
, also known as intestinal polyposis-cutaneous pigmentation syndrome, is a rare inherited...){kind=link}

Peutz Jeghers Syndrome Peutz-Jeghers syndrome (PJS), also known as intestinal polyposis-cutaneous pigmentation syndrome, is a rare inherited disorder characterized by the development of hamartomatous polyps in the gastrointestinal (GI) tract and distinctive pigmented spots (mucocutaneous pigmentation) on the lips, mouth, fingers, and sometimes other areas of the skin. Hamartomatous polyps are unusual growths of the native cells (GIT, skin, etc.), lacking normal cell organization. The rare disease has an approximate prevalence of 1/50,000 to 1/200,000 people.[1] Moreover, the abnormal growths appear as dark-colored spots on different parts of the body.
Patients suffering from PJS have a higher risk of developing various types of cancers (an estimated 15-fold increased risk of intestinal cancer). As per reports, there is a 30.9% cancer risk in 40-year-olds suffering from Peutz-Jeghers, which rises to 76.2% by the age of 60. Therefore, cancer screening is very important, especially in older patients.[2] There is no definitive cure for the disease. However, doctors manage the polyps by surgically removing them.
Peutz-Jeghers Syndrome Symptoms: Peutz Jeghers Syndrome
The disease is characterized by the formation of polyps in the mucous membranes and spots on the skin. Generally, skin presentations are more frequently seen in children than in adults (where polyp-related symptoms are more common).
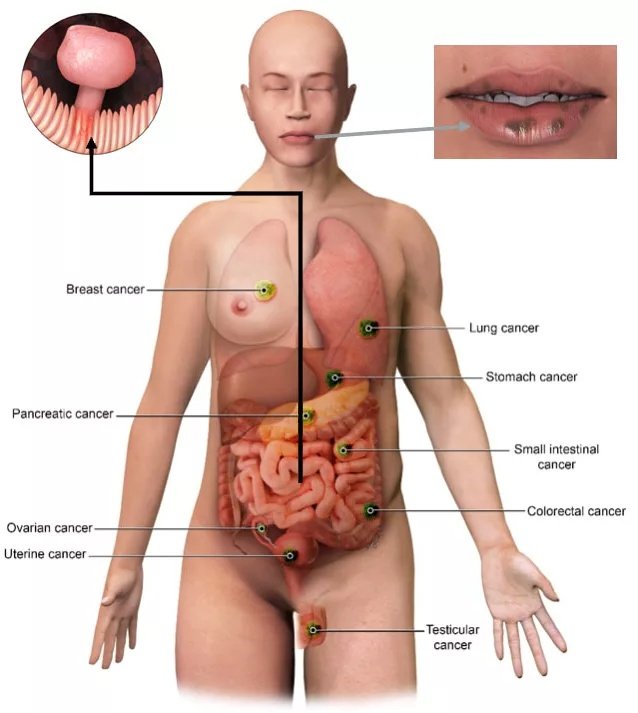
The illustration shows symptomatic presentations of Peutz-Jeghers syndrome. Attribution Klimkowski S, Ibrahim M, Ibarra Rovira JJ, Elshikh M, Javadi S, Klekers AR, CC BY 4.0 <https://creativecommons.org/licenses/by/4.0>, via Wikimedia Commons
Dermatological Presentations:
A common presentation of the inherited disorder in children is dark spots on the skin. The spots range in color from blue-gray to brown and appear within the first couple of years after birth. The noted average size of the spots ranges from 1 to 5 millimeters, and foci are oval/round-shaped. These hyperpigmented spots can resemble freckles when they form on the facial region. Common sites for skin spots are around.[3]:
- Face
- Eyes
- Nose
- Mouth (vermilion border of the lips)
- Hand fingers and palms
- Feet
- Orifices (anus)
Clinicians have also noted localized depigmentation in several cases, which led to the improper diagnosis of vitiligo. Many patients claim that the mucocutaneous hyperpigmented spots fade over time (after adolescence).
GI Disturbances:
Peutz-Jeghers syndrome affects the gastrointestinal tract, leading to GI-related symptoms. Manifestations of GI disturbance are generally seen during the first three decades of life (till 30 years of age). The mean age of GI symptom onset is 13 years. Common issues include:
Abdominal Pain
Imaging studies have helped clinicians in revealing the true nature of the disease. Not all patients report tummy aches. However, it is mostly adult individuals who suffer from nonspecific symptoms like abdominal pain. In one study, a 43-year-old presenting to the ER with abdominal pain was diagnosed with PJS-related intestinal polyps.[4]
Nausea & Vomiting
Several Peutz-Jeghers syndrome feel nauseous due to the disease. Nauseatic feeling may be accompanied by episodes of vomiting, indicating underlying problems with the GI tract. A 2022 study concluded that symptoms like colicky abdominal pain, oral pigmentations, and feelings of nausea/vomiting are indicative of hamartomatous polyps of PJS.[5]
A 32-year-old pregnant woman reported to the ER with complaints of diarrhea, abdominal colic (pain), nausea, and vomiting. Unfortunately, the patient lost her life in the hospital, and the autopsy report revealed multiple arborizing (branching) gastrointestinal polyps (mainly in the small intestine). Thus, indicating the possible severity of the disease too.[6]
Bleeding
Gastrointestinal bleeding is a presentation of the disorder. The blood is passed into the poop and makes the stool dark colored. A 5-year-old boy was admitted to the hospital with chief complaints of bloody stools, nausea, and stomach pain. Diagnostic studies revealed polyps in more than seven locations of the intestines. Therefore, scintigraphy (a diagnostic technique that uses radioactive material to visualize internal structures) revealed bleeding from the pylorus of the stomach, the upper part of the GI tract, the middle part of the colon, and the lower parts of the intestines.[7]
Anemia:
Chronic anemia is a usual outcome of large intestinal polyps. Excessive bleeding from the hamartomatous polyps causes anemia. There are scores of clinical studies that have found a relationship between anemia and hamartomatous polyps. In one such study, a patient suffered from chronic anemia due to solitary and giant PJS polyps.[8]
A 30-year-old female with PJS had primary symptoms of GI bleeding and anemia.[9] Thus, to prevent further falls in hemoglobin level, our doctors adopt different strategies to treat polyps. In a 2022 study, the laboratory analysis of a 53-year-old man revealed iron deficiency anemia with hemoglobin levels of 6.0 g/dL. Doctors performed double-balloon enteroscopy-assisted polypectomy to alleviate symptoms and improve Hb levels.[10]
Peutz-Jeghers Syndrome Causes
Nature has provided the human body with tumor suppressor genes that act as brakes to prevent the uncontrolled division of cells. These genes monitor the cell division process and remove abruptly divided cells to prevent tumor formations. However, these genes can stop functioning due to disorders.
A notable tumor suppressor gene is the SKT11 gene. Mutations in the SKT11 gene (in one copy) lead to the development of PJS. A study on a Chinese family with PJS revealed that haploinsufficiency of the SKT11 gene can contribute to the pathogenesis of the syndrome. Haploinsufficiency is a condition in which one (functional) copy of the gene is not sufficient for the maintenance of normal cell function, in this case SKT11 gene.[11]
The vast majority of patients develop the disease as a result of a faulty (mutated) gene passed from one of the parents. Around 70-80% of PJS patients have a family history of the disease. However, a small percentage (around 20-30%) don’t have a familial connection. While the exact cause of this development is unclear, many experts believe that all such individuals acquire a genetic mutation later in life.
Though rare, there have been cases of mutations in other genes as well that lead to PJS. Unique mutations are seen in the following genes:[12]
- TGFBR1
- BMPR1A
- ENG
Inheritance Pattern Of Peutz-Jeghers Syndrome:
Peutz-Jeghers syndrome is passed on to the offspring in an autosomal dominant pattern. This means that you get a single copy of the SKT11 gene from both parents. Optimal working of the body requires functional and normal genes from both parents. There is a high risk of Peutz-Jeghers syndrome if you receive even one copy of the mutated gene from either of your parents.
Similarly, you can pass on a mutated gene to your offspring. The chances of a child getting the disorder, if you have a mutation, are 50/50. Therefore, genetic counselling and timely genetic testing are crucial in preventing disease aggravation.
Peutz-Jeghers Syndrome Diagnosis
Diagnostic Criteria:
In the clinic/hospital, your doctor will take a complete history of the disease. He will ask you questions about questions of Peutz-Jeghers syndrome in immediate family members or relatives. After a thorough physical examination of the skin pigmentations and co-occurring abdominal pain, bloody stools, the doctor analyzes the patient according to the diagnostic criteria. The average age of PJS diagnosis is 23. Thus, we see more youngsters getting diagnosed with the syndrome than oldies. Clinicians reach a diagnosis if any of these criteria are met:
- There are more than 2 gastrointestinal hamartomatous polyps.
- Characteristic mucocutaneous hyperpigmented spots are present on the skin. It may involve any region, such as the facial skin or the skin of the fingers and genitals. The dermatological presentations are there with a family history of the syndrome.
- There are Peutz-Jeghers polyps (any number) in a patient with a relative (1st-degree) suffering from the condition.
- PJS polyps (any number) are present in conjunction with typical dark spots (pigments) associated with the syndrome.
Diagnostic Tests:
Genetic Testing
The primary diagnostic test for Peutz-Jeghers syndrome is genetic testing. It is considered the most reliable test in patients presenting with dermal pigmentation and GIT polyps. A doctor takes a sample from your body to extract the DNA. Samples can be taken from your blood, saliva, or cheek (swab test).

Genetic testing is a frequently adopted lab test for genetic disorders.
The sample is then sent to the laboratory for testing, where technicians extract the DNA and analyze it using different types of testing, like molecular testing, biochemical testing, and cytogenetic testing.[13] The lab identifies which genes have undergone mutations.
Endoscopic Evaluations
Physicians adopt different types of endoscopic tests to visualize and analyze gastrointestinal structures. Common endoscopic procedures for Peutz-Jeghers syndrome include:
- Colonoscopy: A Diagnostic colonoscopy is done by inserting a flexible tube with a camera into the intestines.
- Upper endoscopy: It is a similar process to colonoscopy to examine the upper structures of the GIT, including the stomach, esophagus, and the duodenum (beginning region of the small intestine). The tube/camera is inserted via the mouth.
- Capsule endoscopy: It is an advanced type of endoscopy procedure where the patient swallows a tiny capsule containing a camera. The camera captures images of the digestive tract and provides valuable information regarding the gastrointestinal tract. It has proven benefits in estimating polyp size and other details.[14]
CT/MRI Enteroscopy
It is a non-invasive diagnostic procedure that uses a contrast material to visualize the inside of the small intestine. A Computerized Tomography scan or an MRI scan of the intestines and abdominal structures helps diagnose jejunal intussusception in PJS patients.[15]
Doctors can also remove a part of the polyp growth for a biopsy. This is done when cancer is suspected.
Differential Diagnosis:
Peutz-Jeghers Syndrome Vs Hereditary Hemorrhagic Telangiectasia (HHT)
Peutz-Jeghers can have HHT-like symptoms, but there are certain differences between the two disorders. While PJS presents with dark spots, GI tract polyps, and increased risk of cancers, HHT causes recurrent nose bleeds due to blood vessel dilations (telangectasias). PJS arises due to a mutation in the SKT11 gene, but HHT is the result of genetic mutations in the ALK1 or ENG genes.
Peutz-Jeghers Syndrome Treatment
Polypectomy, i.e., surgical removal of the polyps, is the most frequently adopted treatment strategy in PJS patients. Surgical intervention is indicated in cases where symptoms are significant or complications like bleeding, intussusception, or bleeding are expected.
Endoscopic polypectomy is a minimally invasive procedure in which doctors remove small, accessible polyps. This procedure involves a diagnostic endoscope with surgical instruments to cut the polyps. Clinical studies show that endoscopic treatment is a feasible option in the treatment of PJS-associated polyps and serves to be a good alternative to laparotomy in patients.[16]
Healthcare providers adopt different diagnostic and therapeutic procedures, like small-intestine endoscopy and balloon-assisted endoscopy (BAE), to treat symptoms like bleeding, obstruction, and intussusception caused by hamartomatous polyps.[17] Balloon-assisted endoscopy uses a balloon to widen the intestinal wall (via inflation and deflation of a balloon) to allow insertion of an endoscopic tube and surgical instruments.
In selected cases, segmental resection of the small or large intestine may be required if large or numerous polyps cannot be safely removed endoscopically or if there is suspicion of malignancy. Rarely, a prophylactic colectomy may be considered, though most management is focused on regular surveillance rather than extensive surgery.
Peutz-Jeghers Syndrome Complications
There are several complications associated with this genetic syndrome.
Cancers:
The greatest complication of Peutz-Jeghers syndrome is cancer development. As per studies, the median age of cancer diagnosis in patients was 45 years.[18] Cancers developing due to genetic mutations have a high rate of morbidity and mortality.
As expected, the hamartomatous polyps of the colon tend to convert into malignancies. Thus, gastrointestinal cancers are the most common cancers that develop due to faulty tumor suppressor genes.[19] In addition to intestinal carcinomas, patients are at a very high risk of breast, genitourinary, and lung cancers.
Intestinal polyposis-cutaneous pigmentation syndrome greatly increases breast cancer risk. Thus, doctors advise breast surveillance in all PJS patients.[20] Other types of cancers seen in such patients include:
- Pancreatic cancer
- Ovarian cancer
- Uterine cancer
- Cervical cancer
- Testicular cancer
- Stomach cancer
Intestinal Obstruction & Intussusception:
Bowel obstruction is an outcome of giant intestinal polyps. This blockage of the intestine often occurs due to a process called intussusception. It is a serious condition in which a section of the intestine lodges (or slides) into a neighboring intestine segment. This leads to blockage of food and fluids, which can cut off the blood supply. It presents with gastric symptoms like abdominal pain, nausea/vomiting, and bloody stools.
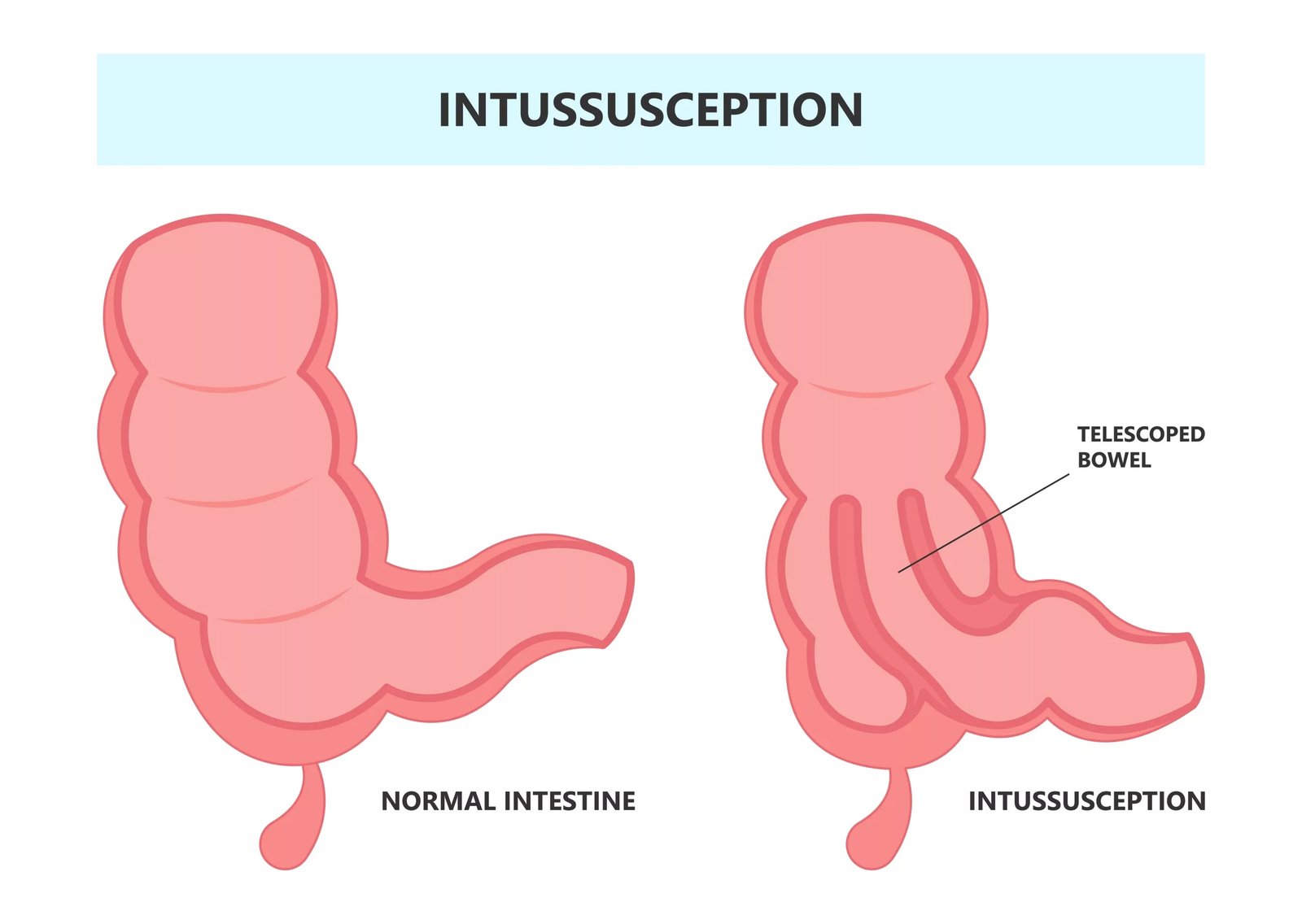
The lodging of one small intestine’s part into another part is known as intussusception and is a common complication of Peutz-Jeghers syndrome.
This complication is most commonly seen in younger patients. The intestinal obstruction due to intussusception can recur even after bowel resection. Therefore, doctors advise to properly follow up with patients properly.[21]
There may even be multiple intussusceptions in a patient, which are revealed in CT and MRI entrographies.[22]
Managing Peutz-Jeghers Syndrome
Genetic Counselling:
Unfortunately, there is no way to prevent the occurrence of this genetic disorder. However, doctors advise genetic counselling to patients with a familial history of SKT11 gene mutation. It informs the patients of the probability of their offspring getting the disease and keeps them aware of the possible complications.
Screenings:
The syndrome has a high risk of cancer development; all patients diagnosed with Peutz-Jeghers must undergo regular screenings to stay aware of any carcinogenic developments in the body. There is a variety of cancers that can arise due to PJS. Therefore, doctors advise multiple screening tests.
- CT/MRI enteroscopies should start at an early age (up to 10 years) and be repeated every 2-3 years if polyps are present. Doctors advise starting screening at the age of 18 and then following repeat screenings every 2-3 years if polyps are absent and the diagnosis is made on the basis of genetics.
- Upper endoscopy screening starts at 12 and is to be repeated annually in the presence of polyps and every 2-3 years in their absence. Endoscopic ultrasound is needed every 1-2 years, starting at 25 years of age.
- Women need to undergo annual breast exams, pelvic exams (and transvaginal ultrasounds) at ages 18-25 years, whereas men require testicular exams beginning at age 10.
Final Word
Peutz-Jeghers syndrome is a rare, genetic condition caused by a mutation in the STK11 gene (tumor suppressor gene), which leads to the formation of hamartomatous gastrointestinal polyps and dark spots on the skin. Transmitted to children in an autosomal dominant pattern, this syndrome presents with abdominal pain, bloody stools, nausea/vomiting, anemia, and brown-black hyperpigmented spots on facial skin. Symptoms mostly arise in young patients. It disposes patients to different types of cancers, including gastrointestinal, urinary tract, breast, and pancreatic cancers.
Clinicians diagnose PJS using genetic testing and visualize GIT structures with endoscopies and colonoscopies. Treatment involves removing polyps (polypectomy) with the help of therapeutic endoscopy. Complications of the syndrome include intestinal intussusception and cancer. Therefore, patients diagnosed with PJS need to undergo annual cancer screenings. Genetic counselling helps parents stay informed about the probability of disease in their children.
References
[1] Tacheci I, Kopacova M, Bures J. Peutz-Jeghers syndrome. Curr Opin Gastroenterol. 2021 May 1;37(3):245-254. doi: 10.1097/MOG.0000000000000718. PMID: 33591027.
[2] Wang, Z., Wang, Z., Wang, Y., Wu, J., Yu, Z., Chen, C., … & Chen, Y. (2022). High risk and early onset of cancer in Chinese patients with Peutz-Jeghers syndrome.Frontiers in Oncology,12, 900516.
[3] Nevozinskaya, Z., Korsunskaya, I., Sakaniya, L., Perlamutrov, Y., & Sobolev, V. (2019). Peutz-Jeghers syndrome in dermatology.Acta Dermatovenerol Alp Pannonica Adriat,28(3), 135.
[4] Klimkowski, S., Ibrahim, M., Ibarra Rovira, J. J., Elshikh, M., Javadi, S., Klekers, A. R., … & Elsayes, K. M. (2021). Peutz–jeghers syndrome and the role of imaging: Pathophysiology, diagnosis, and associated cancers.Cancers,13(20), 5121.
[5] Kalantari, M. E., Savadi, H., Sherafati, H., Bagherzadeh, A. A., & Zandbaf, T. (2022). Abdominal pain with oral pigmentations as a clue for Peutz-Jeghers syndrome.Frontiers in Emergency Medicine,6(4), e58-e58.
[6] Santos, V. M. D., Santos, L. A. M. D., & Modesto, L. C. (2022). Peutz-Jeghers syndrome: revisited.Autopsy and Case Reports,12, e2021384.
[7] Ermaya, Y. S., Rahmawanti, D., Rosalina, I., & Prasetyo, D. (2022). Clinical Manifestation of Peutz-Jeghers Syndrome in Children with Gastrointestinal Bleeding: A Case Report.Archives of Pediatric Gastroenterology, Hepatology, and Nutrition,1(1), 28-34.
[8] Rodriguez-Guzman, F., Ruas, J. N., CABRAL, J. G. G. D. A. L., Micelli-Neto, O., Venco, F. E., & Ardengh, J. C. (2023). Chronic anemia caused by giant and solitary Peutz-Jeghers hamartomatous polyp treated by endoscopic resection.Arquivos de Gastroenterologia,60(2), 282-284.
[9] Shakil, S., Aldaher, Z., & DiValentin, L. (2022). Peutz-Jeghers syndrome presenting with anemia: a case report.Cureus,14(7).
[10] Onuma, K., Sudo, G., Inoue, H., Kuriyama, T., Takada, Y., Yawata, A., & Nakase, H. (2022). Double-balloon enteroscopy-assisted polypectomy for a solitary jejunal Peutz–Jeghers polyp causing anemia.Endoscopy,54(S 02), E906-E907.
[11] Zhao, N., Wu, H., Li, P., Wang, Y., Dong, L., Xiao, H., & Wu, C. (2021). A novel pathogenic splice site variation in STK11 gene results in Peutz–Jeghers syndrome.Molecular Genetics & Genomic Medicine,9(8), e1729.
[12] Amru, R. L., & Dhok, A. (2024). Peutz-Jeghers Syndrome: A Comprehensive Review of Genetics, Clinical Features, and Management Approaches.Cureus,16(4).
[13] Aslan, P. G., Çağlayan, A. O., Bora, E., Koç, A., Yucel, H., Ülgenalp, A., … & Akarsu, M. (2024). Clinical and molecular analysis in patients with Peutz-Jeghers syndrome.The Turkish Journal of Gastroenterology,35(5), 374.
[14] Stewart, J., Fleishman, N. R., Staggs, V. S., Thomson, M., Stoecklein, N., Lawson, C. E., … & Attard, T. M. (2023). Small intestinal polyp burden in pediatric Peutz–Jeghers syndrome assessed through capsule endoscopy: a longitudinal study.Children,10(10), 1680.
[15] Cohen, E., Yuying, L., Brian, K. L., Alexandros, P., Kumta, N. A., Sands, B. E., & Lucas, A. L. (2022). S3424 Imaging-Negative Double Jejunal Intussusception Diagnosed on Laparoscopy With Intraoperative Enteroscopy in a Patient With Peutz-Jeghers Syndrome. The American Journal of Gastroenterology, 117(10S), e2161-e2161.
[16] Oguro, K., Sakamoto, H., Yano, T., Funayama, Y., Kitamura, M., Nagayama, M., … & Yamamoto, H. (2022). Endoscopic treatment of intussusception due to small intestine polyps in patients with Peutz-Jeghers Syndrome.Endoscopy international open,10(12), E1583-E1588.
[17] Yamamoto, H., Sakamoto, H., Kumagai, H., Abe, T., Ishiguro, S., Uchida, K., … & Nakayama, Y. (2023). Clinical guidelines for diagnosis and management of Peutz-Jeghers syndrome in children and adults. Digestion, 104(5), 335-347.
[18] van Lier, M. G., Westerman, A. M., Wagner, A., Looman, C. W., Wilson, J. P., De Rooij, F. W., … & Van Leerdam, M. E. (2011). High cancer risk and increased mortality in patients with Peutz–Jeghers syndrome.Gut,60(2), 141-147.
[19] Klimkowski, S., Ibrahim, M., Ibarra Rovira, J. J., Elshikh, M., Javadi, S., Klekers, A. R., … & Elsayes, K. M. (2021). Peutz–jeghers syndrome and the role of imaging: Pathophysiology, diagnosis, and associated cancers. Cancers, 13(20), 5121.
[20] Loehrer, E., Wagner, A., Bahar, M., Ramzan, F. R., Jelsig, A. M., Goverde, A., … & Latchford, A. (2025). The clinicopathological features of breast cancer in Peutz-Jeghers syndrome: results from an international survey.Familial Cancer,24(2), 41.
[21] Sreemantula, H. S., Joseph, C. A., Jamal, F., Agrawal, S., Thirumaran, R., Sreemantula, H. S., & Joseph, C. (2022). Intussusception caused by Peutz-Jeghers syndrome.Cureus,14(4).
[22] Boumeriem, K., Badr, K., Nabil, M. B., Ittimade, N., & Kaoutar, I. (2025). A case of multiple small bowel intussusceptions revealing a PEUTZ-JEGHERS syndrome.Radiology Case Reports,20(10), 5251-5254.