
, also known as dementia with Lewy bodies (DLB), is the second most common neurodegenerative dementia after Alzheimer’s...){kind=link}

Lewy body dementia (LBD), also known as dementia with Lewy bodies (DLB), is the second most common neurodegenerative dementia after Alzheimer’s disease. Lewy bodies are abnormal aggregates of the protein alpha-synuclein that form in the brain nerve cells. These protein deposits affect brain regions responsible for cognition, behavior, and movement. LBD is an umbrella term that includes two related clinical conditions: Dementia with Lewy bodies (DLB) and Parkinson’s disease dementia (PDD). It affects approximately 1.5 million people and their families in the United States.[1]
Lewy body dementia weakens the mental abilities that gradually get worse over time. Visual hallucinations may occur in people with LBD as they may perceive things that are not present. They may also have changes in alertness and attention.
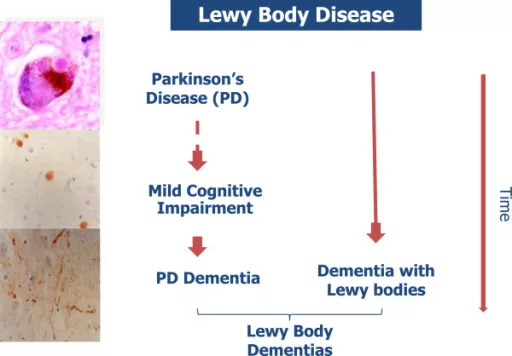
Progression of Lewy body disease: A medical infographic illustrates stages linking Parkinson’s disease, mild cognitive impairment, and dementia with Lewy bodies under the broader category of Lewy Body Dementia. Image credit: McKeith et al.,Diagnosis and management of dementia with Lewy bodies, Alzheimer’s Research & Therapy, 2014. Available viaPubMed Central(Open-i). Licensed under CC BY.
People with Lewy body dementia commonly have symptoms of Parkinson’s disease. Such symptoms may involve tremors, rigid muscles, difficulty walking, and slow movement.
LBD is not often diagnosed or misdiagnosed because its symptoms can be similar to other more familiar conditions, such as Alzheimer’s disease and Parkinson’s disease. Accurate diagnosis requires careful clinical evaluation, and awareness among clinicians has improved, but challenges remain.[2]
What is Lewy Body Dementia?
In the study of Parkinson’s, German neurologist Friedrich H. Lewy first described Lewy bodies in the early 1900s. Lewy body dementia (LBD) is a neurodegenerative disease associated with abnormal deposits of a protein called alpha-synuclein in the brain. These deposits are called Lewy bodies, and they interfere with normal brain chemistry and cause impairment of thinking, movement, behavior, mood, and other body functions.
Lewy bodies are found in several parts of the brain. When they accumulate in the brainstem, they disrupt the production of dopamine (a neurotransmitter that is vital in motor control). The decrease in dopamine leads to Parkinsonism, which includes tremor, bradykinesia, rigidity, and postural instability. Lewy bodies (LB) are also present in the cerebral cortex, where the decline of acetylcholine contributes to cognitive decline and neuropsychiatric symptoms.
LBD (Lewy body dementia) can be challenging to diagnose due to its early symptoms being similar to those of other neurodegenerative diseases, especially Alzheimer’s disease. Lewy body dementia usually starts at the age of 50 or older, but younger people can also be affected. It seems to be a little more prevalent in men than in women. LBD is a progressive disease, and the symptoms appear slowly and become more severe. The average LBD duration is five to seven years after diagnosis, but it can be between two and twenty years, depending on the individual factors.[3]
Symptoms of Lewy body dementia
LBD produces a mix of symptoms. They can be different for each person. Some symptoms start early or show up later. It may slowly get worse over time.
Cognitive Impairment (Thinking)
Lewy body dementia causes changes in thinking abilities. These changes include
- Impaired Attention and Concentration
- Fluctuating cognition (episodes of confusion alternating with clarity)
- Memory Dysfunction (often less prominent early compared to Alzheimer’s disease)
- Disorientation
- Disorganized thought processes
- Visual Hallucinations (often well-formed and recurrent)
- Language Impairment[4]
Mood and behavior
Behavior and mood changes are seen in LBD. It may vary from person to person according to their level of cognitive decline. These changes may include
- Affective Disorders (anxiety, and emotional lability)
- Apathy
- Sadness
- Psychotic Features (Delusions (usually paranoid) and hallucinations develop)
- Behavioral Disturbances (Agitation, irritability, and restlessness)
Motor (Extrapyramidal) Symptoms
Some individuals with LBD do not experience movement symptoms for several years. Some have them early on, and some people never develop movement symptoms. The signs of these problems are very mild or easily overlooked. These symptoms include:
- Bradykinesia (Slowness of voluntary movements)
- Muscle Rigidity
- Resting Tremor (Uncontrolled rhythmic movements of oscillation)
- Gait Abnormalities (Shuffling, decreased arm swing, and instability)
- Dysarthria and Dysphagia (speech articulation and swallowing)
- Hypomimia (Loss of facial expressiveness).
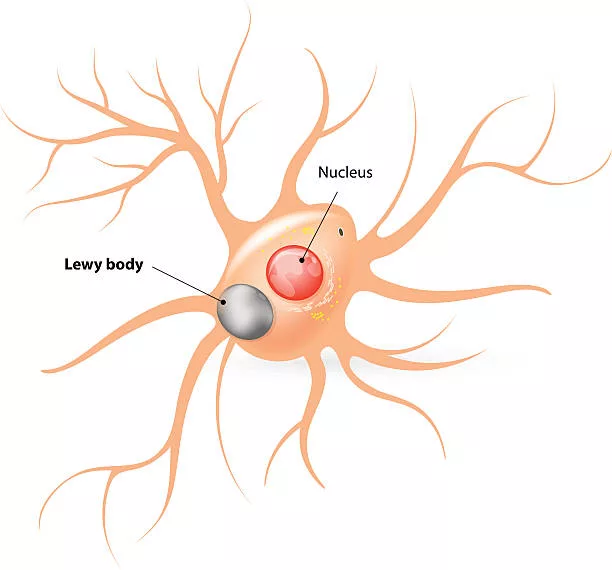
A labeled diagram of a nerve cell highlights the nucleus and a Lewy body inclusion within the cell.
Dysfunction of the Autonomic Nervous System
People with LBD also suffer from dysfunction of the Autonomic Nervous System. Some of the nervous system symptoms may include
- Orthostatic Hypotension
- Sialorrhea (excessive salivation)
- Gastrointestinal dysfunction (especially constipation)
- Rhinorrhea (runny nose)
- Bladder Dysfunction
- Hyperhidrosis (excessive sweating)
- Sexual dysfunction
- Seborrheic dermatitis (itchy rash with flaky skin)
- Fainting
- Thermoregulatory Dysfunction
- Hyposmia/Anosmia
- Heat and cold insensitivity[5] [6]
Sleep Disorders
Sleep disorders are undiagnosed but common in people with LBD. LBD sleep disorders may include:
- Insomnia
- REM Sleep Behavior Disorder (RBD)
- Excessive Daytime Somnolence
- Restless Legs Syndrome (RLS)[7] [8]
Lewy Body Dementia Causes
The cause of LBD is unknown, but scientists are learning more about its biology and genetics. Lewy body dementia occurs when proteins called alpha-synuclein, called Lewy bodies, build up in brain cells.
This buildup leads to the loss of neurons that produce important neurotransmitters:
- Acetylcholine (affecting memory and learning)
- Dopamine (affecting movement and behavior)
Many patients with LBD also have coexisting Alzheimer-type pathology, including amyloid plaques and tau tangles.
A medical 3D graphic depicting brain degeneration and neuron communication, commonly associated with Lewy body dementia.
Doctors and researchers don’t know why some people get LBD, and others don’t.[9]
Risk factors of LBD
Researchers are also getting to know about LBD risk factors.
- Age is considered the greatest risk factor, with most people developing the disorder over age 50.
- LBD affects men more than women.
- A biological family history of Lewy bodies or Parkinson’s disease can also raise the risk of LBD.
- Some diseases and health conditions, especially REM sleep behavior disorder and loss of smell, are associated with increased risk of Lewy body dementia.
Other general risk factors:
- Diet
- Lack of exercise
- Toxic exposures
These may contribute to general neurodegenerative risk. Scientists and researchers are still studying other risk factors that may raise the risk of developing this condition or disease.[10]
Complications of Lewy body dementia
It can lead to serious health problems or diseases, and some may be life-threatening:
- Pneumonia (often due to swallowing difficulties)
- Heart problems
- Aggressive behavior
- Tremors (worsening movement signs)
- Trouble eating, swallowing, or speaking
- Increased risk of injury and falling
- Need help walking or moving
- Depression (increases the risk of suicide)
- May cause death (7 to 8 years after symptoms start). Death is usually related to complications such as aspiration pneumonia, immobility, or infections rather than the disease itself.[11]
The 7 Stages of Lewy Body Dementia Explained
There is no universally accepted staging system for LBD. Unlike Alzheimer’s disease, progression is often variable and marked by fluctuations rather than a strictly linear decline. However, clinicians sometimes describe its course using generalized stages adapted from broader dementia models.
- Preclinical Stage
- Very Mild Cognitive Decline.
- Mild Cognitive Decline
- Mild Dementia
- Moderate Dementia
- Severe Cognitive Decline
- Late-Stage Lewy Body Dementia
The experience can appear in various forms to different individuals, yet these phases can be used as a guide to follow the process.[12]
Stage 1: No Cognitive Decline (Also known as the Preclinical Stage)
In the first stage, symptoms may not be noticeable. Individuals with this stage may have slight changes in behavior. Stage one patients can have restlessness, REM sleep behavior disorder, mild anxiety, depression, or a reduced sense of smell. Individuals can also exhibit problems in decision-making and recalling some events.
Motor symptoms such as tremor or stiffness are not consistently present at this stage and should not be considered diagnostic.
The initial signs of LBD resemble those of Alzheimer’s and Parkinson’s diseases. It is, therefore, important to consult a doctor in case you experience any of the above symptoms. They can indicate a diagnosis of LBD.
Stage 2: Very Mild Cognitive Decline
During the second stage, the symptoms can be more severe. Often called mild cognitive impairment (MCI), stage two symptoms result in declines in cognitive functioning. Some initial symptoms in stage two are recall, language processing, and problem-solving. Activities that involve focus and multitasking may be a challenge.
Many people diagnosed with Lewy body dementia can maintain their independence and not need help with activities of daily living. In individuals who have early symptoms of Lewy body dementia, it is important to exclude the diagnosis of Alzheimer’s disease or Parkinson’s disease with dementia. Fluctuations in cognition may begin to appear, which is a key feature distinguishing LBD from Alzheimer’s disease.
Stage 3: Early Dementia (Mild LBD)
During the third stage of LBD, the symptoms are more severe. At stage three, people who live with LBD may have increased anxiety, depression, and apathy about life. They may need help with more complex daily activities (such as managing their finances and taking medications). It’s at this stage that people with LBD may become frustrated or overcome with emotion. Parkinsonian features (slowness, rigidity) may begin to appear around this stage or earlier, depending on whether the presentation aligns with DLB or PDD.[13]
Stage 4: Moderate Cognitive Decline (Moderate Dementia)
It’s usually at stage four where a person may experience a decline in cognitive abilities. For example, many people have issues with dressing, bathing, eating, remembering, problem-solving, and communicating with others.
LBD is diagnosed in many individuals at stage four since it has become more apparent. Individuals with LBD can also get agitated, confused, and paranoid at this phase. Fluctuations in awareness and attention become more pronounced and can vary significantly from day to day.
Stage 5: Moderately Severe Cognitive Decline (Moderately Severe Dementia)
During stage 5 of LBD, the symptoms can be more prominent and severe. A person with Lewy bodies can start to lose cognitive functions considerably.
As an example, a person with LBD might lose the capacity to communicate and carry out everyday tasks. They can be confused, lost, and struggle to resolve daily issues.
LBD can lead to the individual’s inability to identify family and friends. Therefore, individuals with Lewy body dementia can be more dependent on their caregivers to offer a supportive and loving living environment. Autonomic symptoms such asorthostatic hypotension and constipation may also become more prominent.
Stage 6: Severe Cognitive Decline (Moderately Severe Dementia)
The sixth stage is characterized by increased symptoms and severity of the disease. The person can no longer communicate or respond to family and friends.
The person may need the help of a full-time caregiver 100% of the time. An individual with Lewy body dementia in stage six might not be capable of walking or sitting up without assistance. Swallowing difficulties (dysphagia) may develop, increasing the risk of aspiration pneumonia.
An individual with LBD can also exhibit agitation, aggression, and potential hallucinations. Individuals with LBD may have moments of clarity in which they respond to familiar voices.[14]
Stage 7: Late-Stage Lewy Body Dementia (Severe Cognitive Decline)
During end-stage LBD, individuals have severe cognitive and physical impairment. The individual in stage seven may also experience a total loss of memory, speech difficulties, and struggles with performing basic daily tasks when the disease advances.
People may experience a decrease in mobility, and confusion may increase. Cognitive and physical symptoms have advanced to stage seven, but individuals can and do continue to live full and rewarding lives.
Because the process of dementia differs among individuals, determining the appropriate type of memory and dementia care will help you and your loved one live your best life at this last stage.[15]
Diagnosis of LBD and Tests
Physical and neurological exams and other tests are done by doctors to differentiate between LBD and other diseases. DLB diagnosis is typically clinical in nature and is determined by the presence of core clinical patterns, such as fluctuating cognition (severe changes in attention and alertness), visual hallucinations, REM sleep behavior disorder (RBD), and Parkinsonism (bradykinesia, rigidity, and gait instability).
Besides clinical evaluation, dopamine transporter imaging (DaT scan) with either a SPECT or a PET can be used as a supportive biomarker. Dopamine transporter (DaT) imaging showing reduced uptake. Nevertheless, there is no single test, brain scan, or medical test that can definitively diagnose LBD.[16]
Medical history and physical examination
- A brief history of past and current diseases, medicines, and symptom progression
- Analysis of cognitive function, behavior, or motor symptoms/signs
- Analysis of memory impairment and movement abnormalities
Neuropsychological tests
These tests are used to evaluate memory and other cognitive functions and could help to determine affected parts of the brain. Doctors may examine you to detect any Parkinson’s disease, strokes, tumors, or other illnesses. A neurological exam includes
- Strength
- Walking
- Balance
- Reflexes
- Sense of touch
- Muscle tone
- Eye movements
Medical tests
The blood and other tests can be analyzed in the laboratory to exclude other diseases, hormonal issues, and vitamin deficiencies that may be related to cognitive changes. A sleep test known as a polysomnogram may be required to diagnose REM sleep behavior disorder, which can be treated.
Brain imaging
Various brain imaging methods, including CT scans, MRIs, and some forms of PET (positron emission tomography) scans, can identify brain shrinkage and structural abnormalities and can be used to exclude other potential causes of dementia. Fluorodeoxyglucose PET brain scans, which measure brain functionality.
Single-photon emission computerized tomography (SPECT) or PET images. Such tests may indicate the decreased uptake of dopamine transporters in the brain. This may aid in the diagnosis of Lewy body dementia. No single brain scan or medical test can definitively diagnose LBD.[17]
Management and Treatment
There is no cure for Lewy body dementia and no way to prevent it. However, drugs and treatment can be used to deal with symptoms temporarily.
Medications for Lewy body dementia
Doctors can provide various drugs. These can include:
- Cholinesterase inhibitors (galantamine, rivastigmine, or donepezil) to enhance thinking and memory. (Rivastigmine is commonly preferred)
- Antipsychotics (clozapine, pimavanserin, quetiapine, or aripiprazole) are used to treat hallucinations that do not respond to cholinesterase inhibitors.
Note: Patients with LBD may have severe sensitivity to antipsychotics, which can worsen symptoms or cause serious adverse effects.
- Carbidopa-levodopa to aid movement difficulties.
- Antidepressants (such as SSRIs) are used to deal with depression.
- Clonazepam and melatonin are used for REM or sleep disorders.
- Memantine to relieve the early symptoms. Notably, it is used as an adjunct therapy in moderate to severe cases of Lewy body dementia, but its benefits are variable, and it is not considered first-line treatment compared to cholinesterase inhibitors.
Doctors can also prescribe drugs to treat nervous system symptoms, such as dizziness or changes in blood pressure when standing. They are normally prescribed when other measures such as elevating your legs, consuming more salt-based foods, or taking in more fluids do not work.[18]
Therapies for Lewy body dementia
Various forms of treatment can be useful, such as:
Occupational therapy
Help patients to stay independent through teaching methods of coping with everyday activities.
Physical therapy
Improves strength, balance, and ability to move
Speech therapy
Helps with speaking, language, and swallowing
A calm and steady routine can be a benefit as well. This can prevent symptoms such as agitation, stress, and confusion. Support groups, individual and family psychotherapies, Music/art therapy, and exercise also help deal with LBD.[19]
What’s the difference between Lewy Body Dementia (LBD) and Alzheimer’s disease?
Lewy Body Dementia (LBD) and Alzheimer’s are both progressive neurodegenerative diseases that are incurable, and differ in their early symptoms. LBD mostly begins with cognitive changes, clear hallucinations, and movement problems, whereas Alzheimer’s usually begins with severe short-term memory loss. LBD is caused by the abnormal protein deposits (Lewy bodies), and Alzheimer’s is associated with amyloid plaques and tau tangles.[20]
What is the life expectancy for people with Lewy body dementia?
On average, people tend to live five to seven years after diagnosis, but it is possible to live much longer.
Prognosis
The prognosis is generally progressive and variable, with a gradual decline. The patients succumb to several complications such as falls, immobility, heart complications, drug side effects, pneumonia, difficulty in swallowing, and suicide due to depression. Upon initial diagnosis, the average life expectancy is 5-8 years. It may also be caused by the insufficiency of knowledge about LBD among doctors and the population. and the inability to distinguish it from other similar diseases. which results in a delay in the diagnosis and postpones the onset of the targeted treatment. Healthcare providers should enhance awareness about LBD and establish investigative techniques to make an early diagnosis.[21]
Wrap up
Lewy Body Dementia is a complicated, progressive neurodegenerative illness that causes cognitive impairment across multiple domains, neuropsychiatric abnormalities, Parkinsonian movement symptoms, and autonomic dysfunction. LBD exhibits a variable clinical course with a strong influence on functional capacity and life quality as described in its symptoms, causes, diagnosis, progression, and treatment. The optimal patient outcomes depend on early recognition, correct differential diagnosis with conditions like Alzheimer’s disease, and a multidisciplinary treatment approach. There is no definite cure, but timely therapeutic interventions and supportive care can help to reduce the burden of symptoms and improve the overall prognosis.
References
[1] Galvin, J. E., Duda, J. E., Kaufer, D. I., Lippa, C. F., Taylor, A., & Zarit, S. H. (2010). Lewy body dementia: The caregiver experience of clinical care.Parkinsonism & Related Disorders,16(6), 388–392. https://doi.org/10.1016/j.parkreldis.2010.03.007
[2] Haider, A., & Sánchez-Manso, J. C. (2023, February 12).Lewy Body Dementia. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482441/
[3] Hanson, J. C., & Lippa, C. F. (2009). Chapter 11 Lewy Body Dementia.International Review of Neurobiology,84, 215–228. https://doi.org/10.1016/s0074-7742(09)00411-5
[4] Wiese, L. K., Lingler, J., & Lindauer, A. (2021). Alzheimer’s disease and Lewy body dementia: Discerning the differences: Assessment is key for optimal management.American Nurse Journal,16(1), 10. https://pmc.ncbi.nlm.nih.gov/articles/PMC9266700/#S10
[5] Wiese, L. K., Lingler, J., & Lindauer, A. (2021). Alzheimer’s disease and Lewy body dementia: Discerning the differences: Assessment is key for optimal management.American Nurse Journal,16(1), 10, https://pmc.ncbi.nlm.nih.gov/articles/PMC9266700/#S10
[6] Morrin, H., Fang, T., Servant, D., Aarsland, D., & Rajkumar, A. P. (2017). Systematic review of the efficacy of non-pharmacological interventions in people with Lewy body dementia.International Psychogeriatrics,30(3), 395–407. https://doi.org/10.1017/s1041610217002010
[7] Simard, M., van Reekum, R., & Cohen, T. (2000). A review of the cognitive and behavioral symptoms in dementia with Lewy bodies.The Journal of Neuropsychiatry and Clinical Neurosciences,12(4), 425–450. https://doi.org/10.1176/jnp.12.4.425
[8] Wiese, L. K., Lingler, J., & Lindauer, A. (2021). Alzheimer’s disease and Lewy body dementia: Discerning the differences: Assessment is key for optimal management.American Nurse Journal,16(1), 10. https://pmc.ncbi.nlm.nih.gov/articles/PMC9266700/#S10
[9] Hanson, J. C., & Lippa, C. F. (2009). Chapter 11 Lewy Body Dementia.International Review of Neurobiology,84, 215–228. https://doi.org/10.1016/s0074-7742(09)00411-5
[10] Kuring, J. K., Mathias, J. L., & Ward, L. (2020). Risk of Dementia in persons who have previously experienced clinically-significant Depression, Anxiety, or PTSD: A Systematic Review and Meta-Analysis.Journal of Affective Disorders,274, 247–261. https://doi.org/10.1016/j.jad.2020.05.020
[11] McKeith, I. G., & Mosimann, U. P. (2004). Dementia with Lewy bodies and Parkinson’s disease.Parkinsonism & Related Disorders,10, S15–S18. https://doi.org/10.1016/j.parkreldis.2003.12.005
[12] Armstrong, M. J. (2021). Advances in dementia with Lewy bodies.Therapeutic Advances in Neurological Disorders,14, 175628642110576. https://doi.org/10.1177/17562864211057666
[13] Boeve, B. F. (2012). Mild cognitive impairment associated with underlying Alzheimer’s disease versus Lewy body disease.Parkinsonism & Related Disorders,18, S41–S44. https://doi.org/10.1016/s1353-8020(11)70015-3
[14] Forlenza, O. V., Diniz, B. S., Stella, F., Teixeira, A. L., & Gattaz, W. F. (2013). Mild cognitive impairment (part 1): clinical characteristics and predictors of dementia.Revista Brasileira de Psiquiatria,35(2), 178–185. https://doi.org/10.1590/1516-4446-2012-3503
[15] Jessen, F., Amariglio, R. E., Buckley, R. F., van der Flier, W. M., Han, Y., Molinuevo, J. L., Rabin, L., Rentz, D. M., Rodriguez-Gomez, O., Saykin, A. J., Sikkes, S. A. M., Smart, C. M., Wolfsgruber, S., & Wagner, M. (2020). The characterisation of subjective cognitive decline.The Lancet Neurology,19(3), 271–278. https://doi.org/10.1016/s1474-4422(19)30368-0
[16] McKeith, I. G., Boeve, B. F., Dickson, D. W., Halliday, G., Taylor, J.-P., Weintraub, D., Aarsland, D., Galvin, J., Attems, J., Ballard, C. G., Bayston, A., Beach, T. G., Blanc, F., Bohnen, N., Bonanni, L., Bras, J., Brundin, P., Burn, D., Chen-Plotkin, A., & Duda, J. E. (2017). Diagnosis and management of dementia with Lewy bodies.Neurology,89(1), 88–100. https://doi.org/10.1212/wnl.0000000000004058
[17] McKeith, I. G., Boeve, B. F., Dickson, D. W., Halliday, G., Taylor, J.-P., Weintraub, D., Aarsland, D., Galvin, J., Attems, J., Ballard, C. G., Bayston, A., Beach, T. G., Blanc, F., Bohnen, N., Bonanni, L., Bras, J., Brundin, P., Burn, D., Chen-Plotkin, A., & Duda, J. E. (2017). Diagnosis and management of dementia with Lewy bodies.Neurology,89(1), 88–100. https://doi.org/10.1212/wnl.0000000000004058
[18] Kuring, J. K., Mathias, J. L., & Ward, L. (2020). Risk of Dementia in persons who have previously experienced clinically-significant Depression, Anxiety, or PTSD: A Systematic Review and Meta-Analysis.Journal of Affective Disorders,274, 247–261. https://doi.org/10.1016/j.jad.2020.05.020
[19] McKeith, I. G., & Mosimann, U. P. (2004). Dementia with Lewy bodies and Parkinson’s disease.Parkinsonism & Related Disorders,10, S15–S18. https://doi.org/10.1016/j.parkreldis.2003.12.005
[20] Robillard, A. (2007). Clinical diagnosis of dementia.Alzheimer’s & Dementia,3(4), 292–298. https://doi.org/10.1016/j.jalz.2007.08.002
[21] Haider, A., & Sánchez-Manso, J. C. (2023, February 12).Lewy Body Dementia. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482441/