
{kind=link}

Polyhydramnios Amniotic Fluid Polyhydramnios is characterized by an excess volume of amniotic fluid within the amniotic sac. Usually, a balance is maintained between amniotic fluid production and removal through fetal urination, lung fluid secretion, swallowing, and intramembranous absorption. Polyhydramnios occurs when this equilibrium is disrupted. The most common method of diagnosis is an abdominal ultrasound. The condition is often recognized accidentally in most patients during their ultrasonography evaluation for other reasons in their third trimester. The condition can be classified from mild to severe based on the size of the deepest vertical pocket (DVP) and amniotic fluid index (AFI). It occurs in 1 to 2% of all pregnancies. Based on severity, it is classified as mild, moderate, or severe. Around 65–70% of cases are mild, 20% are moderate, and 10–15% are severe.[1]
Etiology & Pathophysiology of Polyhydramnios: Polyhydramnios Amniotic Fluid
In approximately 50-60% of cases, the condition is idiopathic.[2] In other cases, it may result from a pathology that leads to excessive urine production, impairs fetal swallowing, and decreases fluid reabsorption from the gastrointestinal tract. Gestational diabetes is also an important cause. Less common causes of polyhydramnios include chromosomal abnormalities and intrapartum trans placental infections.
Excess Fetal Urine Production:
Fetal urination and fetal lung fluid produce amniotic fluid. The production of fetal urine typically occurs at a steady state. It increases as the pregnancy advances and the fetus grows. The approximate hourly fetal urine production rate for fetuses at 40 weeks is approximately 27–52 mL/hour.[3] However, the rate is typically low in growth-restricted fetuses and high in larger fetuses.[4]
Excessive production of fetal urine is generally due to maternal diabetes. Glucose freely crosses the placenta, and maternal hyperglycemia leads to osmotic diuresis and fetal hyperglycemia. Macrosomic fetuses (a fetus with a considerable birth weight) tend to produce more urine even in non-diabetic pregnancies. Rarely, excessive urine production is linked to conditions such as severe fetal anemia (e.g., parvovirus B19 infection, hemolytic disorders, alpha-thalassemia) or arteriovenous shunting leading to high-output cardiac failure. Certain renal and urological disorders, such as Bartter syndrome, can also result in severe polyhydramnios.[5] Bartter syndrome is an autosomal recessive condition. It affects fetal renal tubular function, causing sodium loss and polyuria, which leads to severe polyhydramnios.
Impaired Gastrointestinal Absorption & Fetal Swallowing:
Absorption of fluid occurs through fetal swallowing (direct absorption via fetal membranes also plays a role). Just as urine production increases, fetal swallowing also increases as pregnancy progresses. The approximate amount of swallowed amniotic fluid by the fetus is 500 to 1000 mL per day.[6] Impaired fetal gastrointestinal tract occurs due to:
- Duodenal Atresia: A congenital disability in which part of the duodenum is missing or blocked. The missing part prevents fluid and food from passing from the stomach into the intestines.
- Esophageal Atresia: A birth defect in which the esophagus is not fully formed.
- Tracheoesophageal Fistula: An anomalous connection between the trachea and the esophagus.
- Diaphragmatic Hernia: A congenital disability in which there is a hole in the diaphragm.
- Thoracic Mass: An abnormal growth in the chest cavity.
These conditions significantly limit the absorption of amniotic fluid, ultimately leading to polyhydramnios.
Swallowing increases with the increase in amniotic fluid. This is the vital component of amniotic fluid regulation. Additionally, the hypotonic nature of the fluid compared to the isotonic fetal plasma creates an osmotic gradient. This gradient enables the direct absorption of the fluid into the fetal vessels on the surface of the placenta (intramembranous absorption).[7]
Several central nervous system, neuromuscular, and craniofacial conditions may interfere with swallowing, such as:
- Lesions of the Central Nervous System: Abnormally developed tissues in the brain or spinal cord.
- Neuromuscular Dysfunction: These include arthrogryposis syndrome (a group of conditions characterized by multiple joint contractures present at birth) or myotonic dystrophy.
- Craniofacial Abnormalities: These include cleft lip or cleft palate, obstructive neck masses, and micrognathia (lower jaw smaller than normal size).
Symptoms of Polyhydramnios
Most women with polyhydramnios, particularly mild cases, are asymptomatic. When symptoms do occur, usually in moderate to severe cases, they may include:
- Abdominal enlargement with a rapid increase in belly size, making the uterus larger than expected for gestational age
- Sudden abdominal pain
- Tightness or discomfort in the stomach. It can be due to the stretched uterus
- Indigestion and constipation
- Shortness of breath or difficulty in breathing
- Swollen legs, feet, and ankles due to fluid retention
- Increased frequency of urination due to bladder compression
- Urinary tract infections (UTIs)
- Uterine contractions that mimic preterm labor.
- Abnormal fetal positioning (e.g., breech or transverse lie)
Diagnosis of Polyhydramnios
In general, this condition is detected during an ultrasonography performed for another indication or when the symphysis-fundal height is greater than expected for the gestational age. In such situations, the pregnant women are often asymptomatic.
History & Physical Examination:
Doctors obtain a focused medical and prenatal history to assess patients for signs, risk factors, and symptoms related to underlying etiologies. They may evaluate for:
- Features of impaired glucose tolerance (gestational diabetes)
- Congenital infections (e.g., history of febrile illness with rash or sick contacts)
- Risk factors for alloimmunization (Rh-negative blood types, blood transfusions, and history of bleeding in pregnancy).
Doctors can also ask the patient about:
- Their perception of fetal movements (limited movement of the fetus suggests a muscular disorder in the fetus).
- Uterine contractions
- Abdominal pain
- Cramping
- Vaginal bleeding
- Loss of fluid (suggestive of membrane rupture)
In patients with severe disease, physical examination can reveal:
- Lower extremity edema
- Dyspnea from diaphragmatic pressure
- Grossly distended abdomen
A fundal height above 3 cm for the gestational age in weeks and a rapid enlargement of the uterus warrant sonographic assessment.
Ultrasonography:
Ultrasound measurement of the amniotic fluid volume is the most reliable diagnostic method for polyhydramnios. The two common methods of assessing the amniotic fluid volume include:
Amniotic Fluid Index:
It measures the maximum vertical depth of fluid in four quadrants of the uterus and then sums these measurements. If the amniotic fluid index is 24 cm or greater, it indicates the presence of polyhydramnios.[8] The condition can be classified from mild to severe according to the amniotic fluid index:
- Mild polyhydramnios: 24 to < 30 cm.
- Moderate polyhydramnios: ≥ 30 to 35 cm
- Severe polyhydramnios: ≥ 35 cm[9]
Maximum Vertical Pocket:
A single largest pocket of fluid is measured.
- Normal: 2–7.9 cm
- Mild: 8–11 cm
- Moderate: 12–15 cm
- Severe: ≥ 16 cm[10]
The healthcare provider places the ultrasound transducer perpendicular to the floor, scanning in the sagittal plane parallel to the fetal spine to ensure accuracy.
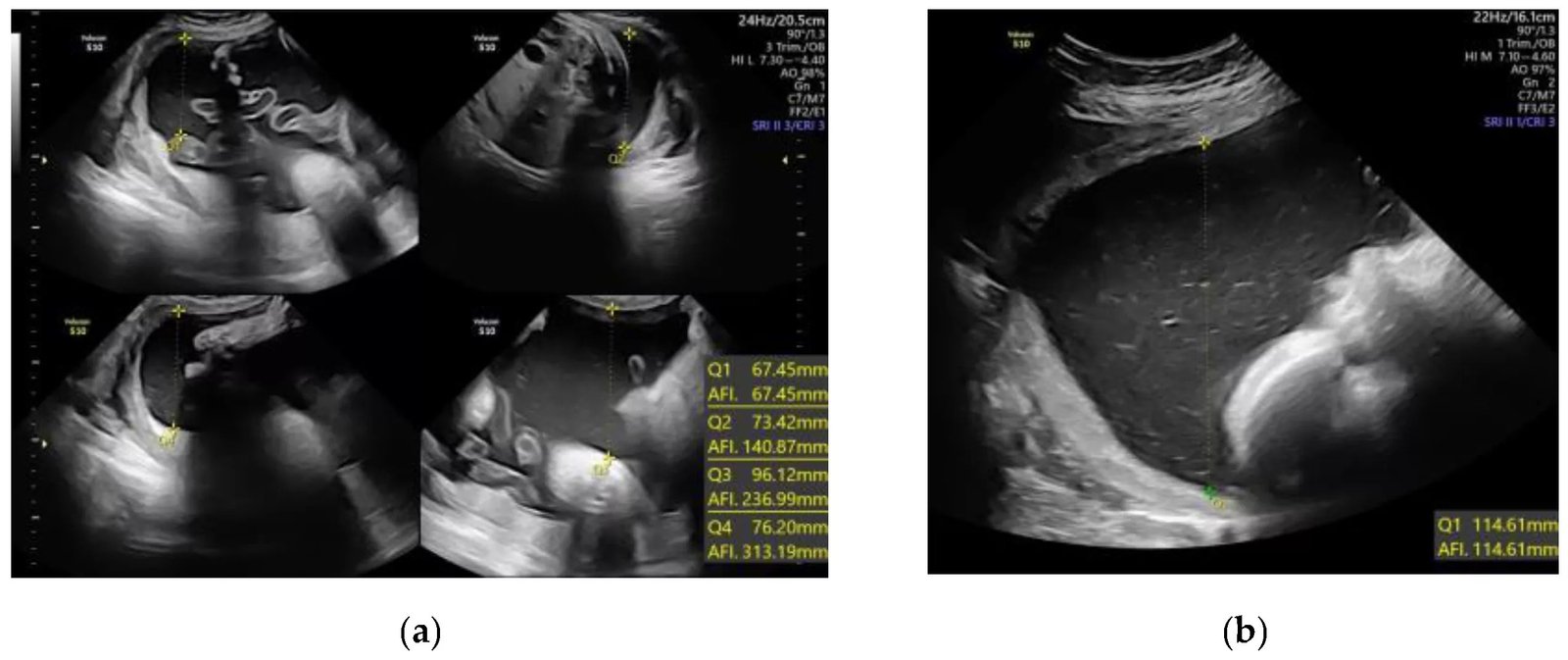
Amniotic fluid volume determination using quantitative sonographic techniques: (a) Amniotic fluid index (AFI); (b) single deepest pocket (SDP). Image Courtesy: Transient Polyhydramnios during Pregnancy Complicated with Gestational Diabetes Mellitus: Case Report and Systematic Review by Preda et al. 2022, doi.org/10.3390/diagnostics12061340, available via https://www.mdpi.com/2075-4418/12/6/1340, CC BY 4.0.
After the diagnosis is confirmed, an evaluation is generally performed to identify the underlying cause of the condition. This process starts with reviewing the prenatal record and obstetric ultrasound.
Screening for Underlying Etiologies:
- Genetic testing (karyotype or microarray via amniocentesis) is indicated if ultrasound findings suggest chromosomal abnormalities such as trisomy 13, 18, or 21.[11]
- Gestational diabetes should be excluded in all cases.
- In monochorionic-diamniotic twin pregnancies, serial ultrasound screening for twin-twin transfusion syndrome is recommended every 2 weeks starting at 16 weeks of gestation.
- Serum testing for congenital infections (TORCH, parvovirus B19) may be appropriate.[12]
Targeted Obstetric Ultrasound:
It is performed to assess the common structural causes of the excess amniotic fluid. According to SMFM, it should assess the fetus for the conditions associated with polyhydramnios, such as:
- Fetal hydrops
- Fetal growth abnormalities
- Specific structural abnormalities
- Arteriovenous shunting leading to high-output cardiac failure
- Neurological dysfunction is assessed by assessing major CNS structures and fetal movements..
Management & Treatment of Polyhydramnios
Management typically depends on the severity and underlying cause of the condition. Mild, idiopathic polyhydramnios is often expectantly managed without specific treatment. Symptomatic moderate to severe disease may benefit from intervention.
Surveillance & Monitoring:
Antepartum fetal surveillance is reasonable for moderate to severe polyhydramnios or when additional risk factors are present. Surveillance commonly uses a nonstress test with a modified or complete biophysical profile (BPP).
Repeat ultrasound is appropriate if new symptoms develop or if there is concern for progression. Serial scans typically assess amniotic fluid volume and fetal growth (both macrosomia and growth restriction can be seen in this setting).
Amnioreduction:
Doctors consider amnioreduction for patients with severe conditions. It is an ultrasound-guided method that eliminates amniotic fluid through a large transabdominal needle (a 15 cm, 20-gauge needle).[13] This procedure removes 1.5 to 3 litres of fluid, and most patients require more than one treatment. However, amnioreduction is not appropriate for asymptomatic individuals.
In cases where polyhydramnios is associated with twin–twin transfusion syndrome (TTTS), treatment strategies differ. The underlying issue in TTTS is abnormal vascular connections between the twins’ placentas, not just fluid overload. While amnioreduction may temporarily improve symptoms, it does not correct the root cause. For this reason, selective fetoscopic laser photocoagulation (SFLP) has become the preferred treatment in severe TTTS. This minimally invasive procedure seals abnormal placental vessels, addressing the underlying pathology. The Society for Maternal–Fetal Medicine (SMFM) recommends SFLP for patients with stage II to IV TTTS before 26 weeks of gestation.[14]
Indomethacin:
Indomethacin (a prostaglandin synthase inhibitor) decreases the amniotic fluid volume, fetal urine output, and uterine irritability in preterm patients. However, because of fetal risks, particularly ductus arteriosus constriction, oligohydramnios, and neonatal complications, its use is generally avoided after 32 weeks and, if considered earlier, is short-course with close fetal ductal monitoring. Tocolytics such as nifedipine or terbutaline may be chosen to treat contractions when needed, but they do not treat the excess fluid itself.[15]
Follow-up & Delivery Planning:
In mild to moderate cases without complications, aim for delivery at 39 to 40 weeks; however, severe cases may require early delivery. The mode of delivery depends on the obstetric ultrasound indications. Careful monitoring of the fetus during labour is advised in moderate to severe cases. Cesarean section can be common due to fetal malposition. With significant polyhydramnios, controlled amniotomy is prudent to reduce the risk of cord prolapse and placental abruption.
Patient & Neonatal Post-delivery Care:
The neonatal team must be present during the delivery. Doctors recommend careful evaluation of babies born after polyhydramnios pregnancies for gastrointestinal anomalies and other congenital conditions. A nasogastric tube is often passed before the first feed to check for tracheoesophageal fistula and esophageal atresia.
Differential Diagnosis & Prognosis of Polyhydramnios
When the pregnant females have a large abdomen that is larger than their gestation age, then the differential diagnosis includes:
- Multiple gestations
- Macrosomia
- Incorrect gestational dating
- Placental abruption
- Molar pregnancy
- Large tumors (e.g., ovarian or uterine)
- Maternal volume overload (rare; due to cirrhosis, preeclampsia, or heart failure)
The prognosis for mild disease is excellent. People with mild conditions usually have a self-limited disease that resolves without any intervention. The maternal and fetal prognosis worsens as the severity of the disease increases. For a fetus, the prognosis directly depends on the underlying cause of the condition. A growth-restricted fetus with polyhydramnios and underlying pathology tends to have a poor prognosis. Rapidly progressive and severe polyhydramnios is an independent risk factor for perinatal mortality.[16]
Complications of Polyhydramnios
Polyhydramnios is associated with a higher incidence of the following conditions:
- Fetal macrosomia
- Fetal malpresentation
- Cord prolapse
- Placental abruption
- Preterm labor
- Cesarean birth
- Shoulder dystocia
- Postpartum hemorrhage
- Perinatal mortality
Polyhydramnios versus Oligohydramnios
Both conditions involve fluctuations in the amniotic fluid, and the distinction between these two conditions is crucial for fetal surveillance and appropriate maternal care during pregnancy. The key differences are summarized in Table 1.
Table 1: Differences Between Polyhydramnios and Oligohydramnios
| Features | Polyhydramnios | Oligohydramnios |
|---|---|---|
| Definition | An abnormally high amount of amniotic fluid during pregnancy. | An abnormally low amount of amniotic fluid during pregnancy. |
| Deepest Pocket Measurement | <2cm | >8 cm |
| Amniotic Fluid Index | AFI >18–25cm (mild: 25–30cm, severe >35cm | AFI <5–7 cm17Hamza, A., et al., Polyhydramnios: causes, diagnosis and therapy. Geburtshilfe und Frauenheilkunde, 2013. 73(12): p. 1241-1246. |
| Causes | Maternal diabetes mellitusFetal anemiaMultiple gestationsImpaired fetal swallowingFetal infections | Post-term pregnancyPremature rupture of membranesMaternal health conditionsUteroplacental insufficiencyFetal urinary tract anomalies |
| Maternal symptoms | Often asymptomaticAbdominal distention and discomfortRespiratory distressPreterm labour symptoms | Often asymptomaticDecreased fetal movement |
| Complications | Cord prolapseMacrosomiaPlacental abruptionPreterm labour and deliveryIncreased risk of fetal anomalies, etc. | Cord compressionFetal growth restrictionIncreased risks of cesarean deliveryPulmonary hypoplasiaLimb contractures, etc. |
| Management | Monitoring, amnioreduction and treatment of the underlying cause. | Close monitoring and animofusion. |
Visual Difference between Polyhydramnios versus Oligohydramnios.
Final Remarks
Poluhydramnios is an abnormal increase in the amniotic fluid. It carries a high risk of adverse pregnancy outcomes. It requires additional antepartum, intrapartum, and postpartum care. Mostly, patients have mild, idiopathic disease that can be managed by an obstetrician, family medicine physician, or even a midwife. However, in severe forms, it is essential to consult with an interprofessional team. Coordinated care and efficient communication among the interprofessional team members are keys to a successful diagnosis and management of polyhydramnios.
References
[1] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[2] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[3] Fägerquist, M., et al., Fetal urine production and accuracy when estimating fetal urinary bladder volume. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 2001. 17(2): p. 132-139.
[4] Seol, H.-J., et al., Hourly fetal urine production rate in isolated oligohydramnios at term. PloS one, 2021. 16(5): p. e0250659.
[5] Luo, Q.-Q., et al., Idiopathic polyhydramnios at term and pregnancy outcomes: a multicenter observational study. The Journal of Maternal-Fetal & Neonatal Medicine, 2017. 30(14): p. 1755-1759.
[6] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[7] Wang, S., et al., Expression of aquaporin 9 in human chorioamniotic membranes and placenta. American journal of obstetrics and gynecology, 2004. 191(6): p. 2160-2167.
[8] Dashe, J.S., et al., Hydramnios: anomaly prevalence and sonographic detection. Obstetrics & Gynecology, 2002. 100(1): p. 134-139.
[9] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[10] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[11] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[12] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[13] Erfani, H., et al., Amnioreduction in cases of polyhydramnios: Indications and outcomes in singleton pregnancies without fetal interventions. European Journal of Obstetrics & Gynecology and Reproductive Biology, 2019. 241: p. 126-128.
[14] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[15] Hwang, D.S., S.M. Jenkins, and H. Mahdy, Polyhydramnios, in StatPearls [Internet]. 2024, StatPearls Publishing.
[16] Pilliod, R.A., et al., The risk of fetal death in nonanomalous pregnancies affected by polyhydramnios. American journal of obstetrics and gynecology, 2015. 213(3): p. 410. e1-410. e6.
[17] Hamza, A., et al., Polyhydramnios: causes, diagnosis and therapy. Geburtshilfe und Frauenheilkunde, 2013. 73(12): p. 1241-1246.