
{kind=link}

Pseudomembranous Colitis Antibiotics If you develop severe diarrhea after taking antibiotics, your doctor may mention a condition called pseudomembranous colitis. The name can sound intimidating at first. The reassuring news is that with the right information and timely treatment, this condition is usually manageable, and recognizing the warning signs early can make a significant difference.
What Is Pseudomembranous Colitis?: Pseudomembranous Colitis Antibiotics
Pseudomembranous colitis (PMC), sometimes informally referred to as Pseudomas colitis, is a severe inflammation of the inner lining of the large intestine (colon) that most commonly occurs due to infection with the bacterium Clostridioides difficile (C. diff). The condition gets its name from the pseudomembranes, which are yellowish-white plaques that develop on the surface of the colon during the disease.[1]
In simple terms, it is a serious inflammation of the inner lining of the large intestine (the colon). When the colon becomes severely inflamed, the immune system responds by sending large numbers of white blood cells to fight the infection. This process produces patches of plaque-like material of yellowish-white color on the colon wall.
These patches are the pseudomembranes. They consist of fibrin (a clotting protein), mucus, dead epithelial cells, bacteria, and inflammatory immune cells. They are not actual membranes produced by the body, which is why they are called pseudo (false) membranes.
The condition can range from mild to life-threatening. In severe cases, it may lead to complications such as toxic megacolon, bowel perforation, sepsis, or dangerously low blood pressure.
Clostridium Difficile and Pseudomembranous Colitis: The Primary Relationship
Clostridioides difficile (also known as C. diff), a bacterium, is the cause of the vast majority of cases of pseudomembranous colitis.[2]
C. diff is a gram-positive, spore-forming anaerobic bacterium. Spores are essentially a resistant and dormant variant of bacteria. They are able to survive on the surface, soil, animal feces, and unwashed hands over remarkably long periods of time. Once they get into the digestive tract, they start working once again and may lead to a severe infection.
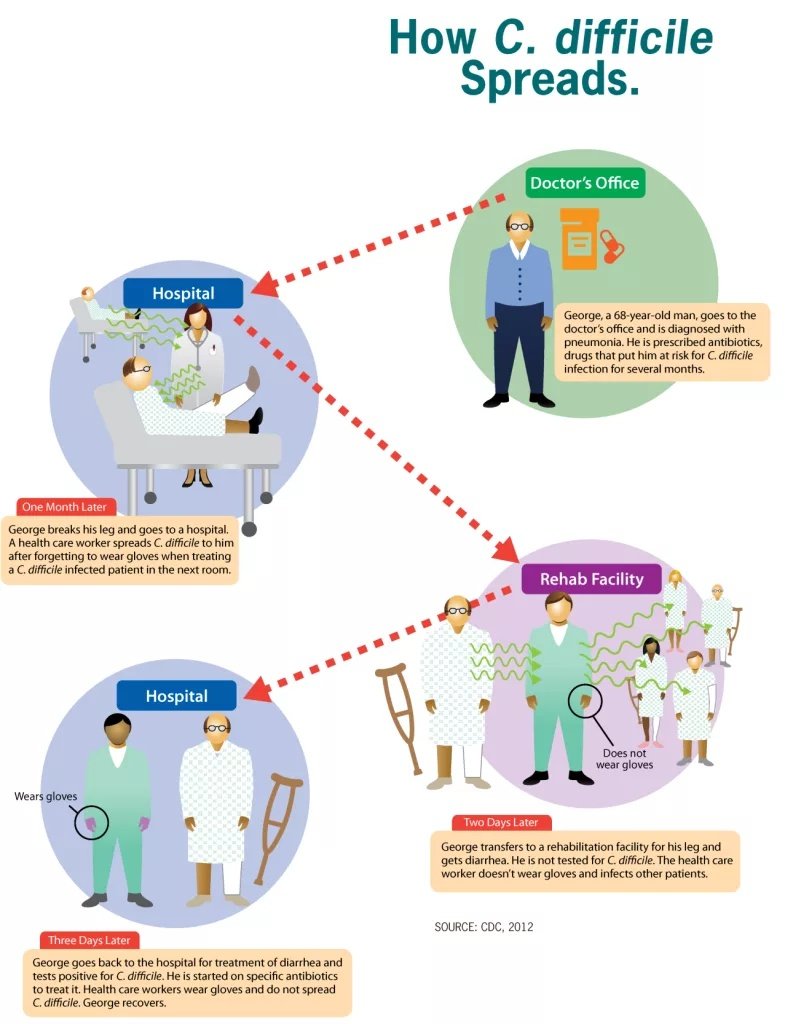
How Clostridioides difficile spreads in healthcare environments. Image credit: Centers for Disease Control and Prevention (CDC), 2012.Public Domain.
When the gut is healthy, it is usually inhabited by hundreds of different bacteria that coexist in a healthy manner. This equilibrium ensures that a particular species does not become too large. However, when this balance is disrupted, C. diff takes advantage of that. It reproduces quickly and causes two potent toxins to be received into the colon: Toxin A (enterotoxin) and Toxin B (cytotoxin). These toxins directly strike the colon wall. They destroy cells lining the colon, interfere with tight cell junctions, cause an exaggerated inflammatory reaction, and cause cell death. The outcome is the typical, swollen, pseudomembrane-coated colon, which is observed in this state.
It is estimated that C. diff causes more than 90% of pseudomembranous colitis cases, and in the United States alone, it leads to over 250,000 infections each year, making it a major healthcare-associated infection.[3]
Less Common Causes
Although C. diff is the culprit that heads the list, it is not the sole one. Other causes include:[4]
- Staphylococcus aureus and Klebsiella oxytaca
- Cytomegalovirus (CMV), Coronavirus
- Ischemic colitis
- Serious exacerbations in inflammatory bowel disease
- Certain chemotherapy drugs
- Heavy metal poisoning
- Some less common causes are Salmonella, Shigella, Campylobacter, and parasites such as Entamoeba histolytica.
Role of Antibiotics in Pseudomembranous Colitis
This is where the relationship between antibiotics and pseudomembranous colitis becomes somewhat paradoxical: antibiotics are the main trigger of the disease, but they are also the main treatment for it.
When someone takes a broad-spectrum antibiotic, the medication will not distinguish between the bad and the good bacteria. It eliminates masses of the normal gut bacteria. C. diff spores are naturally resistant to many antibiotics. Without the competition, it grows exponentially and colonises the colon.[5]
Not all antibiotics are equally dangerous. The following table summarizes the most frequently used antibiotics that are related to the development of pseudomembranous colitis:
| Antibiotic Class | Common Examples | Risk Level |
|---|---|---|
| Lincosamides | Clindamycin | Highest (up to 10% risk) |
| Penicillins | Ampicillin, Amoxicillin | High |
| Cephalosporins | Cefazolin, Ceftriaxone | High (most frequent due to wide use) |
| Fluoroquinolones | Ciprofloxacin, Levofloxacin | High |
| Carbapenems | Imipenem, Meropenem | Moderate |
| Macrolides | Azithromycin | Lower, but still possible |
Almost any antibiotic can potentially trigger C. diff infection, even when used for a short duration. In some cases, the condition has developed after a single prophylactic antibiotic dose before surgery.
This does not mean antibiotics should be avoided when they are necessary. It simply emphasizes that they should be used only when medically appropriate and under professional supervision.
Who is at Risk?
Pseudomembranous colitis may occur in anybody, though some populations are highly susceptible. Individuals at the greatest risk of getting this condition are:[6]
- Adults over the age of 65
- Patients who are in hospitals or nursing homes
- Anyone who has recently used antibiotics
- Patients who have undergone gastrointestinal surgery
- Individuals who are receiving chemotherapy due to cancer
- People who have a compromised immune system (HIV, organ transplants, autoimmune diseases, and so on)
- Individuals who had an infection of C. diff before
- Patients in the hospital who are on tube feeding
C. diff is rare in normal children and even more so in infants, even though a surprisingly large proportion (up to 50% ) of infants can harbour the bacteria in their gut without becoming ill.
Pseudomembranous Colitis Symptoms
Recognizing the symptoms early is important because prompt treatment can prevent serious complications.
Symptoms usually appear during antibiotic treatment or within a few days to several weeks after completing it, although they may sometimes develop up to 8–10 weeks later.[7]
Common symptoms include:
- Signs of dehydration, such as dry mouth, dizziness, or reduced urination.
- Watery diarrhea, often frequent and sometimes exceeding 10 episodes per day
- Abdominal pain and cramping
- Fever
- Nausea
- Blood or pus in the stool
In mild to moderate cases, the only symptom is diarrhea. In extreme situations, the image is very different. Excessive diarrhea, high fever, marked leukocytosis (white blood cell count often above 15,000–20,000/mm³), and indicators of dehydration may all coexist.
The most severe cases may progress to toxic megacolon, a situation in which the colon is highly dilated and ceases its functions. This is a surgical emergency. Other severe complications are colonic perforation, septic shock, and kidney failure. Approximately 3 to 8 per cent of cases of pseudomembranous colitis develop to this fatal and life-threatening stage.
Any incidence of diarrhea during or following the administration of antibiotics, particularly in an elderly person or a patient admitted to hospital, should under no circumstances be presumed to be an incidental effect. Health assessment is significant.
How Is Pseudomembranous Colitis Diagnosed?
Pseudomembranous colitis is established by a combination of tests conducted by doctors. A single test will never narrate the entire story, and that is the reason why a layered approach is employed.[8]
- Stool Testing is usually the first step. The physician will test the stool to find the C. diff toxins or antigens.
- The most sensitive method is nucleic acid amplification testing (NAAT), usually PCR, which detects C. diff DNA in stool samples.
- There are also Enzyme immunoassays (EIA) that detect Toxin A and Toxin B and Glutamate dehydrogenase (GDH) antigen testing
- Blood tests may reveal leukocytosis, indicating significant infection. In serious instances of the disease, the number of white blood cells may become extremely high, even up to 100,000 per cubic millimeter.
- Colonoscopy or Flexible Sigmoidoscopy is a procedure that uses a flexible tube containing a camera and is inserted into the colon. This helps the doctor to get a direct view of the typical yellowish pseudomembranes on the colon wall. This procedure may also include taking biopsy samples to search for less common causes of the condition in case C. diff tests show a negative result.
- A CT scan or an abdominal X-ray could be ordered to check whether they have any complications, including toxic megacolon or bowel perforation.
Pseudomembranous Colitis: Treatment with Antibiotics
The irony is in fact true: it is antibiotics that lead to the development of pseudomembranous colitis, and it is antibiotics also that are mostly used to treat the latter. The difference here is that the treatment antibiotics are specifically aimed at C. diff and not at the broad-spectrum agents that initiated the problem in the first place.
Commonly Used Antibiotics
The most recent standard treatments, as also suggested by the Infectious Diseases Society of America (IDSA) and the Society for Healthcare Epidemiology of America (SHEA) in their updated guidelines of 2021, are:[9]
- Fidaxomicin has become the drug of choice as the first-line agent in pseudomembranous colitis due to C. diff. It acts through the prevention of bacterial RNA polymerase. Since it remains mostly in the gut, it avoids causing disturbance to the rest of the gut bacteria in the body. It is also been shown to have a lower recurrence rate than vancomycin.
- Vancomycin (oral) is still recognized as a viable and acceptable choice. It is given orally so that it reaches the colon directly. The oral form of vancomycin is not well absorbed in the bloodstream; this implies that the medication concentrates in areas where it is most required. The typical course is 10 to 14 days.
- Metronidazole used to be regarded as standard treatment, but nowadays it is used only in mild cases or in the absence of the other two drugs. It is less expensive and can be taken by mouth or given intravenously.
- Bezlotoxumab is a monoclonal antibody (not an antibiotic on its own) that assists in the neutralization of C. diff Toxin B. It is used alongside antibiotic treatment in patients who are at high risk of the recurrent infection.
Fecal microbiota transplantation (FMT)
Fecal microbiota transplantation (FMT) has become an alternative treatment option in patients who are non-responsive to antibiotics or where other medications have previously failed. This procedure involves transferring processed stool from a healthy donor into the patient’s colon to restore the natural balance of gut bacteria. It has demonstrated an overall success rate of over 80% in certain studies in the case of recurrent C. diff infection.[10]
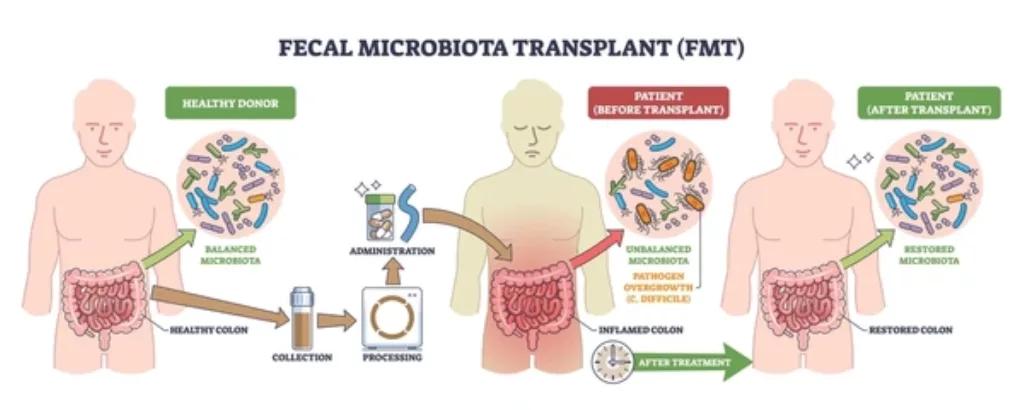
Fecal microbiota transplantation used to restore gut microbiota in pseudomembranous colitis.
Surgery can be required in extreme cases, such as the toxic megacolon or perforation of the colon. In such extreme cases, a colectomy (partial or complete resection of the colon) may be life-saving.
General Supportive Measures
Beyond antibiotics, supportive care plays an important role:[11]
- Stopping or switching the antibiotic that triggered the condition, if possible
- It is advisable to drink a lot of water and other fluids to stay well-hydrated with fluids and electrolytes.
- It is preferable to avoid using antidiarrheal medications such as loperamide, which may worsen the disease by retaining toxins
- Close observation in a hospital environment of severe or elderly patients.
Can Pseudomembranous Colitis Recur?
Unfortunately, yes. One of the most difficult things to deal with in this condition is recurrence. Pseudomembranous colitis can recur in a substantial proportion of patients even after effective treatment, occasionally only a few weeks after the antibiotic course.About 20–25% of patients experience recurrence after the first infection, and the risk increases with each subsequent episode.[12]
Recurrence occurs because:
- C. diff spores are difficult to completely eliminate
- the gut microbiome remains disrupted
The preventive strategies to avoid recurrence are to adhere to the entire course of treatment, maintain strong hand hygiene (use of soap and water) rather than alcohol-based sanitizers, and educate the next healthcare provider about a prior C. diff infection prior to initiating new antibiotics.
Prevention: What the Hospitals and Individuals Can Do?
The solution to the spread of C. diff is at both the individual and institutional levels.[13]
In hospitals and other healthcare facilities, it is essential to prevent the infection from spreading. This means keeping infected people away from others, wearing masks and gloves, and cleaning everything thoroughly with strong disinfectants that have bleach in them. C. diff spores are resistant to alcohol gel hand sanitizers. Must use soap and water.
The best practical prevention measures to take by individuals are:
- Thorough washing of hands with soap and warm water, particularly after bathing and before eating.
- Using antibiotics when they are really required and in the exact dosage.
- When starting any new medications, it is important to inform the doctors of any previous history of C. diff infection.
Final Thoughts
Pseudomembranous colitis is a serious condition that most commonly occurs as a complication of Clostridioides difficile infection following antibiotic use. While the illness may begin with mild diarrhea, it can progress to severe inflammation and life-threatening complications if left untreated.
Specific antibiotic treatment of pseudomembranous colitis, together with more recent interventions such as fecal transplants and monoclonal antibodies, has yielded better results.
Anyone who develops persistent watery diarrhea during or after antibiotic therapy, especially if accompanied by fever or abdominal pain, should seek medical evaluation promptly.
References
[1] Price AB, Davies DR. Pseudomembranous colitis. J Clin Pathol. 1977;30(1):1–12. doi:10.1136/jcp.30.1.1
[2] Bartlett JG, Chang TW, Gurwith M, Gorbach SL, Onderdonk AB. Antibiotic-associated pseudomembranous colitis due to toxin-producing clostridia.N Engl J Med.
[3] Lessa FC, et al.Burden of Clostridium difficile Infection in the United States.N Engl J Med. 2015.
[4] Surawicz CM, McFarland LV. Pseudomembranous colitis: causes and cures.Digestion. 1999;60(2):91–100. doi:10.1159/000007633
[5] Pépin J, Saheb N, Coulombe MA, et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile–associated diarrhea: a cohort study during an epidemic in Quebec.Clin Infect Dis. 2005;41(9):1254–1260. doi:10.1086/496986
[6] Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile–associated diarrhea with high morbidity and mortality.N Engl J Med. 2005;353(23):2442–2449. doi:10.1056/NEJMoa051639
[7] Fekety R. Guidelines for the diagnosis and management of Clostridium difficile–associated diarrhea and colitis.Am J Gastroenterol. 1997;92(5):739–750. PMID: 9149180
[8] Burnham CA, Carroll KC. Diagnosis of Clostridium difficile infection: an ongoing conundrum for clinicians and for clinical laboratories.Clin Microbiol Rev. 2013;26(3):604–630. doi:10.1128/CMR.00016-13
[9] Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults.Clin Infect Dis. 2021;73(5):e1029–e1044. doi:10.1093/cid/ciab549
[10] van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent Clostridium difficile.N Engl J Med. 2013;368(5):407–415. doi:10.1056/NEJMoa1205037
[11] Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).Infect Control Hosp Epidemiol. 2010;31(5):431–455. doi:10.1086/651706
[12] McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW, Greenberg RN. Recurrent Clostridium difficile disease: epidemiology and clinical characteristics.Infect Control Hosp Epidemiol. 1999;20(1):43–50. doi:10.1086/501553
[13] Gerding DN, Muto CA, Owens RC Jr. Measures to control and prevent Clostridium difficile infection.Clin Infect Dis. 2008;46(Suppl 1):S43–S49. doi:10.1086/521861