
, is a debilitating occupational disease in which the...){kind=link}

Phossy Jaw Symptoms Phossy jaw, also known as the phosphorus necrosis of the jaw (PNJ), is a debilitating occupational disease in which the jawbone progressively deteriorates. It was historically caused by long-term exposure to white (yellow) phosphorus, most often affecting workers in match factories during the 19th and early 20th centuries. Inhaling phosphorus fumes over time led to bone death (osteonecrosis) in the jaws, typically the mandible, but sometimes the maxilla as well.[1]
Poor oral hygiene and existing dental decay made workers more vulnerable, and the disease could progress to painful swelling, exposed bone, and foul-smelling discharge. Severe cases were often fatal, with mortality rates of about 20%, mainly due to infection and sepsis.[2] The discovery of red phosphorus led to the prohibition of white phosphorus in the industry. The first white phosphorus matches were produced in 1833, and the first reported PNJ case followed just five years later, in 1838. The condition quickly became a public and political issue.
Today, true phossy jaw is rare, but isolated cases may still occur from exposure to chemical weapons containing white phosphorus.[3] This occupational disease was largely eradicated after the ban on the use of white phosphorus in the matchstick-making industries.[4]
Etiology of Phossy Jaw: Phossy Jaw Symptoms
Phossy jaw results from chronic exposure to the vapors of white (yellow) phosphorus. When heated, white phosphorus vaporizes, and these fumes enter the body mainly through inhalation and to a lesser extent via mucosal absorption or contaminated food/water. The average time from the first exposure to the diagnosis was five years. This condition was most commonly observed in children, adults, and females who had worked up to 16 hours in match factories.[5]
Pathophysiology of Phossy Jaw
The pathophysiology involves loss of bone vitality followed by chronic inflammation and infection. The summary of the mechanism of the tissue damage that occurred in the phossy jaw includes:
- Workers involved in mixing, dipping, and boxing matches become exposed to white phosphorus fumes.
- The localized exposure produces a toxic chemical effect on the gingiva and the periosteum (the outer surface lining of the bone). Phosphorus causes direct necrosis of the bone, but the exact mechanism is unclear.
- The chemical injury leads to loss of blood supply and the death of bone cells, resulting in devitalized bone, which acts as a nidus for secondary bacterial infection, causing abscesses, pus formation, the formation of fistulas, and progressive bone destruction. The affected bone becomes porous, light, and irregular, with sequestra (dead bone fragments) surrounded by sclerotic areas. Unlike normal bone healing, osteonecrosis often fails to heal with treatment.
Overall, the pathophysiology reflects a combination of direct chemical toxicity from white phosphorus, causing bone necrosis and subsequent secondary bacterial osteomyelitis, resulting in progressive tissue destruction and clinical features of the phossy jaw.
Clinical Manifestations
Early symptoms usually start with a persistent toothache and gum swelling that gradually spreads to adjacent teeth and the jawbone. The pain is persistent and progressive.[6] In advanced cases, the necrotic bone may emit a greenish-white glow in the dark due to phosphorus oxidation (Phosphorescence). Chronic cases may rarely involve the central nervous system, causing headaches or seizures.[7]
Signs and symptoms vary according to the stage of the disease. There are three main stages of the phossy jaw.
Stage I:
This is the initial stage that begins with intermittent dental pain and gingival swelling. However, the patient remains healthy.
Stage II:
The disease progresses, and the signs of infection become prominent. The disease spread from the gums to the jawbone. Necrosis begins, and the exposed bone starts to appear. The symptoms of stage II phossy jaw include:
- Significant jaw swelling
- Severe and persistent pain in the jaw
- Development of abscesses
- Formation of a fistula
- Tooth loosening
- Loss of a tooth
- Foul-smelling discharge
- Exposed necrotic bone is starting to appear
Stage III:
This stage is marked by obvious necrosis. The jawbone starts to slough off, and it becomes significantly destroyed. The symptoms of this stage include:
- Exposed and visible necrotic bone in the mouth with foul odor
- Extensive tissue destruction
- Formation of sequestrum
- Severe facial disfigurement
- Persistent non-healing sores
- Continuous loss of teeth
- Potential systemic effects such as fever, malnutrition, and neurological complications.
Diagnosis of Phossy Jaw
The diagnostic methods of the condition involve:
Clinical Presentation & History:
The patient presents with chronic and progressive jaw pain, possible facial swelling, tooth loosening, and spontaneous exfoliation due to alveolar bone necrosis. They can also present with exposed necrotic bone, foul-smelling discharge, and non-healing ulcers or sinus tracts with secondary bacterial infections. The doctor can ask about your history of exposure to white phosphorus and when you were last exposed to it.
Radiographic Findings:
Doctors consider the following imaging modalities for diagnosing the condition:
Plain Radiography
X-rays show osteolytic lesions, sclerotic bone margins, periosteal reaction, and new bone formation in response to necrosis. It can also display a well-demarcated separation between dead and living bone, periosteal reactions, and chronic osteomyelitis (in chronic cases).[8]
Multislice Computed Tomography
Doctors can also request a CT scan for more accurate findings. It can help in visualizing the delineation of necrotic bone extent, soft tissue involvement, sinus tract formation, and other pathological features.
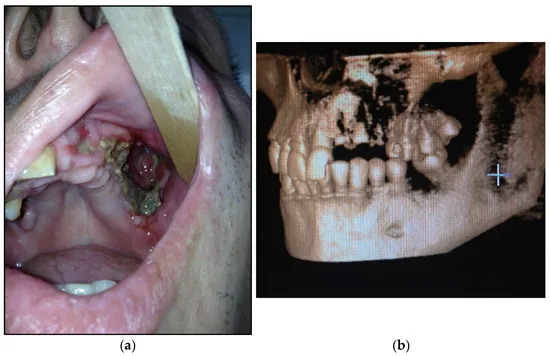
(a) Patient with type 1 toxic phosphorus osteonecrosis. Intraoral view; (b) CT-scan of the patient’s skull. Image courtesy: Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone by Ispiryan et al. 2023, https://doi.org/10.3390/dj11050108, available via https://www.mdpi.com/2304-6767/11/5/108, CC BY 4.0.

(a) Patient with severe toxic phosphorus osteonecrosis. Intraoral view; (b) multi-CT-scan of the patient’s skull before operation. Image courtesy: Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone by Ispiryan et al. 2023, https://doi.org/10.3390/dj11050108, available via https://www.mdpi.com/2304-6767/11/5/108, CC BY 4.0.
Magnetic Resonance Imaging
MRI shows bone marrow edema as an early sign and soft tissue abscess formation.
Elemental Analysis:
Scanning electron microscopy can also be employed to detect the phosphorus content in dental calculus. It is mainly used in forensic or archaeological research, not routine clinical care.[9]
Biopsy:
Doctors can also recommend a biopsy. The biopsy findings are necrotic bone lacking osteocytes, with surrounding inflammatory infiltrate and bacterial colonies. In advanced cases, dysplastic or malignant changes may be noted.
Treatment & Management of Phossy Jaw
The following strategies can help manage and treat the condition:
Immediate Cessation of Phosphorus Exposure:
Removal from occupational exposure is critical to reduce exposure and cease disease progression. Workers with early symptoms should undergo immediate medical evaluation.
Conservative Management:
Conservative management comprises:
- Local irrigation (chlorhexidine 0.2, saline solution, etc).[10]
- Systemic antibiotics in acute infections.
- Avoidance of irritants such as alcohol, tobacco, and the use of dentures.
- Instructions about oral hygiene.
- Gentle removal of sequestrum (from sequestrating lesions) without local anesthesia.
Healthcare providers may use HBO therapy or resection in cases of intractable pain or cases of failure in response to the conservative measures.[11]
HBO Therapy:
Hyperbaric oxygen (HBO) therapy promotes revascularization of damaged tissues. It improves fibroblast activity, supports angiogenesis, and reduces the extent of necrotic bone requiring surgical removal. Hence, HBO therapy also enhances tissue reconstruction and wound healing.
Surgical Management:
In severe or unresponsive cases, the following surgical options may be considered:
- Sequestrectomy (removal of necrotic bone)
- Segmental resection of the jaw if the disease is extensive
- Reconstruction with vascularized bone flaps (e.g., scapular-parascapular, iliac crest, fibular) to restore continuity and provide viable soft tissue coverage.[12]
Historic/Obsolete Treatments
In the 19th and early 20th centuries, reported treatments included gargles with potash or iodine, nitre mixtures, myrrh, flaxseed poultices, fresh air, nutritious diets, and application of leeches. Incisions were sometimes made to drain pus, and morphine was used for pain control.
Differential Diagnosis
Some other diseases which can be mistaken for phosphorus necrosis of the jaw include:
- Osteomyelitis (generally shows signs of infection that are not specific to chemical exposure)
- Osteoradionecrosis or radium jaw (linked to historical radium exposure)
- Osteopetrosis (Lacks a necrotic process and systemic features, a congenital bone disorder)
- Temporomandibular joint disorders (no bone necrosis or pus)
- Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ): Seen in patients receiving bisphosphonate therapy (commonly for osteoporosis, Paget’s disease, or metastatic bone lesions). Characterized by exposed, non-healing necrotic bone in the maxillofacial region, often after dental extractions or trauma. Unlike phossy jaw, BRONJ is not linked to chemical inhalation but to impaired bone remodeling from osteoclast inhibition.
Phossy Jaw versus Radium Jaw
Phossy jaw and radium jaw are both historic occupational diseases. They differ mainly in their causative agent, the affected population, and the pathological effects.
The key differences between the two are summarised in Table 1.
Table 1: Key Differences between Phossy and Radium Jaw
| Features | Phossy Jaw | Radium Jaw |
|---|---|---|
| Causative agent | Ingestion or absorption of white phosphorus. | Ingestion or absorption of radium. |
| Affected population | Matchstick workers | Radium dial painters and radium machine consumers. |
| Pathological effects | InflammationAbscessTooth lossSequestrumJawbone destruction | Bone degradationTumorsPorosityBone cancer |
| Symptoms | ToothacheAbscessesNecrosis of the mandibleJaw bone destruction | Necrosis of the maxilla and mandibleBleeding gumsSevere jaw distortionWeight lossTooth lossBody sorenessBone tumors |
| Treatment | Limited, often requires surgical removal of the jaw. | No effective treatment once advanced. |
Final Remarks
Phossy jaw was a devastating industrial disorder that affected workers exposed to white phosphorus fumes in poorly ventilated match factories. It begins with pain and ultimately results in the formation of an involucrum and necrotic bone. It causes facial disfigurement and can also be fatal. There was no cure before the emergence of antibiotics. Health legislation curbs the emergence of new cases.
References
[1] Hughes, J., et al., Phosphorus Necrosis of the Jaw: A Present-day Study: With Clinical and Biochemical Studies. Occupational and Environmental Medicine, 1962. 19(2): p. 83-99.
[2] Kamboj, M., Phossy jaws. British Dental Journal, 2007. 203(10): p. 559-559.
[3] Jacobsen, C., et al., The phosphorous necrosis of the jaws and what can we learn from the past: a comparison of “phossy” and “bisphossy” jaw. Oral and maxillofacial surgery, 2014. 18(1): p. 31-37.
[4] Myers, M. and J. McGlothlin, Matchmakers’ phossy jaw” eradicated. American Industrial Hygiene Association Journal, 1996. 57: p. 330-392.
[5] Kamboj, M., Phossy jaws. British Dental Journal, 2007. 203(10): p. 559-559.
[6] Campanacho, V., Phosphorus necrosis of the jaw: a review of an 19th and early 20th century occupational disease. 2020.
[7] Pollock, R.A., T.W. Brown Jr, and D.M. Rubin, “Phossy Jaw” and “Bis-phossy Jaw” of the 19th and the 21st centuries: the diuturnity of John Walker and the friction Match. Craniomaxillofacial trauma & reconstruction, 2015. 8(3): p. 262-270.
[8] Jacobsen, C., et al., The phosphorous necrosis of the jaws and what can we learn from the past: a comparison of “phossy” and “bisphossy” jaw. Oral and maxillofacial surgery, 2014. 18(1): p. 31-37.
[9] Campanacho, V., Phosphorus necrosis of the jaw: a review of an 19th and early 20th centuries occupational disease. 2020.
[10] Wong, J., R. Wood, and M. McLean, Conservative management of osteoradionecrosis. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 1997. 84(1): p. 16-21.
[11] Wong, J., R. Wood, and M. McLean, Conservative management of osteoradionecrosis. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 1997. 84(1): p. 16-21.
[12] Jacobsen, C., et al., The phosphorus necrosis of the jaws and what can we learn from the past: a comparison of “phossy” and “bisphossy” jaw. Oral and maxillofacial surgery, 2014. 18(1): p. 31-37.
For more information about Phossy Jaw Symptoms, refer to the latest medical literature.