
, also known as Hereditary Non-Polyposis Colorectal Cancer (HNPCC), is a genetic condition that...){kind=link}

Lynch Syndrome Symptoms Lynch syndrome (LS), also known as Hereditary Non-Polyposis Colorectal Cancer (HNPCC), is a genetic condition that increases the risk of cancers (particularly colorectal and endometrial cancers). Reports suggest that lynch syndrome contributes to 2-3% of all colorectal cancers.[1] It is the most common cause of hereditary colorectal cancer and is found to be present in 1 in every 279 individuals.[2]
Patients also face higher risks of ovarian, gastric, small intestine, pancreatic, hepatobiliary tract, urinary tract, brain, and certain skin cancers. The disease usually causes an early onset of cancers in patients, i.e., below 50 years of age. Currently, there is no cure for the genetic predisposition in Lynch syndrome. However, doctors focus on early detection through regular screening, preventive surgeries, and advanced therapies such as immunotherapy for mismatch repair-deficient cancers. Sadly, cancers caused by the syndrome tend to recur even after removal.
Cancer Types
As mentioned, colorectal and uterine (endometrial) cancers are most frequently seen in Lynch syndrome cases. Colorectal cancers in LS can be aggressive and may spread if not detected early. Endometrial cancer is strongly associated with defects in mismatch repair genes, making it a frequent extracolonic manifestation.[3] However, you can also fall prey to other types of cancers, including:
Ovarian Cancer:
This multi-tumor syndrome is associated with the development of epithelial ovarian cancers. Researchers believe that this type of cancer activates the immune response of the body, which makes it a potential candidate for immunotherapy.[4]
Skin Cancer:
Individuals suffering from Lynch syndrome are also prone to developing skin neoplasms. There is a strong association between skin cancers and LS.[5] Lynch syndrome can present with sebaceous skin tumors, a feature known as Muir-Torre syndrome. Because of this, experts recommend regular dermatologic surveillance for LS carriers, as studies show about 9% of patients may develop LS-associated skin neoplasms.[6]
Liver Cancer:
This syndrome can have an impact on the largest gland in your body. Hepatocellular carcinoma (cancer of the liver cells) is a rare extracolonic manifestation of the LS. Researchers believe that pro-carcinogenic growth in the liver cells is attributed to changes in the SEC63 gene.[7]
Pancreatic Cancer:
Patients may also develop pancreatic cancer or biliary tract cancers as a result of the genetic mutations.[8]
Small Intestine Cancer:
Lynch syndrome is notorious for causing cancerous growths in the large intestine (colon) and the rectum. However, it may also induce uncontrolled division of cells in the small bowel as well. The defective DNA mismatch repair (MMR) genes increase the patient’s propensity to develop small-intestinal adenocarcinomas. These carcinomas may be the initial presentation of the disorder in several patients.[9]
Gallbladder Cancer:
A common extracolonic presentation of the lynch syndrome is cancer of the biliary tract. These types of cancers (biliary tract and pancreatic cancers) are difficult to treat because they are diagnosed pretty late.[10]
Stomach Cancer:
Lynch syndrome patients suffering from atrophic gastritis are at the highest risk of developing gastric cancer. Patients can acquire gastric neoplasms without having atrophic gastritis. However, the chances are greater with the inflammatory disorder.[11]
In addition to the above, LS has been associated with cancers of the brain (glioblastomas), prostate, and the upper urinary tract (renal pelvis and ureter). Studies show LS carriers have up to a 14-fold increased risk of urothelial carcinomas of the urinary tract.[12]
The relationship between LS and breast cancer remains debated. While some studies suggest a slightly elevated risk, breast cancer is not yet considered a core Lynch-associated cancer, though vigilance in postmenopausal women is advised.
Lynch Syndrome Types
The genetic condition is historically divided into two categories, which are mentioned below:
Type Ⅰ:
In this type (aka familial colorectal cancer), cancers develop at an early age, and there is a chance of multiple primary colorectal cancers arising. However, in such patients, the primary focus is on colorectal cancers only.
Type Ⅱ:
There is an increased risk of colorectal cancer. However, patients can also develop other types of cancers, namely endometrial, ovarian, and biliary tract cancers etc.
Another type, i.e., Muir-Torre syndrome (MTS), also exists, which is characterized by the development of keratocanthomas (skin tumors) and sebaceous gland tumors. This variant of HNPCC also arises due to a defect in the MMR genes. Doctors identify it as MTS if there is at least one visceral malignancy and one skin (cutaneous) neoplasm of the sebaceous gland.[13]
It is important to note that this Type I/II classification is more historical, and in modern practice, doctors focus on the underlying genetic mutations in the mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2) or EPCAM deletions when diagnosing and managing Lynch syndrome.
Lynch Syndrome Symptoms
Lynch syndrome itself does not cause obvious symptoms until cancer develops. Most patients remain asymptomatic until they are diagnosed with colorectal, endometrial, or other associated cancers. The symptoms, therefore, depend on the type and site of cancer present:
Colorectal Cancer Symptoms
Blood In Stools:
You may notice some blood in your stools. The disorder is notorious for changing the microbiota of the large bowel, which shows in the excretions. Stool samples from patients with adenomas reveal a raised number of Desulfovibrio bacteria. In a clinical case, a 69-year-old woman reported gastrointestinal bleeding and altered bowel movement was found to be suffering from HNPCC-induced colorectal cancer.[14]
Diarrhea:
By altering the bowel movements and microbiota (of the mucosa), lynch syndrome potentially causes gastric upset in patients. You may develop diarrhea due to the underlying colorectal cancer. A 49-year-old perimenopausal woman suffering from HNPCC-induced endometrial carcinoma reported diarrhea and intermittent fever for more than 1 month before being diagnosed with lynch syndrome.[15]
Constipation:
As mentioned, issues related to the digestive system are frequent in HNPCC. Thus, constipation can be a presenting symptom of the mutational disorder. In a clinical report, a 57-year-old woman presented with chronic constipation and abdominal discomfort for twenty years. Genetic testing revealed that she was suffering from Lynch syndrome.[16]
Bloating & Abdominal Pain:
Patients often experience abdominal distention and bloating due to colorectal cancers. Abdominal pain in CRC patients may accompany symptoms of bloating.[17]
Nausea & Vomiting:
Young patients with lynch syndrome report nausea and vomiting unrelated to food intake or acid reflux. These symptoms are attributed to underlying cancers developing in the body.
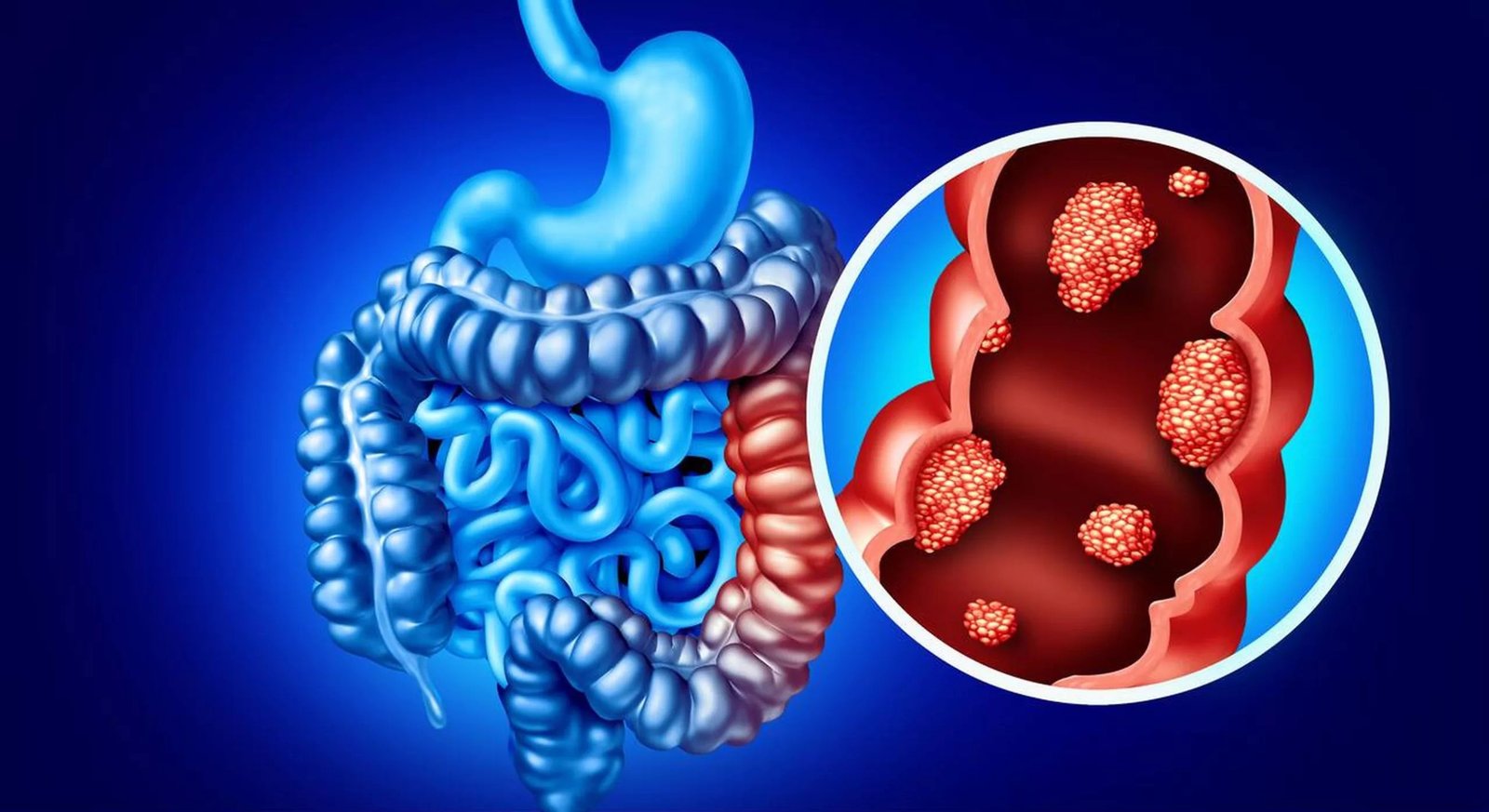
Illustration of colorectal cancer highlighting abnormal tumor growth in the colon lining.
Endometrial and Ovarian Cancer Symptoms
Women may present with abnormal uterine bleeding, pelvic or abdominal pain, and sometimes urinary urgency or bloating due to the tumor burden.
Other Cancer Symptoms
Depending on the site, LS-related cancers may cause fatigue, nausea, vomiting, or site-specific symptoms. For example, urinary tract cancers may cause hematuria (blood in urine), while stomach or small bowel cancers may lead to persistent indigestion, abdominal discomfort, or obstruction.
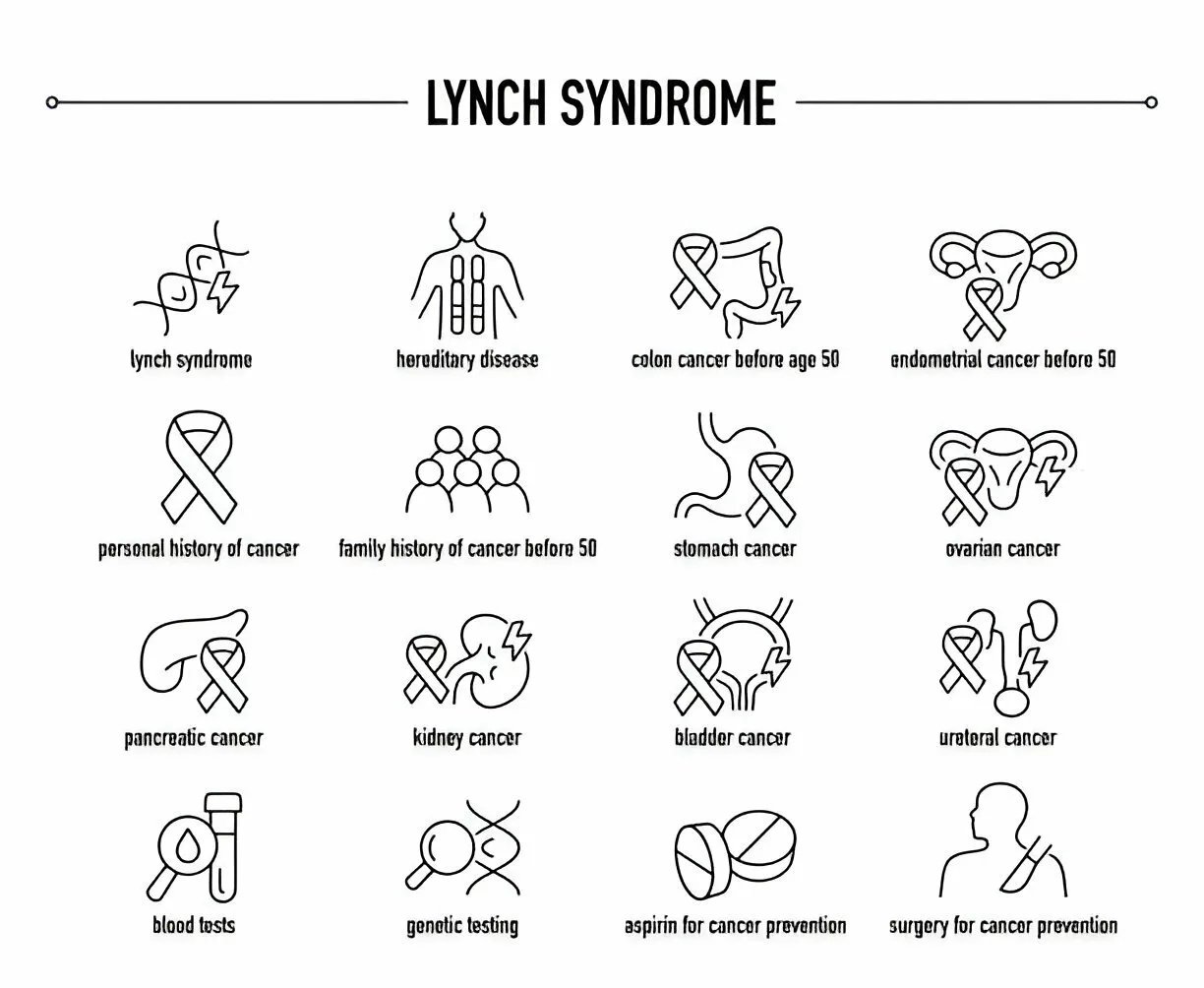
Vector Illustration showing manifestations of Lynch Syndrome
Lynch Syndrome Causes
Your body is naturally capable of fixing any errors in your DNA, like mismatches between DNA bases or deletions, etc. This feature helps the body maintain the integrity of its genome. However, sometimes, the genes controlling this correction can become mutated, leading to uncontrolled division of cells (known as cancers). This is what happens in lynch syndrome as well.
There are five genes called the mismatch repair (MMR) genes, which are responsible for fixing errors in the DNA. A genetic mutation in one of these five genes causes HNPCC:[18]
- MSH2
- MSH6
- MLH1
- PMS2
- EPCAM (large deletions in EPCAM silence the neighboring MSH2 gene, causing MMR deficiency)
With no instructions from the MMR genes, there is no elimination of damaged cells. Thus, there is a buildup of abnormal DNA, which eventually leads to the development of cancers in different parts of the body.
Detailed studies reveal that the MLH1 variant has the highest risk of colorectal cancers, while the MSH2 variant carries the highest risk of other types of cancers.[19]
Microsatellite Instability:
There are short, repeating DNA sequences throughout your genome known as microsatellites. These sequences are prone to error. When mismatch gene repair is deficient (due to a genetic mutation), the microsatellites become unstable. The result of this instability is a higher rate of insertions and deletions. This phenomenon is known as microsatellite instability and is pretty common in cancers arising from underlying Lynch syndrome.[20]
Lynch Syndrome Inheritance:
PNCC is an autosomal dominant condition, which means that a mutated gene from one parent is sufficient to cause the disorder in the offspring. Thus, patients must inform about their disease to family members. Genetic counselling helps evaluate the risk of the disease in future offspring.
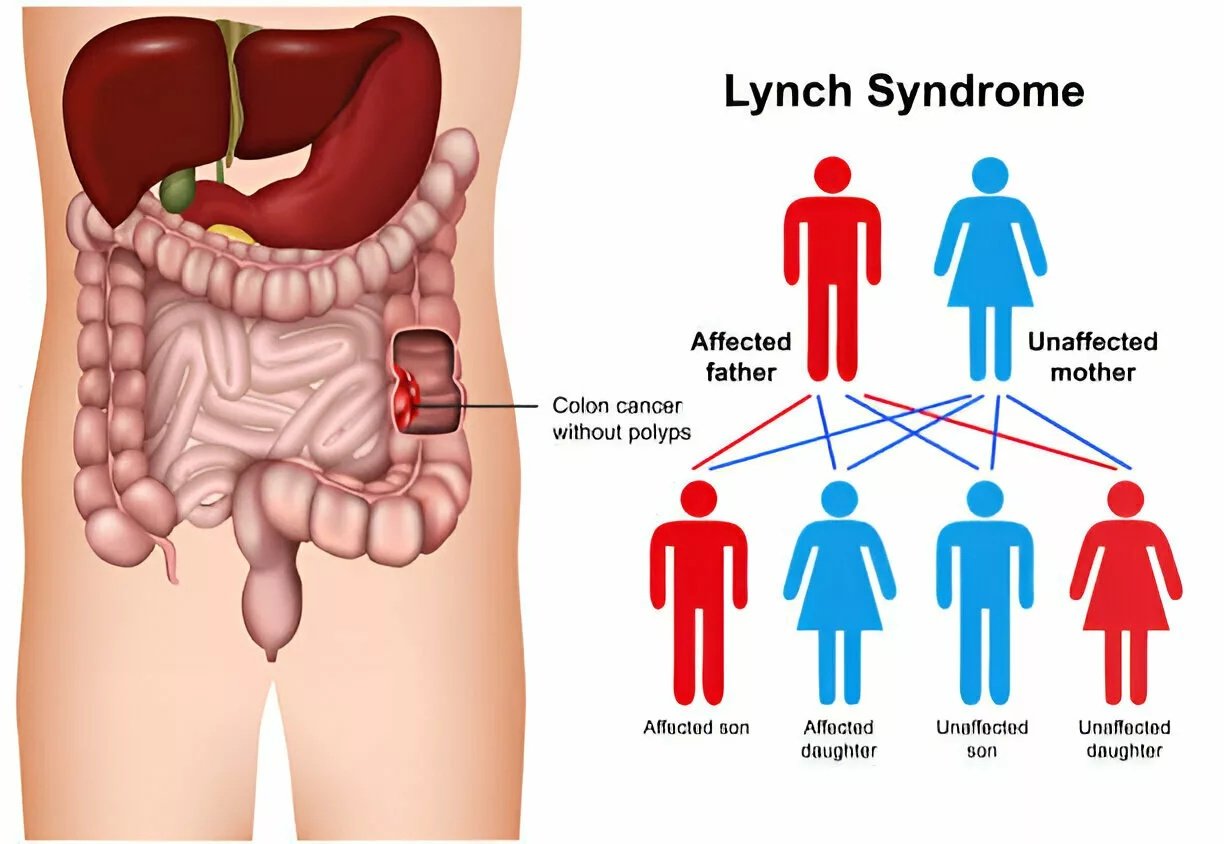
The illustration shows the chances of lynch syndrome in children if one of the parents is a carrier/patient.
Lynch Syndrome Diagnosis
Doctors reach a diagnosis after thoroughly analyzing your symptoms. The history of the symptoms and familial history of the disorder are important questions. If lynch syndrome is suspected, your healthcare provider may order the following tests:
Genetic Testing:
The primary test in diagnosing hereditary non-polyposis colorectal cancer is genetic testing. Your doctor will likely advise genetic testing for you and your children if you have a familial history of lynch syndrome.
In this test, a healthcare provider takes a sample (from a blood sample or a buccal swab from your mouth). Lab technicians analyze the samples to determine which genes have mutated. Doctors confirm the diagnosis if genetic mutations are identified in samples. This method of diagnosis is cost-effective and aids in informed decision-making.[21]
Microsatellite instability testing helps in lynch syndrome diagnosis.
In addition to genetic testing, doctors may also carry out tests like:
- Microsatellite instability testing: This test checks the stability of microsatellites in a sample.
- Immunohistochemistry (IHC) testing: It involves using special dyes to stain samples and check that stains (related to specific proteins) are missing. Data regarding the missing proteins can help determine the genes involved in Lynch syndrome.
Your healthcare provider will order the following tests after a confirmed diagnosis of lynch syndrome:
Imaging Studies:
Colonoscopy
Colonoscopy refers to a diagnostic test in which a doctor examines the inside of the colon and the bowels (small and large intestines) by inserting a thin, flexible tube with an endoscope (camera). This study allows doctors to diagnose colorectal cancers. Screening colonoscopy in patients with lynch syndrome can prove to be an effective surveillance strategy. Timely colonoscopies have even been shown to reduce the incidence of colorectal cancers.[22]
Endoscopy
Doctors can also use an endoscope to visualize the small bowel and the stomach to check for cancers. This can be done in an upper endoscopy procedure. Your doctor may also give you a capsule to swallow. This capsule contains a tiny camera and light that takes pictures of the digestive tract in a process called capsule endoscopy.
Ultrasound
To check for uterine and endometrial cancers, your health professional might perform a transvaginal ultrasound. This imaging test helps examine the uterus and the ovaries with the help of a probe, which is inserted into the vaginal canal. Your doctor may also repeat these ultrasounds every year or so to use them as a screening test for endometrial cancer.
Urine Test:
A urine sample can also provide valuable information regarding complications associated with Lynch syndrome. Urinalysis is mostly done in cases of urothelial carcinomas.
Biopsy:
Your doctor may remove a small sample of the cancerous growth for a detailed analysis. This removal of the tumour segment is called a biopsy. After removing the tissue sample of the tumor is sent to the lab for microscopic examination.
Differential Diagnosis
Lynch Syndrome Vs Familial Adenomatous Polyposis (FAP)
Both are inherited conditions, but there are significant differences between the two. While lynch syndrome is known to cause colorectal cancer, familial adenomatous polyposis causes the development of coloured polyps in the colorectal region. Unlike lynch syndrome, FAP arises due to a mutation in the APC gene instead of the MMR genes. FAP increases the risk of small intestine and colorectal cancer. On the other hand, HNPCC can cause different types of cancers, including pancreatic cancer, brain cancer, etc.
Lynch Syndrome Treatment
Due to the wide range of organs involved, lynch syndrome treatment generally requires a team of clinicians, including oncologists, gastroenterologists, gynaecologists, and urologists etc. Geneticists and genetic counselors also play a vital role in the management of the disease and the guidance of the patients.
There is no cure to treat the genetic mutation. Most of the time, management involves detecting and surgically removing cancers from your body. Oncological management differs for different types of cancers. Surgeons remove colonic adenomas via a complete endoscopic polypectomy with a follow-up colonoscopy every one to two years.
Chemotherapy (with chemotherapeutic agents like fluorouracil, irinotecan, oxaliplatin, and leucovorin) can only be used as an adjuvant in the treatment of sporadic cancers.
Immunotherapy:
Immunotherapy is a cancer treatment type that stimulates the body’s immune system to eliminate or fight the cancer cells. In the recent past, immune checkpoint-inhibiting agents have shown promising results as anti-tumor drugs for lynch syndrome-induced CRC.[23] Immunotherapeutic drug pembrolizumab is now the first-line treatment in the UK for metastatic MSI-high (microsatellite instability)/dMMR (deficient mismatch repair gene) CRCs.[24]
Lynch Syndrome Prognosis
The syndrome has a good prognosis with early detection and treatment. Clinical studies show that the overall survival of HNPCC patients with colorectal cancer is:
- 90% (approximately) at 5 years
- 80% at 10 years
- 70% at 15 years
The study also found that the metachronous (occurring at different times) tumor rate was 10-30% at up to 15 years. This rate significantly improved with subtotal or total colectomy.[25]
Some patients (diagnosed with the syndrome) undergo surgical removal of prone organs to prevent disease complications before cancers develop. Common procedures include colectomy (intestine removal), hysterectomy (uterus removal), and oophorectomy (ovaries removal).
How To Prevent Lynch Syndrome?
Limited evidence suggests that a daily low-dose (100mg/day) of aspirin can prevent colorectal cancer development in LS carriers.[26]
If you are a lynch syndrome gene carrier, cancer screening can save you from advanced disease. You can follow these steps for screening:
- Colon cancer: A screening colonoscopy every year or two after turning 20.
- Endometrial/Ovarian cancer: A transvaginal ultrasound every year or two.
- Stomach/Small intestine cancer: An endoscopy every two to five years.
- Urinary tract/system cancer: A urinalysis every year or two.
Final Word
Hereditary non-polyposis colorectal cancer, or lynch syndrome, is a genetic mutation disorder that impacts the mismatch repair (MMR) genes. The deficiency in mismatch gene repair leads to the development of faulty DNA in cells, which can cause cancers in various organs. Colorectal cancers (CRCs) and endometrial cancers are the most common cancers, but patients can also develop intestinal, brain, pancreatic, and breast cancer.
Most patients with CRCs experience intestinal symptoms like diarrhea, constipation, blood in stools, and bloating, etc. Diagnosis is mainly done via genetic testing. To further investigate cancers, doctors use endoscopy, colonoscopy, ultrasounds, and tumor biopsies. There is currently no cure for the disorder. However, timely diagnosis and treatment of the specific cancer saves from disease exacerbations. Immunotherapy has been shown to improve the condition, and limited evidence suggests that daily low-dose aspirin can prevent lynch syndrome.
References
[1] Abu-Ghazaleh, N., Kaushik, V., Gorelik, A., Jenkins, M., & Macrae, F. (2022). Worldwide prevalence of Lynch syndrome in patients with colorectal cancer: Systematic review and meta-analysis. Genetics in Medicine, 24(5), 971-985
[2] Idos, G., & Valle, L. (2021). Lynch syndrome.
[3] hao, S., Chen, L., Zang, Y., Liu, W., Liu, S., Teng, F., … & Wang, Y. (2022). Endometrial cancer in Lynch syndrome.International Journal of Cancer,150(1), 7-17.
[4] Rasmussen, M., Lim, K., Rambech, E., Andersen, M. H., Svane, I. M., Andersen, O., … & Therkildsen, C. (2021). Lynch syndrome-associated epithelial ovarian cancer and its immunological profile.Gynecologic Oncology,162(3), 686-693.
[5] Miller, J. D., Lew, C. R., Lillehaugen, T., & Thiel, E. (2023). EPH130 Association of Lynch Syndrome with Skin Cancer: An Exploratory Analysis Using Claims Data.Value in Health,26(6), S187.
[6] Zhong, C. S., Horiguchi, M., Uno, H., Ukaegbu, C., Chittenden, A., LeBoeuf, N. R., … & Yurgelun, M. B. (2023). Clinical factors associated with skin neoplasms in individuals with Lynch syndrome in a longitudinal observational cohort.Journal of the American Academy of Dermatology,88(6), 1282-1290.
[7] Casper, M., Weber, S. N., Kloor, M., Müllenbach, R., Grobholz, R., Lammert, F., & Zimmer, V. (2013). Hepatocellular carcinoma as extracolonic manifestation of Lynch syndrome indicates SEC63 as potential target gene in hepatocarcinogenesis.Scandinavian journal of gastroenterology,48(3), 344-351.
[8] Zalevskaja, K., Mecklin, J. P., & Seppälä, T. T. (2023). Clinical characteristics of pancreatic and biliary tract cancers in Lynch syndrome: A retrospective analysis from the Finnish National Lynch Syndrome Research Registry.Frontiers in Oncology,13, 1123901.
[9] Jun, S. Y., Lee, E. J., Kim, M. J., Chun, S. M., Bae, Y. K., Hong, S. U., … & Hong, S. M. (2017). Lynch syndrome-related small intestinal adenocarcinomas.Oncotarget,8(13), 21483.
[10] Takamizawa, S., Morizane, C., Tanabe, N., Maruki, Y., Kondo, S., Hijioka, S., … & Okusaka, T. (2022). Clinical characteristics of pancreatic and biliary tract cancers associated with Lynch syndrome.Journal of Hepato‐Biliary‐Pancreatic Sciences,29(3), 377-384.
[11] Cho, H., Yamada, M., Sekine, S., Tanabe, N., Ushiama, M., Hirata, M., … & Sugano, K. (2021). Gastric cancer is highly prevalent in Lynch syndrome patients with atrophic gastritis.Gastric Cancer,24(2), 283-291.
[12] Lonati, C., Moschini, M., Simeone, C., Spiess, P. E., & Necchi, A. (2022). Lynch syndrome in urological practice: diagnosis, therapeutic strategies, and screening for upper tract urothelial carcinoma.Current Opinion in Urology,32(1), 40-47.
[13] Le, S., Ansari, U., Mumtaz, A., Malik, K., Patel, P., Doyle, A., & Khachemoune, A. (2017). Lynch Syndrome and Muir-Torre Syndrome: An update and review on the genetics, epidemiology, and management of two related disorders.Dermatology Online Journal,23(11).
[14] Duque, R. P., Santos, N., Freire, B., Oliveira, C. M., Mendes, J. M., Macedo, J. P., & Sampaio, F. (2024). An Unusual Case of Lynch Syndrome.Cureus,16(6).
[15] Li, B., Wang, Y., Wang, Y., Li, S., & Liu, K. (2022). Deep Infiltrating Endometriosis Malignant Invasion of Cervical Wall and Rectal Wall With Lynch Syndrome: A Rare Case Report and Review of Literature.Frontiers in Oncology,12, 832228.
[16] Azizi, A. H., Inam, Z. S., & Farrell, T. J. (2018). Patient with Lynch syndrome with subsequent development of small bowel adenocarcinoma.Case Reports,2018, bcr-2018.
[17] Edwards, P., & Monahan, K. J. (2022). Diagnosis and management of Lynch syndrome.Frontline Gastroenterology,13(e1), e80-e87.
[18] Abildgaard, A. B., Nielsen, S. V., Bernstein, I., Stein, A., Lindorff-Larsen, K., & Hartmann-Petersen, R. (2023). Lynch syndrome, molecular mechanisms and variant classification.British journal of cancer,128(5), 726-734.
[19] Li, X., Liu, G., & Wu, W. (2021). Recent advances in Lynch syndrome.Experimental hematology & oncology,10(1), 37.
[20] Latham, A., Srinivasan, P., Kemel, Y., Shia, J., Bandlamudi, C., Mandelker, D., … & Stadler, Z. K. (2019). Microsatellite instability is associated with the presence of Lynch syndrome pan-cancer.Journal of Clinical Oncology,37(4), 286-295.
[21] Tiernan, G., Freeman, V., Morrow, A., Hogden, E., Canfell, K., Kang, Y. J., & Taylor, N. (2022). What would I do? Perspectives on the factors underlying Lynch syndrome genetic testing and results sharing decisions for high‐risk colorectal cancer patients.Psycho‐Oncology,31(4), 587-596.
[22] Newton, K., Green, K., Lalloo, F., Evans, D. G., & Hill, J. (2015). Colonoscopy screening compliance and outcomes in patients with Lynch syndrome.Colorectal Disease,17(1), 38-46.
[23] Duraturo, F., Liccardo, R., De Rosa, M., & Izzo, P. (2019). Genetics, diagnosis and treatment of Lynch syndrome: Old lessons and current challenges.Oncology letters,17(3), 3048-3054.
[24] Williams, M. H., Hadjinicolaou, A. V., Norton, B. C., Kader, R., & Lovat, L. B. (2023). Lynch syndrome: from detection to treatment.Frontiers in Oncology,13, 1166238.
[25] Toh, J. W. T., Hui, N., Collins, G., & Phan, K. (2022). Survival outcomes associated with Lynch syndrome colorectal cancer and metachronous rate after subtotal/total versus segmental colectomy: Meta-analysis.Surgery,172(5), 1315-1322.
[26] Serrano, D., Patrignani, P., Stigliano, V., Turchetti, D., Sciallero, S., Roviello, F., … & Bonanni, B. (2022). Aspirin colorectal cancer prevention in Lynch syndrome: recommendations in the era of precision medicine.Genes,13(3), 460.