rarer cause is Budd-Chiari Syndrome, where a blood clot physically blocks the veins draining the liver. This leads to a sudden, painful enlargement of the liver.
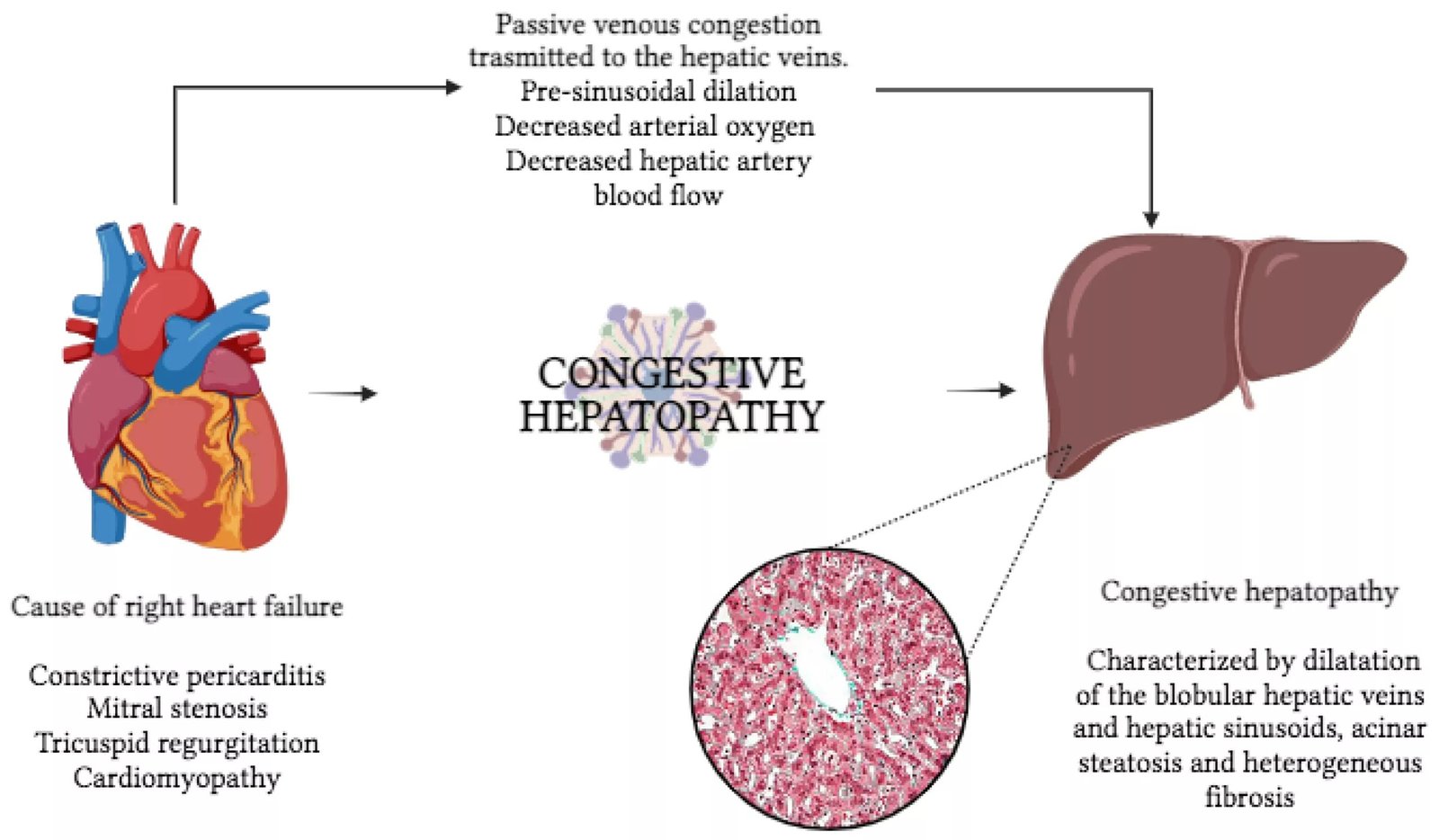
When the right side of the heart (RHF) is unable to pump efficiently, blood “backs up” through the venous system and into the liver. This passive congestion causes the liver to become engorged, heavy, and tender, a condition known ascongestive hepatopathy. (Image Courtesy: Aspromonte, N., Fumarulo, I., Petrucci, L., Biferali, B., Liguori, A., Gasbarrini, A., Massetti, M., & Miele, L. (2023). The Liver in Heart Failure: From Biomarkers to Clinical Risk. International Journal of Molecular Sciences, 24(21), 15665. Available fromMDPIand licensed under CC by 4.0)
4. Space-Occupying Liver Lesions
Sometimes the liver tissue itself is fine, but the overall size increases because of a growth inside the liver. For example, a large cyst/abscess (often caused by bacteria or parasites) can cause localized hepatomegaly. Similarly, liver cancer can also cause significant liver enlargement.
Symptoms of an Enlarged Liver
One of the most frustrating aspects of hepatomegaly is that it is often silent. Because the liver itself does not have many pain-sensing nerves, you may not feel the organ swelling until it begins to push against the surrounding capsule or neighboring organs like the stomach.
As the enlargement progresses, you may notice:
- Right upper quadrant discomfort as a dull ache or fullness just under the right rib cage. Unlike a sharp muscle strain, this pain is often persistent and may worsen when you lean forward.
- A significantly enlarged liver can press against the stomach wall. This makes you feel full after eating only a small amount of food.
- A constant feeling of fatigue. This is the most common systemic symptom.
- Nausea, also accompanied by a loss of appetite.
Signs of Advanced Liver Stress
In cases of advanced hepatomegaly, we also see physical signs:
- Jaundice: yellowing of the skin and the whites (sclera) of the eyes
- Abdominal distension (ascites)
- Dark colored urine and pale stools
- Pruritus (itching)
Diagnosis of Hepatomegaly
In minor, silent cases, the diagnosis is usually incidental, something found while imaging the body for a different reason. However, if symptoms are present, we use a combination of tools to decode the problem.
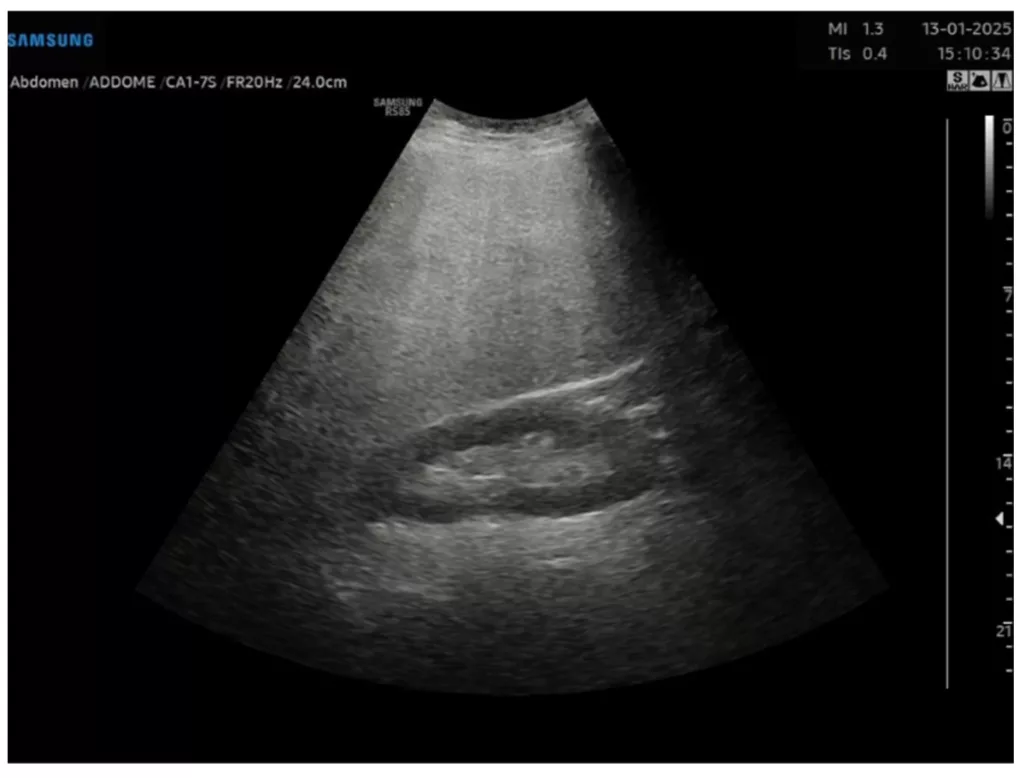
Advanced Metabolic Dysfunction (MASLD).This ultrasound scan of a 46-year-old male shows “Grade III” or severe steatosis. Notice the “bright” liver; this is a classic diagnostic sign of a liver overloaded with fat due to underlying metabolic conditions like Type 2 Diabetes and hypertension. (Image Courtesy: Ibba, F., Airola, C., Rozera, T., Petrucci, L., Carlino, G., Varca, S., Cavallaro, C., De Matthaeis, N., & Pizzolante, F. (2025) Clinical Value of Ultrasound Fat Fraction in Grading Hepatic Steatosis: Preliminary Cut-Off Values in Obese Patients. Gastroenterology Insights, 16(4), 47. Available fromMDPIand licensed under CC by 4.0)
Abdominal Ultrasound
If a physical exam suggests an enlargement, the next step is almost always an abdominal ultrasound. It is fast, non-invasive, and gives us the topography of the liver. Common ultrasound findings are:
| Finding | What it Means | Clinical Significance |
|---|---|---|
| Echogenic Liver5Al Salam H, Knipe H, Bell D, et al. Echogenic liver. Reference article, Radiopaedia.org | The liver looks bright on ultrasound | Hallmark of steatosis because of the fat |
| Coarse echo texture | The liver looks grainy or uneven. | Suggests chronic inflammation or earlycirrhosis |
| Hepato-splenomegaly | Both liver and spleen are enlarged. | Often points toportal hypertensionor systemic infection |
| Dilated Hepatic Veins | The veins inside the liver (hepatic) are wide. | Suggests acongestivecause (heart failure) |
Blood Tests
Imaging shows us how the shape and size of the liver have changed; blood work tells us if there is a defect in the function of the liver.
- ALT & AST: These are enzymes inside liver cells. If the cells are inflamed or dying (from hepatitis or fat), these enzymes leak into the bloodstream. High levels indicate active liver cell death.
- ALP & GGT: Elevation of these values suggests a blockage in the bile ducts or a congestive cause.
- Albumin & INR: These show if the liver is actually working. If these are abnormal, the hepatomegaly is likely chronic and serious.
Progression and Complications
A common question we hear in the clinic is whether an enlarged liver will eventually return to its normal size. The answer depends entirely on the stage of the underlying pathology. If the stressor is not removed, the liver moves through three distinct phases.
Initially, the liver is simply heavy. This is the stage of Steatosis or acute inflammation. At this point, the organ is physically large, but the tissue is still elastic and functional. If you intervene here, the hepatomegaly is almost entirely reversible. However, if the swelling persists for years, the liver begins to replace its healthy functional cells with fibrous scar tissue to protect itself. This is Fibrosis. While the liver may still be enlarged at this stage, it starts to become firm or coarse on an ultrasound.
The final and most dangerous stage is Cirrhosis. In a paradox, the liver actually begins to shrink at this stage and can not filter blood any longer. This leads to portal hypertension, where blood pressure spikes in the veins connecting the digestive tract to the liver. This pressure is what causes the most severe complications of hepatomegaly:
- Ascites
- Esophageal Varices (bleeding veins in the throat)
- and Hepatic Encephalopathy (an altered state of consciousness due to toxin buildup)

The progression from simple fat accumulation (Steatosis) to permanent scarring (Cirrhosis) is the primary driver of chronic hepatomegaly. The microscopic insets show how triglyceride droplets eventually give way to dense fibrous tissue, physically altering the organ’s size and function.
How to Manage Hepatomegaly?
Because hepatomegaly is simply a symptom, the treatment is simply fixing the root cause. We don’t shrink the liver with a pill; we remove the underlying insult that is making it swell. Based on the cause, we have the following management strategies:
Reversing Fatty Liver (MASLD)
Fatty liver disease is the most common cause of mild hepatomegaly. The good news is that it is often reversible.
- Clinical data show that losing just 7% to 10% of your body weight can physically shrink the liver and clear the fat from the cells.
- Focus on resistance training, which pulls fat out of the liver to be used as muscle fuel.
- Focus on a low-glycemic diet to lower insulin levels. When insulin is high, the liver is in fat-storage mode. By lowering it, the liver can finally begin to burn its own fat stores.
Managing Inflammation and Congestion
- If an infection is the cause, we use targeted antivirals to stop the attack on the liver cells.
- If the enlargement is congestive (due to heart failure), we use diuretics to remove the excess fluid backing up into the liver. This drains the organ and returns it to a normal size.
- Be extremely careful with liver detox supplements. There are many herbs and supplements being advertised as being able to prevent or reverse liver damage that are totally unregulated and can instead cause drug-induced liver injury, actually making the enlargement worse.
Final Word
Of course, getting to know that you have an enlarged liver comes as a shock to most patients. However, hepatomegaly is usually a warning sign. It doesn’t mean you’re going to need a transplant; rather, it requires systematic investigation to rule out metabolic stress, infection, or heart issues.
In most instances, an enlarged liver gives us an opportunity. It gives you the chance to fix metabolic health or address an infection before the injury becomes permanent. So, if your ultrasound incidentally shows an enlarged liver, take the report seriously, follow up with your doctor, and remember that the liver is one of the most resilient, forgiving organs in your body if you give it the right environment to heal.
References
[1] Jones J, Walizai T, Sharma R, et al. Hepatomegaly. Reference article, Radiopaedia.org
[2] Chan, W. K., Chuah, K. H., Rajaram, R. B., Lim, L. L., Ratnasingam, J., & Vethakkan, S. R. (2023). Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A State-of-the-Art Review. Journal of obesity & metabolic syndrome, 32(3), 197–213.
[3] David, S., & Hamilton, J. P. (2010). Drug-induced Liver Injury. US gastroenterology & hepatology review, 6, 73–80.
[4] Kozielewicz, D. M., Sikorska, K., & Stalke, P. (2021). Liver abscesses – from diagnosis to treatment. Clinical and Experimental Hepatology, 7(4), 329–336.
[5] Al Salam H, Knipe H, Bell D, et al. Echogenic liver. Reference article, Radiopaedia.org
[6] Wazir, H., Abid, M., Essani, B., Saeed, H., Ahmad Khan, M., Nasrullah, F., Qadeer, U., Khalid, A., Varrassi, G., Muzammil, M. A., Maryam, A., Syed, A. R. S., Shah, A. A., Kinger, S., & Ullah, F. (2023). Diagnosis and Treatment of Liver Disease: Current Trends and Future Directions. Cureus, 15(12), e49920.
[7] Armandi, A., & Schattenberg, J. M. (2021). Beyond the Paradigm of Weight Loss in Non-Alcoholic Fatty Liver Disease: From Pathophysiology to Novel Dietary Approaches. Nutrients, 13(6), 1977.
[8] Alevroudis, I., Kotoulas, S. C., Tzikas, S., & Vassilikos, V. (2023). Congestion in Heart Failure: From the Secret of a Mummy to Today’s Novel Diagnostic and Therapeutic Approaches: A Comprehensive Review. Journal of clinical medicine, 13(1), 12.