
{kind=link}

pancreatic cancer genetics Pancreatic cancer is called a silent killer in clinical circles because it is very rarely detected in its early stages, where it could have been most treatable. It’s often described as one of the most formidable challenges in modern oncology. Similar to a lot of cancers, one of the biggest questions patients have after receiving the diagnosis is, “Is this in my genes? Are my children at risk?”
As medical professionals, we are seeing a shift in how we answer this. Until recently, with most cases turning out to be sporadic (due to accumulated DNA damage over time), we believed that genetics was less of a factor than we now realize. We know that even in people with certain inherited gene defects, smoking multiplies the risk approximately two- to threefold. Other lifestyle factors like chronic pancreatitis, obesity, and long-standing type 2 diabetes can also exacerbate this genetic fault.
The Global Burden: pancreatic cancer genetics
To understand the risk, we must first look at the scale of the problem. Globally, pancreatic cancer is the 12th most common cancer, but it ranks as the third leading cause of cancer-related deaths in many high-income nations.
As reported by the World Health Organization (WHO), new cases diagnosed each year are as high as 500,000. For 2026, it is estimated that approximately 67,500 people will be diagnosed in the U.S. alone, with nearly 52,000 predicted to die from the disease. Since the five-year survival rate is barely 11-13%, the mortality rate is nearly as high as the incidence.
At a time when mortality for many cancers is dropping because of earlier screening and newer treatment options, pancreatic cancer deaths continue to rise. In fact, it is on track to become the second biggest cause of cancer death by 2030.
Sporadic vs. Hereditary Pancreatic Cancer
The development of any cancer is essentially a series of genetic accidents. However, there is a distinct difference between having “genetic” cancer and “hereditary” cancer:
- Sporadic (90%): Most pancreatic cancers are caused by acquired mutations. These are DNA errors that occur during your lifetime due to aging, tobacco use, or chronic inflammation. Somatic mutations are only found in the tumor itself and cannot be passed down to your children.
- Hereditary (10%): About 1 in 10 patients with pancreatic cancer carries a germline mutation. These are inherited genetic faults from a parent that are present in every cell of the body, significantly lowering the threshold for cancer to develop.
When Should You Suspect a Hereditary Link?
In the clinic, we don’t just look at the pancreas; we look at the whole family tree. We suspect a hereditary component when we see:
- Families with two or more first-degree relatives (parents, siblings, or children) or a combination of first- and second-degree relatives diagnosed with the disease.
- A diagnosis before age 50 is a major red flag.
- Because many of the genes are not pancreas-only, but are involved in other malignancies as well, clinicians have to consider a multi-cancer cluster: a family history of breast, ovarian, colon, or skin cancer (melanoma) can actually point toward a pancreatic risk.
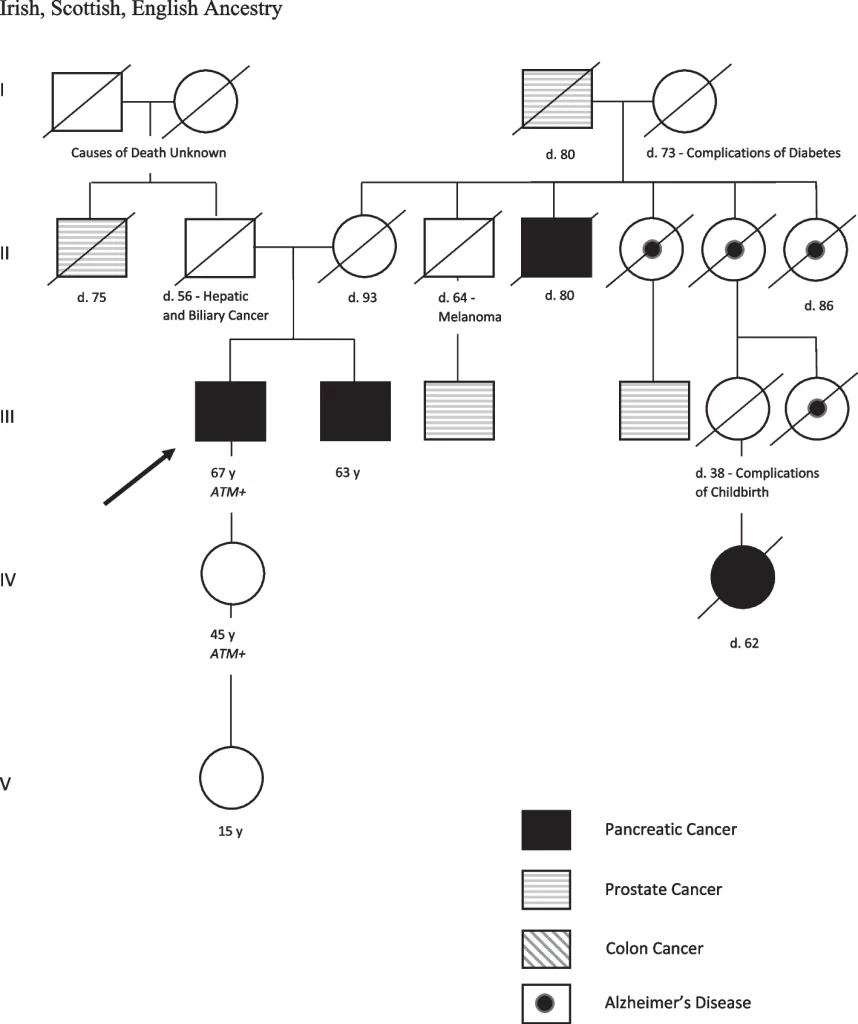
Pedigree Analysis of Familial Pancreatic Cancer: This three-generation pedigree illustrates a strong maternal predisposition to malignancy. Key features include multiple cases of Pancreatic Cancer (PC) and Prostate Cancer, appearing across first and second-degree relatives. Such a multi-cancer cluster often indicates a shared underlying germline mutation, such as BRCA2. (Image Courtesy: Lowe, T., DeLuca, J., Abenavoli, L. et al. Familial pancreatic cancer: a case study and review of the psychosocial effects of diagnoses on families. Hered Cancer Clin Pract 21, 17 (2023). Available fromSpringerand licensed under CC by 4.0)
The Key Genetic Players
Doctors used to look at these as literally separate organ genes and believed that BRCA mutations were just a breast cancer problem, but we now understand they are part of a broader failure in the body’s DNA repair machinery. Most hereditary pancreatic cancers are caused by mutations in tumor suppressor genes.
In a healthy body, these genes act like biological check-points, identifying and fixing errors in our DNA. When these are mutated from birth, cancer cells can grow unchecked.
| Hereditary Gene Mutation | Associated Cancer Risks (Primary) | Approximate Lifetime Risk of Pancreatic Cancer | Key Characteristics |
|---|---|---|---|
| Familial Pancreatic Cancer | Pancreatic cancer (multiple family members) | 10-20% (depending on the number of affected relatives) | Defined by ≥ 2 first-degree relatives with pancreatic cancer6Petersen G. M. (2016). Familial pancreatic cancer. Seminars in oncology, 43(5), 548–553. |
| BRCA1, BRCA2 | Breast, Ovarian, Prostate, Skin cancer (Melanoma) | BRCA2: ~5–10%; BRCA1: ~2–3% | Most common cause of inherited pancreatic cancer |
| PALB2 | Breast, Ovarian | 5-10% | Often works in conjunction with BRCA2 |
| CDKN2A (p16) | Melanoma (FAMMM Syndrome) | 10-20% | High risk, also linked to other cancers |
| STK11 | Peutz-Jeghers Syndrome7Sherman S, Menon G, Krishnamurthy K. Peutz-Jeghers Syndrome. [Updated 2025 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535357/(GI polyps, breast) | 30-40% | Syndrome itself is very rare, but it has a high risk for pancreatic cancer |
| Lynch Syndrome(MLH1, MSH2, MSH6, PMS2) | Colorectal, Endometrial, Ovarian cancer | 1-5% | Also increases risk for gastric, urinary tract, and bile duct cancers |
| ATM | Breast, Prostate | 1-5% | Role in DNA repair, emerging as a risk factor |
| PRSS1/SPINK1 | Hereditary Pancreatitis | ~40-50% (if chronic pancreatitis develops) | Directly causes chronic pancreatitis, which is a major risk factor for cancer |
Modifiable Risk Factors
For individuals with a known mutation, the genetic risk is always present, but the trigger itself is their lifestyle. This is what we call the Two-Hit Hypothesis: you are born with the first hit (the gene defect), but cancer usually requires a second hit (environment) to begin.
- For a BRCA2 carrier, smoking multiplies the risk. Basically, carcinogens damage DNA, and the repair gene that could have otherwise fixed that damage is broken itself.
- Several metabolic disorders have the potential to cause chronic inflammation in the pancreas. Cells exposed to inflammation long-term can turn cancerous in a person genetically at risk. Obesity and Type 2 Diabetes are examples of this.
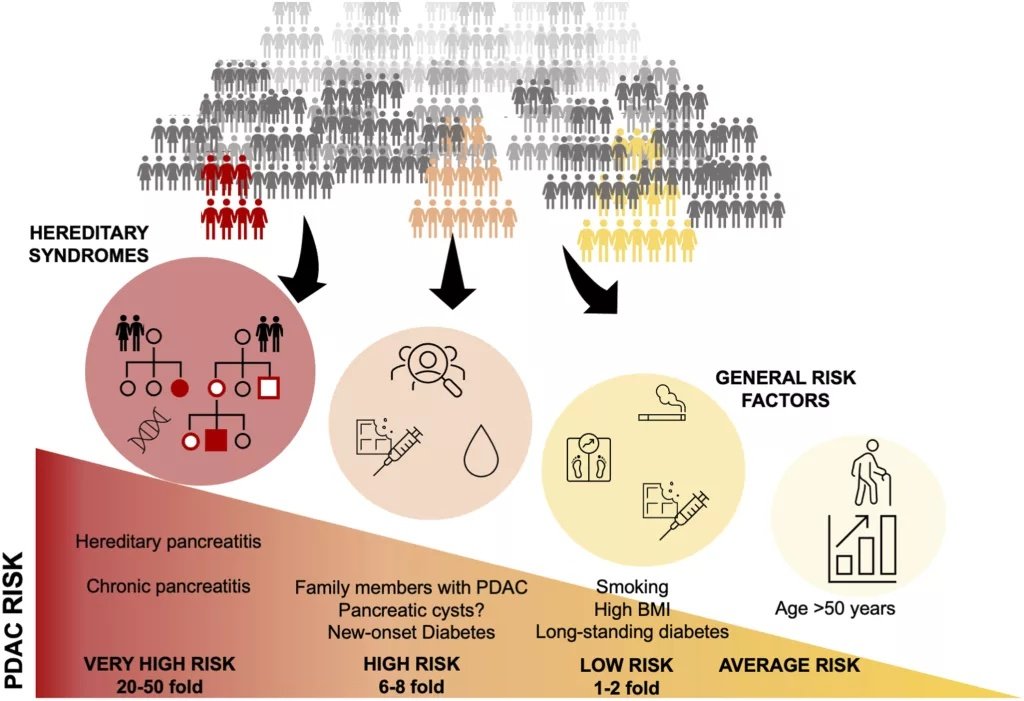
The spectrum of pancreatic cancer (PDAC) risk. While rare genetic syndromes carry the highest individual risk (up to 50-fold), common factors like smoking and age affect the largest portion of the population. (Image Courtesy: Søreide, K., Ismail, W., Roalsø, M., Ghotbi, J., & Zaharia, C. (2023). Early Diagnosis of Pancreatic Cancer: Clinical Premonitions, Timely Precursor Detection and Increased Curative-Intent Surgery. Cancer Control. Available fromSageJournalsand licensed under CC by 4.0)
Warning Signs and Symptoms of Pancreatic Cancer
Pancreatic cancer often progresses silently, and early-stage disease rarely causes noticeable symptoms. When symptoms do appear, they are usually a sign of advanced disease and may be vague or easily overlooked.
Common warning signs include:
- Painless jaundice with dark urine and pale stools
- Unexplained weight loss and loss of appetite
- Persistent upper abdominal pain radiating to the back
- New-onset diabetes or sudden worsening of previously stable diabetes
- Fatigue, nausea, or digestive discomfort
Because these symptoms are nonspecific and often appear late, they are not reliable for early detection, reinforcing the importance of genetic risk assessment and surveillance in high-risk individuals.
Diagnosis & Screening Opportunities
There is no one pathognomonic test (like a PSA for prostate cancer) that can detect pancreatic cancer in the general population. However, for individuals at high risk, we use an established surveillance-based strategy on the International Cancer of the Pancreas Screening (CAPS) protocol.
Genetic Counseling
Before any blood work, we map the family tree and determine if testing is appropriate. Testing usually involves a simple blood or saliva sample to look for mutations in the genes listed above.
Annual Imaging
For high-risk individuals, annual screening starts at age 50. Another criterion in practice is to screen 10 years earlier than the youngest diagnosis in the family, with earlier initiation (around age 40) recommended for certain syndromes such as Peutz-Jeghers. We rely on two primary tools:
- Endoscopic Ultrasound (EUS): A gastroenterologist passes a thin, flexible tube into the stomach. A tiny ultrasound probe at the tip provides high-resolution images of the pancreas from just inches away.
- MRI/MRCP: This specialized MRI looks at the pancreatic ducts to find pre-cancerous lesions before they turn invasive.
The Role of CA 19-9
CA 19-9 is a tumor marker we use to monitor how a patient is responding to treatment, but it is not a reliable screening tool because gallstones or jaundice can cause false positives.
Treatment for Pancreatic Cancer
The good thing about identifying a hereditary link is that it changes how we treat the disease. We are moving away from a one-size-fits-all approach of traditional chemotherapy, towards precision medicine.
Patients with BRCA1, BRCA2, or PALB2 mutations have a specific flaw at a molecular level: they cannot easily repair damage to their own DNA. We use this weakness against them through two primary methods:
Platinum-based Chemotherapy
- Drugs like Cisplatin or Oxaliplatin work by physically creating breaks in the DNA of cancer cells. Because the gene in charge of fixing this is defective or missing, it cannot fix these breaks and goes through programmed cell death.
PARP Inhibitors
- These are a newer class of oral medications that block backup DNA repair pathways, leading to synthetic lethality in the cancer cells. The cells have multiple ways to fix DNA: one uses the BRCA gene, and another uses an enzyme called PARP.
- In a BRCA-mutated patient, the cancer has already lost the first repair method. By giving a PARP Inhibitor, we block the second repair method.
- This creates synthetic lethality, a state where the cancer cell is deprived of all its backup plans for survival. It dies because it can no longer maintain its genetic code, while the healthy cells (which have at least one functional repair pathway) remain largely unharmed.
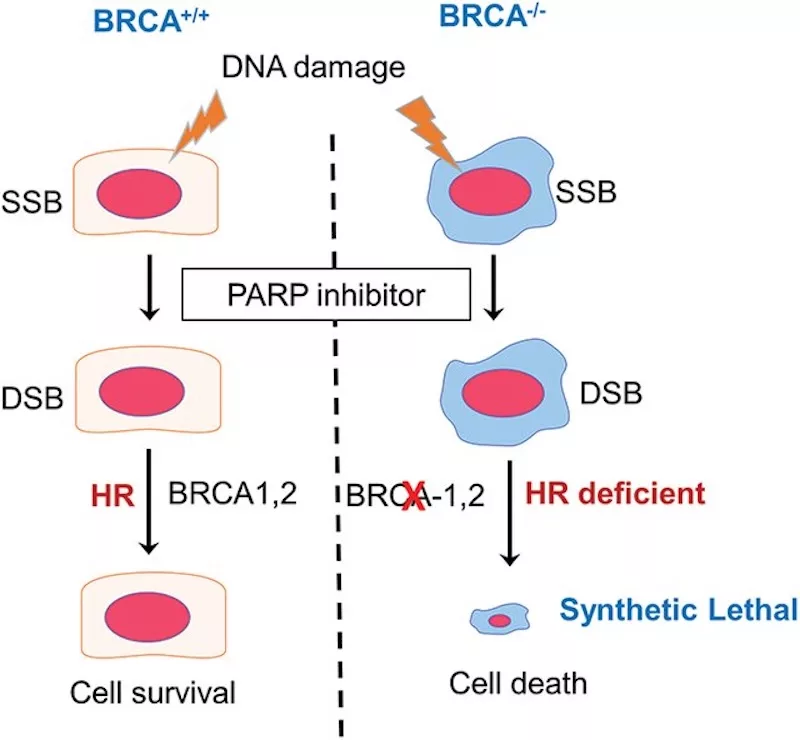
PARP inhibitors block the repair of single-strand DNA breaks, which then convert into more severe double-strand breaks during cell replication. While healthy cells utilize the BRCA gene to repair this damage, BRCA-mutant cancer cells lack this “backup” system, leading to targeted cell death through the mechanism of synthetic lethality. (Image Courtesy: NAMBIAR, D.K., MISHRA, D., SINGH, R.P. (2023). Targeting DNA repair for cancer treatment: Lessons from PARP inhibitor trials. Oncology Research, 31(4), 405–421. Available fromResearch Gateand licensed under CC by 4.0)
Final Word
In all the years that we’ve been trying to find a cure for cancer, one lesson has remained constant at every stage: the best time to treat a cancer is before it becomes one. While you cannot change your genes, knowing your genetic status allows for early detection and ultimately, a better chance at survival.
If you have a family history of pancreatic cancer or multiple cases of breast and colon cancer, talk to your physician. We now have the tools to go hunting for the disease while it is still small enough to be defeated. Genetic risk assessment is the only way to stay one step ahead of the silent killer.
References
[1] Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians, 71(3), 209-249.
[2] Ferlay J, Colombet M and Bray F. Cancer Incidence in Five Continents, CI5plus: IARC CancerBase No. 9. [cited 7 Feb 2022]. In: International Agency for Research on Cancer [Internet]. Available from: http://ci5.iarc.fr.
[3] Siegel, R. L., Kratzer, T. B., Wagle, N. S., Sung, H., & Jemal, A. (2026). Cancer statistics, 2026. CA: a cancer journal for clinicians, 76(1), e70043.
[4] Stoffel, E. M., Brand, R. E., & Goggins, M. (2023). Pancreatic Cancer: Changing Epidemiology and New Approaches to Risk Assessment, Early Detection, and Prevention. Gastroenterology, 164(5), 752.
[5] Jacobs, E. J., Chanock, S. J., Fuchs, C. S., Lacroix, A., McWilliams, R. R., Steplowski, E., Stolzenberg-Solomon, R. Z., Arslan, A. A., Bueno-de-Mesquita, H. B., Gross, M., Helzlsouer, K., Petersen, G., Zheng, W., Agalliu, I., Allen, N. E., Amundadottir, L., Boutron-Ruault, M. C., Buring, J. E., Canzian, F., Clipp, S., … Zeleniuch-Jacquotte, A. (2010). Family history of cancer and risk of pancreatic cancer: a pooled analysis from the Pancreatic Cancer Cohort Consortium (PanScan). International journal of cancer, 127(6), 1421–1428.
[6] Petersen G. M. (2016). Familial pancreatic cancer. Seminars in oncology, 43(5), 548–553.
[7] Sherman S, Menon G, Krishnamurthy K. Peutz-Jeghers Syndrome. [Updated 2025 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535357/
[8] Pandol, S. J., Apte, M. V., Wilson, J. S., Gukovskaya, A. S., & Edderkaoui, M. (2012). The Burning Question: Why is Smoking a Risk Factor for Pancreatic Cancer? Pancreatology : Official Journal of the International Association of Pancreatology (IAP) … [et al.], 12(4), 344.
[9] Pothuraju, R., Rachagani, S., Junker, W. M., Chaudhary, S., Saraswathi, V., Kaur, S., & Batra, S. K. (2018). Pancreatic cancer associated with obesity and diabetes: an alternative approach for its targeting. Journal of experimental & clinical cancer research : CR, 37(1), 319.
[10] Canto MI, Harinck F, Hruban RH, et alInternational Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancerGut 2013;62:339-347.
[11] Brown, T. J., & Reiss, K. A. (2021). PARP Inhibitors in Pancreatic Cancer. Cancer journal (Sudbury, Mass.), 27(6), 465–475.