
{kind=link}

What are Keloid Scars?: Keloid Scars They
Keloid Scars They A ‘Keloid scar’ is “an unusually raised, firm, and thick scar that forms after surgery or an injury,” as described in Harvard’s medical dictionary.[1] It forms due to abnormal wound healing and excessive deposition of fibrous tissue that extends beyond the original wound margins into surrounding normal skin. Usually occurring between the ages of 10 to 30 years, Keloids have both cosmetic and functional challenges, limiting mobility if present near joints. Due to its high recurrence rate, the treatment remains challenging, ranging from topical steroids to cryotherapy, radiotherapy, or surgical excision.[2]
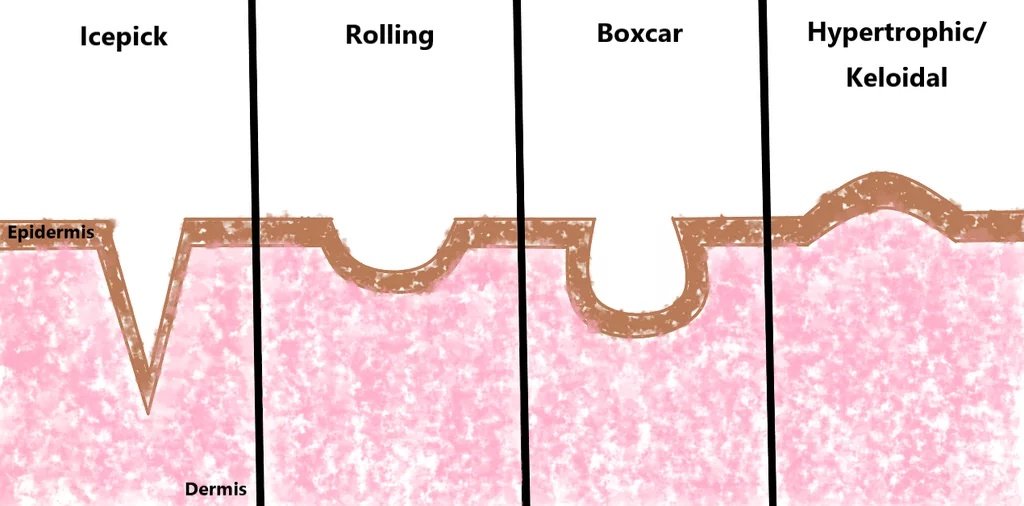
Diagram of acne scar classification showing major morphological scar types—atrophic (icepick, boxcar, rolling), hypertrophic, and keloid scars—with keloid scars represented as raised scars in contrast to other scar types. This image is sourced fromWikimedia Commonsunder a Creative Commons Attribution‑ShareAlike 4.0 International license, illustrating the morphological classification of acne scars, including icepick, boxcar, rolling, hypertrophic scars, and keloids
What do Keloid Scars look like?
A keloid scar is a raised, lumpy growth that slowly grows beyond the margins of the original wound. They are thick, firm, and have an irregular appearance. The color of the raised scar varies from pink, red, to brown and darker colors depending on your skin color. The surface is hairless, smooth, and shiny.
You can feel discomfort in the scar, with a constant tender, sore, or itchy feeling. Occasionally, people experience a burning sensation under the skin. Depending on the location of the wound or scar, movement can become limited or uncomfortable, especially if it is present on a joint. Over time, keloids typically persist and may continue to enlarge, rather than fading or regressing, often requiring medical intervention.[3]

Hyperinflammatory chest wall keloid (“butterfly keloid”) demonstrating extensive raised, firm scar tissue extending beyond the boundaries of the original wound, characteristic of exaggerated fibroproliferative healing. This image is sourced fromWikimedia Commonsand is licensed under the Creative Commons Attribution-ShareAlike 3.0 Unported (CC BY-SA 3.0) license. Image credit:‘Keloid-Hyperinflammatory, Chest Wall Keloid, Butterfly Keloid’by James Heilman, MD.
How can you get a Keloid Scar?
Keloids usually occur due to abnormal healing of a wound or a skin injury. You can develop a keloid if you have:
1. Skin Injury or Trauma:
If your skin gets injured, and the wound penetrates into the deeper layers of your skin, it can be a trigger for keloid formation. This is due to increased inflammation and activated fibroblasts in the area. Skin injuries include:[4]
- Surgical incisions
- Accidental injuries (e.g., shaving cuts)
- Burns
- Ear or body piercings
- Tattoos
- Insect bites
- Injections
- Diseases such as acne, chickenpox, and folliculitis
2. Local Tissue Factors:
The location of the wound largely determines if it will turn into a keloid or not. Mechanical forces influence inflammation-driven pathalogical scarring of the wound.
You can experience keloid formation due to the following local causes:[5]
- Areas with high skin tension (e.g., neck, jaw, sternum): The shape of the keloid is based on the direction of the tension of the skin.
- Areas with repetitive movements (e.g., elbow and knee joints, shoulders): Repetitive movements, such as walking, moving your arms, etc., put force on the wound and cause the skin to stretch. This leads to increased inflammation, delayed healing, and a strong possibility of keloid formation.
- Repeated injury: Repetitive injury or infection on the same wound or scar can lead to excess collagen deposition, resulting in keloid formation.

Post-surgical keloid scar characterized by raised, firm, hyperpigmented scar tissue extending beyond the original wound margins, consistent with abnormal collagen overproduction following surgery. Keloid, Post Surgical” by James Heilman, MD, licensed under CC BY-SA 3.0, viaWikimedia Commons.
Who is most likely to get a Keloid Scar?
Keloid scars are dictated by several different factors that can be categorised as genetic, systemic, local, and lifestyle-related.
1. Genetic:6Sadiq A, Khumalo NP, Bayat A. Genetics of Keloid Scarring [Internet]. Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, editors. PubMed. Cham (CH): Springer; 2020.
- Race: If you have darkly pigmented skin, such as that of black people, you have the greatest risk of developing keloids. Followed by, if you are of Asian, Latin American, or Mediterranean descent.
- Family History: If anyone in your family has a keloid, you are likely to develop one too.
- Age: If you are in between 10-30 years old, you are more prone to developing a keloid.
2. Systemic:
- Pregnancy: The hormonal changes during pregnancy can increase your risk of keloids.
- Hypertension: High blood pressure has been associated with increased keloid severity in some studies. Hypertension causes damage to the blood vessels. In turn, it affects blood flow and contributes to inflammation and an abnormal cellular environment. This eventually promotes keloid development instead of normal healing of the wound.[6]
- Female gender: If you’re a female, fluctuations in hormonal levels can be a risk factor. Estrogen plays a role in widening the blood vessels (vasodilation) and also increases inflammation during the wound healing process.[7]
- Inflammatory cytokines: Increased levels of inflammatory cytokines can increase your risk of keloid formation. This is usually caused by diseases involving chronic inflammation, such as asthma, diabetes, and autoimmune diseases.[8]
3. Lifestyle risk factors:
- Continuous body movements (e.g., athletes, manual labour) cause tension in the wound or scar.
- Alcohol: Excess consumption of alcohol impairs wound healing by promoting inflammation.[9]
- Prolonged exposure to hot water can increase inflammation in the wound.
- Obesity: An increase in fatty tissue drives chronic inflammation.[10]
How does the scar develop?
To understand abnormal wound healing, we need to understand the normal wound healing process first. Normal wound healing occurs in three phases, and Abnormal wound healing in hypertrophic or keloid scars occurs due to changes in these stages.[11] [12]
| Phase | Normal wound healing | Abnormal wound healing (hypertrophic or keloid scars) |
|---|---|---|
| Inflammatory phase | Inflammatory molecules such as cytokines, prostaglandins, IL-6, IL-8, etc., cause vasodilation of the blood vessels. This consequently causes more immune cells (mast cells, macrophages, lymphocytes) to flow into the area to protect the wound from infection and microorganisms. The immune cells also release growth factors that play a crucial role in the next phase. | This phase is prolonged, causing the release of more inflammatory proteins and growth factors (such as TGF-beta, IL-6, IL-8), driving extra immune cells into the wound. |
| Proliferative phase | Fibroblasts (the main cells responsible for building structure in the body) increase in number to deposit collagen and fill the wound. This is regulated by transforming growth factor-beta (TGF-beta). New blood vessels also form in the wound, and new skin cells help in closing the wound. | The prolonged inflammatory phase drives fibroblast activation and increased collagen synthesis. Keloidal fibroblasts have increased proliferative activity and lower rates of cell death (apoptosis), leading to the overproduction of collagen and extracellular matrix components. |
| Remodeling phase | The new skin cells, blood vessels, and collagen are rearranged to look more like normal skin and less like a scar. | The prolonged activation of fibroblasts results in abnormal deposition of type 1 and 3 collagen. The scar is not remodeled to look closer to the skin; however, the scar is dense, hard, and raised. Consequently, it may continue to grow since the earlier phases go unchecked and unregulated. |
Common Sites for Keloid Scars
As discussed earlier, keloid scars usually develop in areas with repetitive movements or greater skin tension. These areas include:[13]
- The earlobe is a common region for keloid formation, often associated with piercings. There is also mechanical stress from continuous head movements throughout the day.
- Chest: The breastbone and upper chest are also common areas for growth because the skin in this area is subjected to high and frequent skin tension from everyday movements, such as arm motion and breathing.
- Shoulders: Frequently affected due to skin movement and tension.
- Head and Neck: The jaw, chin, and neck are areas where the skin is constantly under mechanical stress due to daily movements like talking, eating, and postural changes.
- Abdomen: In females who have delivered through a cesarean, their cesarean scar is prone to conversion into a keloid. Increased levels of estrogen, progesterone, and growth factors during pregnancy can promote fibroblast activity and collagen deposition into the scar, as discussed earlier.[14]
Hypertrophic Scar vs Keloid Scar
Although Hypertrophic and Keloid scars have many similarities, they are both different entities, and one should know the difference between them. They both form due to excess collagen deposition during abnormal wound healing, resulting in thick, raised scars. Additionally, they both develop after skin injury, and are tender to the touch or itchy.
However, hypertrophic scars (HS) remain confined to the margins of the original wound, but keloid scars extend beyond the margins of normal skin. HS forms within a short period of time (within weeks), and they often flatten over time, but keloids grow slowly (over months) and do not regress over time. Hypertrophic scars don’t have a genetic or ethnic predisposition, but keloids do. Hypertrophic scars are easier to treat, and in contrast, management of keloids can be challenging due to their high recurrence rate.
The table below summarizes their differences:
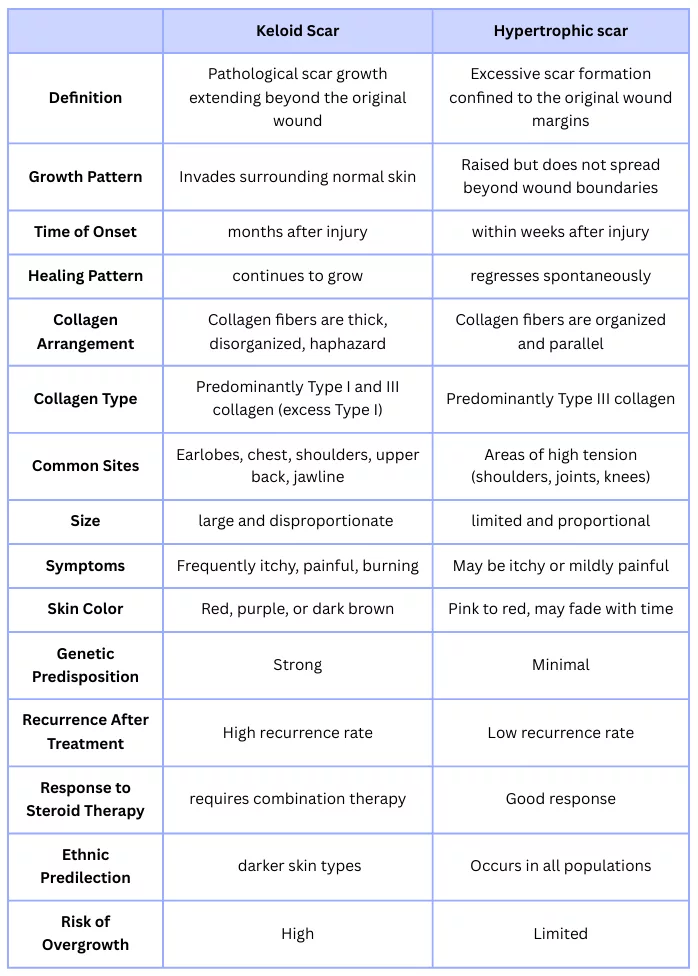
Comparison table highlighting the key clinical, histological, and behavioral differences between keloid scars and hypertrophic scars.

Hypertrophic scar on the forearm, observed four months after the inciting injury, showing raised, firm scar tissue confined within the original wound boundaries. This image is sourced fromWikimedia Commonsand is licensed under the Creative Commons Attribution-ShareAlike 3.0 Unported (CC BY-SA 3.0) license. Image credit: “Hypertrophic scar – 4 months after incident” by James Heilman, MD.
How can you treat or reduce the appearance of keloid scars?
Keloid scars can be treated either through non-invasive methods or invasive ones. Generally, your clinician may start with a non-invasive treatment and move on to invasive ones depending upon the response to the treatment.
Non-invasive or Conservative Treatments:
- Silicone dressings: They have been recommended as a first-line preventive and adjunctive therapy, particularly for early or immature scars. These silicone patches or gels help keep the scar or wound hydrated. It also prevents secondary or repeated trauma to the wound.[15]
- Pressure Therapy: Pressure on the scar or wound, in the form of custom clothing or tight bandages, helps in the prevention and treatment of Keloidal growths. The constant pressure constricts blood flow and causes hypoxia in the region. Consequently, less blood flow would result in less inflammation and less collagen deposition, decreasing the growth of the keloid.[16]
- Topical Corticosteroids: Help reduce inflammation and collagen deposition. Topical corticosteroid tape or patches can help reduce keloid height, redness, and fibroproliferative tissue, particularly in children or small lesions.
- Sun protection: Sun exposure increases melanin production, inflammation, and enzymes that regulate collagen synthesis. UV exposure slows healing and increases scar healing. Henceforth, you should keep the wound or scar covered from the sun and apply broad-spectrum SPF 30+ sunscreen, helping reduce the appearance of the keloid.

Scapular keloid in a 9-year-old boy before and after treatment with corticosteroid tape, demonstrating reduction in scar height, erythema, and fibroproliferative tissue following topical corticosteroid therapy.This image is sourced fromWikimedia Commonsand is licensed under the Creative Commons Attribution-ShareAlike 3.0 Unported (CC BY-SA 3.0) license. Image credit: “Effect of fludroxycortide tape on a scapular keloid of a 9-year-old boy” by James Heilman, MD.
Invasive or Surgical Treatments:
Intralesional corticosteroid injections:18Yin Q, Juliette M.I. Louter, Niessen FB, Gibbs S, Gizem Tasdemir-Kilic, Lapid O, et al. Intralesional Corticosteroid Administration in the Treatment of Keloids: A Scoping Review on Injection Methods. Dermatology. 2023 Jan 1;239(3):462–77.
This is a first-line invasive treatment of keloid scars. The most common agent used is triamcinolone acetonide (TAC). Corticosteroids have anti-inflammatory effects by constricting the blood vessels and decreasing the flow of inflammatory molecules. Additionally, it inhibits the proliferation of fibroblasts and slows down new collagen deposition. Your clinician will use a fine needle to insert the drug directly into the lesion. This therapy can be repeated every 4-6 weeks until the lesion has completely transgressed.
5-FU (5-Fluorouracil) injections:
These injections block DNA synthesis, inhibit fibroblast growth, and reduce collagen production, acting as a blood supply limiting agent.
Bleomycin injections:
Bleomycin is an anti-tumor agent that inhibits DNA synthesis, causing keratinocyte necrosis and fibroblast apoptosis.
Cryotherapy:19Barara M, Chander R, Mendiratta V. Cryotherapy in treatment of keloids: Evaluation of factors affecting treatment outcome. Journal of Cutaneous and Aesthetic Surgery [Internet]. 2012 [cited 2020 Jan 13];5(3):185.
Cryo means ‘to freeze’. Liquid Nitrogen is applied or injected into keloid scars. This freezes and destroys the tissue, and the abnormal cells die. This is an effective and commonly used treatment method for treating most bulky and thick keloids.
Laser Therapy:20Leszczynski R, da Silva CA, Pinto ACPN, Kuczynski U, da Silva EM. Laser therapy for treating hypertrophic and keloid scars. Cochrane Database of Systematic Reviews. 2022 Sep 26;2022(9).
Various lasers can be used in the treatment of keloids. Lasers help control inflammation via destruction of lesional blood vessels. The heat produced from the lasers helps to break down the excess deposition of collagen and fibrotic tissue, alleviating pain and discomfort. It also helps reduce its size and improve texture. Your clinician might use different types of lasers to treat the lesion, based on your presenting complaint.
- Pulsed Dye Laser (PDL): This laser targets blood vessels and is excellent for redness and itching, often combined with steroids.
- Nd: YAG Laser (Long-pulsed): This laser targets deep blood vessels, effective for thicker scars, sometimes used with fractional lasers or steroids.
- CO2 & Erbium Lasers: Used to vaporize scar tissue, often followed by steroid infusion.
- Fractional Lasers: Create micro-channels to stimulate collagen remodeling.
Radio-frequency or Combination Therapies:
Radiofrequency is an emerging adjunctive therapy that heats up the scar tissue and causes controlled denaturing of collagen and collagen breakdown. Multiple sessions (e.g., 3-8) are often needed, spaced about a week apart, depending on keloid size and response.
Surgical Excision:21Goutos I. Intralesional excision as a surgical strategy to manage keloid scars: what’s the evidence? Scars, Burns & Healing. 2019 Jan;5:205951311986729.
Your clinician might choose to surgically remove your keloid, but the recurrence rate is very high. Consequently, surgical excision is followed by a combination of other techniques (corticosteroid injections, pressure therapy, etc.)
Wrap Up
Keloid scars result from abnormal wound healing and can cause both cosmetic and functional issues. Treatment can be challenging because of their high recurrence rate, but a combination of preventive measures and targeted therapies, including silicone dressings, pressure therapy, intralesional corticosteroids, cryotherapy, and laser therapy, can help reduce scar size, symptoms, and discomfort. Early recognition, proper wound care, and individualized management are important for the best outcomes.
References
[1] Medical Dictionary of Health Terms: J-P – Harvard Health [Internet]. Harvard Health. 2011.
[2] Arya Tjipta Prananda, Rony Abdi Syahputra. Photobiomodulation therapy in keloid management: a comprehensive review. Frontiers in Medicine. 2025 Jul 9;12.
[3] Mayo Clinic. Keloid scar – Symptoms and causes [Internet]. Mayo Clinic. 2023.
[4] Mayo Clinic. Keloid scar – Symptoms and causes [Internet]. Mayo Clinic. 2023.
[5] Ogawa R, Okai K, Tokumura F, Mori K, Ohmori Y, Huang C, et al. The relationship between skin stretching/contraction and pathologic scarring: The important role of mechanical forces in keloid generation. Wound Repair and Regeneration. 2012 Feb 14;20(2):149–57.
[6] Sadiq A, Khumalo NP, Bayat A. Genetics of Keloid Scarring [Internet]. Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, editors. PubMed. Cham (CH): Springer; 2020.
[7] Ogawa R, Arima J, Ono S, Hiko Hyakusoku. CASE REPORT Total Management of a Severe Case of Systemic Keloids Associated With High Blood Pressure (Hypertension): Clinical Symptoms of Keloids May Be Aggravated by Hypertension. Eplasty [Internet]. 2013 Jun 3 [cited 2025 Dec 26];13:e25.
[8] Noishiki C, Hayasaka Y, Ogawa R. Sex Differences in Keloidogenesis: An Analysis of 1659 Keloid Patients in Japan. Dermatology and Therapy [Internet]. 2019 Oct 4 [cited 2021 Dec 29];9(4):747–54.
[9] Nangole FW, Ouyang K, Anzala O, Ogengo J, Agak GW. Multiple Cytokines Elevated in Patients with Keloids: Is It an Indication of Auto-Inflammatory Disease? Journal of Inflammation Research [Internet]. 2021 Jun [cited 2024 Nov 1];Volume 14:2465–70.
[10] Rosa DF, Sarandy MM, Novaes RD, Freitas MB, do Carmo Gouveia Pelúzio M, Gonçalves RV. High-Fat Diet and Alcohol Intake Promotes Inflammation and Impairs Skin Wound Healing in Wistar Rats. Mediators of Inflammation [Internet]. 2018;2018:4658583.
[11] FC I. Is the Increase of Body Mass Index (BMI) A Risk Factor for Keloid? Clinical Dermatology Open Access Journal. 2016 May 22;1(1)
[12] Kirsner RS, Eaglstein WH. The wound healing process. Dermatologic Clinics [Internet]. 1993 Oct 1;11(4):629–40.
[13] Carswell L, Borger J. Hypertrophic Scarring Keloids [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020., Hyun Jee Kim, Yeong Ho Kim. Comprehensive Insights into Keloid Pathogenesis and Advanced Therapeutic Strategies. International Journal of Molecular Sciences [Internet]. 2024 Aug 12;25(16):8776–6.
[14] Bayat A, Arscott G, Ollier WER, Ferguson MWJ, Mc Grouther DA. Description of site-specific morphology of keloid phenotypes in an Afrocaribbean population. British Journal of Plastic Surgery. 2004 Mar;57(2):122–33.
[15] Talluri A, Gurram VS. Management of Caesarean Scar Keloid in Pregnancy: A Multidisciplinary Approach. Cureus. 2025 Oct 25.
[16] Kim SW. Management of keloid scars: noninvasive and invasive treatments. Archives of Plastic Surgery. 2021 Mar 15;48(2):149–57.
[17] Tahir SM, Ihebom D, Simman R. Compression Therapy for Keloid Scars: A Systematic Review and Meta-analysis. Plastic & Reconstructive Surgery Global Open. 2024 Jun 1;12(6):e5864–4.
[18] Yin Q, Juliette M.I. Louter, Niessen FB, Gibbs S, Gizem Tasdemir-Kilic, Lapid O, et al. Intralesional Corticosteroid Administration in the Treatment of Keloids: A Scoping Review on Injection Methods. Dermatology. 2023 Jan 1;239(3):462–77.
[19] Barara M, Chander R, Mendiratta V. Cryotherapy in treatment of keloids: Evaluation of factors affecting treatment outcome. Journal of Cutaneous and Aesthetic Surgery [Internet]. 2012 [cited 2020 Jan 13];5(3):185.
[20] Leszczynski R, da Silva CA, Pinto ACPN, Kuczynski U, da Silva EM. Laser therapy for treating hypertrophic and keloid scars. Cochrane Database of Systematic Reviews. 2022 Sep 26;2022(9).
[21] Goutos I. Intralesional excision as a surgical strategy to manage keloid scars: what’s the evidence? Scars, Burns & Healing. 2019 Jan;5:205951311986729.