
{kind=link}

What is Hypochondroplasia?: Hypochondroplasia Short Limb
Hypochondroplasia Short Limb Hypochondroplasia is a rare short-limb dwarfism associated with mutations in the fibroblast growth factor receptor 3 (FGFR3) gene. It is a type of endochondral dysplasia, meaning that the normal process of replacing cartilage with bone during growth is impaired, particularly in the long bones. This disruption leads to proportionally shortened limbs, while the trunk is usually near normal in length. The features are often subtle at birth and become more noticeable in early childhood, with affected children gradually developing disproportionate stature, shortened arms and legs, and broad hands and feet. Unlike achondroplasia, facial features are typically mild, and many infants may initially appear normal.
The condition has been approximated to be found in approximately 1/15000-40000 births; therefore, it is not as prevalent as achondroplasia.[1]
Causes of Hypochondroplasia
Hypochondroplasia is a genetic disorder that is caused by activating mutations in the FGFR3 gene, which disrupts normal bone growth. Pathogenic variants of the FGFR3 gene in chromosome 4p16.3 cause the disease. FGFR3 codes for a receptor protein that regulates bone and cartilage formation through endochondral ossification. These gain-of-function mutations lead to overactivity of FGFR3. This overactivity inhibits the growth and differentiation of chondrocytes in the growth plate, thus leading to the shortening of long bones. Approximately twenty FGFR3 mutations are known. All cause milder effects than those in achondroplasia.[2]
Hypochondroplasia follows autosomal dominant inheritance. One mutated FGFR3 copy serves a 50% risk if a parent is affected. However, 80-90% of cases are de novo (sporadic, new mutations not inherited).[3]
A small minority lacks identifiable FGFR3 mutations. It may be due to variants in unidentified genes or undetected regulatory changes in FGFR3, a phenomenon termed genetic heterogeneity. No environmental or lifestyle factors contribute. In these cases, the causes are purely genetic and unpredictable.
Symptoms of Hypochondroplasia
Presentation of the disease is deceptive. By age 2-5 years, children exhibit a disproportionate short stature.
Core skeletal symptoms include:[4]
- Rhizomelia/Mesomelia: Patients present with short upper arms and thighs, milder than those of achondroplasia.
- Brachydactyly: Patients present with short, broad fingers and toes.
- Macrocephaly: Mild macrocephaly or relative frontal bossing may occur, but often the features are subtle.
- Lordosis/scoliosis: Patient presents with an exaggerated lumbar curve due to short legs.
Other physical traits may include:
- Joint laxity
- Broad trunk
- Short neck
- Bowed legs
Neurological and cognitive issues can also occur uncommonly, and symptoms may include:[5]
- Mild intellectual disability may occur in rare cases
- Temporal lobe epilepsy is also rare
- Obstructive sleep apnea
Less common symptoms are:
- Acanthosis nigricans (reported but uncommon)[6]
- Obesity predisposition
- Foramen magnum stenosis is rare and usually mild
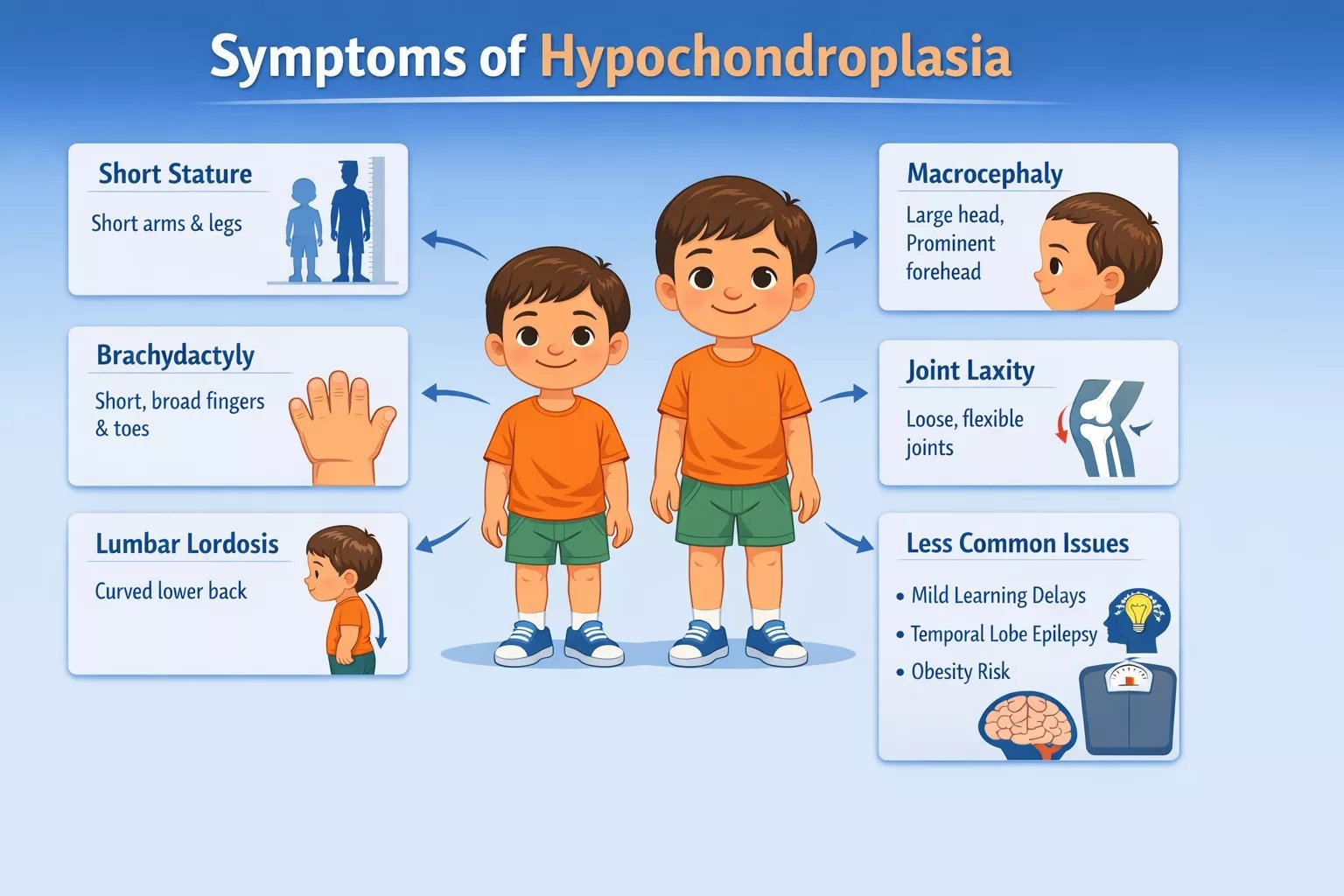
Illustration showing key physical features of hypochondroplasia in a child
Hypochondroplasia Diagnosis
Diagnosis combines clinical exam, radiology, and genetics. No single test suffices due to overlap with achondroplasia or idiopathic short stature.
Clinical Evaluation
Clinical evaluation involves the following steps:
Height Velocity Plots
Height velocity measures growth rate in cm per year, plotted on standardized over serial measurements. In hypochondroplasia, infants often have normal birth length and early growth, but after infancy, growth velocity decelerates sharply. This signals FGFR3-related impairment in endochondral ossification.
Anthropometry Details
Anthropometry is an exact body measurement. They apply standardized measurements, including stadiometers, tape measures, and callipers, and compare them with age- or sex-specific references.[7]
Family History Assessment
Clinicians review the family history to look for an autosomal dominant pattern. They ask whether parents or relatives have short stature, shortened limbs, or a known diagnosis of skeletal dysplasia. Family heights may be plotted using mid-parental height charts to assess inheritance patterns. Although many cases occur due to new (de novo) mutations and lack a family history, subtle findings in previous generations or consanguinity may still be relevant. Genetic counselling is recommended when hereditary features are identified.[8]
Radiographic Findings
Radiographic findings reveal:
- Short long bones with metaphyseal flaring and a narrowed lumbar interpedicular distance (mild flaring, less pronounced than in achondroplasia)
- Short pedicles, posterior vertebral scalloping, squared ilia, horizontal acetabular roof, short, broad femoral necks.
Molecular Confirmation
Molecular confirmation includes:
- FGFR3 sequencing detects mutations.
- Prenatal amniocentesis if family history or ultrasound flags.
Differential Diagnosis
Differential diagnosis include:
- Pseudoachondroplasia – Normal face but progressive short stature with loose joints and early joint problems.
- Turner syndrome – Short stature in females with neck webbing and heart defects, without limb disproportion.
Hypochondroplasia should be distinguished from other causes of short stature, particularly achondroplasia. Detailed differences between hypochondroplasia and achondroplasia are discussed below:
Hypochondroplasia Vs Achondroplasia
Both skeletal dysplasias associated with FGFR3 include achondroplasia and hypochondroplasia that cause the short limb dwarfism. Hypochondroplasia is, however, mild, with a later onset, and is not so complicated.
| Features | Hypochondroplasia | Achondroplasia |
|---|---|---|
| Severity | – Mild features; subtle until the age of two. | – Severe and evident at birth. |
| Clinical Features | – Joint laxity– Genu varum often self-resolves– Higher risk of mild Intellectual disability– Temporal epilepsy | – Trident hands– Foramen magnum stenosis– Hydrocephalus– Severe sleep apnea |
| Radiographic Distinctions | – Narrowed lumbar interpedicular distance– Mild metaphyseal flaring– Squared ilia | – Progressive widening– Tombstone vertebrae– Champagne glass femurs |
Complications
Though milder, complications arise, warranting monitoring. Orthopaedic complications include:
- Tibial bowing that self-resolves often
- Spinal stenosis
- Osteoarthritis (occurs due to joint stress)
The respiratory complications can be mild obstructive sleep apnea and frequent otitis media. There can be neurologic complications like epilepsy and hydrocephalus (infrequently). Some other complications can include delayed puberty in some patients and an increased risk from reduced activity.
Management and Treatment of Hypochondroplasia
There is no cure; management is supportive and symptom-focused.
Growth Hormone Therapy
Its use is still controversial and off-label. Some trials show 5-10 cm gain but variable response due to FGFR3 resistance. FDA approves GH off-label for hypochondroplasia. No serious adverse events reported, though monitoring for glucose intolerance or scoliosis is needed.[9]
Limb-Lengthening Surgery
This elective, invasive procedure uses distraction osteogenesis to elongate bones. It is reserved for severe disproportion impacting function or quality of life. Risks include infection, nerve injury, non-union, and joint contractures. Complications can be higher in multi-segment approaches, requiring multidisciplinary rehab. It is usually performed after skeletal maturity and improves body proportions, but it demands psychological readiness. Outcomes show functional gains, but trunk-limb mismatch may remain.[10]

Photographs of a female patient at age 13 (left) and age 17 (right) standing beside her mother. Following two adolescent-onset, two-segment lower-limb lengthenings totaling 10.25″ (26 cm), her height increased from 4′ (122 cm) to 5′1.5″ (156 cm). She also underwent 10 cm of humeral lengthening. Image courtesy: Extensive Limb Lengthening for Achondroplasia and Hypochondroplasia by Paley, 2021, doi.org/10.3390/children8070540, available via:MDPIunder license CC BY 4.0.
Orthopaedic Interventions
They target limb deformities and spinal complications.
- Bracing addresses tibial bowing
- Osteotomies for persistent genu varum
- Spinal decompression if stenosis is symptomatic
Multidisciplinary Care
Management of Neurological symptoms includes a multidisciplinary approach for hypochondroplasia that integrates physical therapy, nutrition, and psychological support. It will optimize function, prevent complications, and enhance quality of life.
Physical Therapy
Physical therapy is aimed at eliminating ligamentous laxity in the knees, hips, and elbows. Stability is achieved through strengthening exercises. Preventing contractures through proprioceptive training and range-of-motion stretches. Aquatic therapy is best for low-impact joint decompression. There are such goals as gait efficiency, lordosis, core stability, and endurance.
Dietary Support
Nutritional counselling is used to reverse the threat of obesity. Low-glycemic foods are useful for maintaining lean mass during growth spurts. Supplementation with calcium and vitamin D is beneficial for bone health in cases of dysplasia.
Psychological Support
Counselling is done in response to matters of self-esteem that can be caused by short stature stigma, bullying, or identity problems. The support options are cognitive-behavioural therapy (CBT) or family sessions since the diagnosis. In young people, the issue of body image is discussed using body image workshops to address transition concerns. The results are enhanced self-efficacy and long-term support to help the patient stabilize, empower themselves, and minimize isolation.
Prognosis and Expectancy of Life
Prognosis is good overall. Patients can enjoy a normal lifespan provided they are complication-free. The majority of them live independently, and their fertility is unaffected. Cognitive problems, if they occur, are responsive to early intervention and frequent screening, which may help alleviate orthopaedic/neurological risks.[11]
A Quick Review
Hypochondroplasia is a manageable skeletal dysplasia with generally good long-term outcomes. The affected people usually gain normal life expectancy, fertility, and independence. Clinical, radiographic, and genetic evaluation helps in making a diagnosis before complications like spinal stenosis or obesity develop. On the other hand, orthopaedic interventions and promotion of growth (GH therapy) improve function.
References
[1] Oehrlein, E. M., Pekala, R., Cavallaro, S., Cho, M., Crews, C., Dauber, A., … & Reese, E. S. (2025). Living With Hypochondroplasia: A Qualitative Exploration of Children’s and Caregivers’ Experiences, Challenges, and Unmet Needs.Molecular Genetics & Genomic Medicine,13(11), e70151.
[2] Chen, J., Yang, J., Zhao, S., Ying, H., Li, G., & Xu, C. (2018). Identification of a novel mutation in the FGFR3 gene in a Chinese family with Hypochondroplasia.Gene,641, 355-360.
[3] Doherty, M. A., Hertel, N. T., Hove, H. B., & Haagerup, A. (2017). Neurological symptoms, evaluation and treatment in Danish patients with achondroplasia and hypochondroplasia.Journal of Rare Diseases Research & Treatment,2(4), 25-32.
[4] Bober MB, Bellus GA, Cheung MS, Jain M, Nikkel SM, Tiller GE. Hypochondroplasia. In: Adam MP, Bick D, Mirzaa GM, et al., editors.GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993‑2025.
[5] Genomics Education Programme. Hypochondroplasia Knowledge Hub [Internet].
[6] Soto‑García D, Batalla A, Oro‑Ayude M, Flórez Á. Acanthosis Nigricans and Hypochondroplasia Associated with FGFR3 Mutation: A Case Report.Indian J Dermatol. 2023;68(3):333–334
[7] Nakano, Y., Kubota, T., Ohata, Y., Takeyari, S., Kitaoka, T., Miyoshi, Y., & Ozono, K. (2023). Assessment of body fat mass, anthropometric measurement and cardiometabolic risk in children and adolescents with achondroplasia and hypochondroplasia.Endocrine Journal,70(4), 435-443.
[8] Guo, R., Haldeman-Englert, C. R., Akilapa, R., Irving, M., Holder-Espinasse, M., Mulle, J. G., … & van der Sluijs, P. J. (1993). GeneReviews®.
[9] Massart, F., Miccoli, M., Baggiani, A., & Bertelloni, S. (2015). Height outcome of short children with hypochondroplasia after recombinant human growth hormone treatment: a meta-analysis.Pharmacogenomics,16(17), 1965-1973.
[10] Paley, D. (2021). Extensive limb lengthening for achondroplasia and hypochondroplasia.Children,8(7), 540.
[11] dam MP, Bick D, Mirzaa GM, et al., editors.Hypochondroplasia. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1999‑2026. PMID: 20301650.