
{kind=link}

What is Rotor Syndrome?: Rotor Syndrome Comprehensive
Rotor Syndrome Comprehensive Rotor syndrome or Rotor type hyperbilirubinemia is a rare congenital disease that impairs the capacity of the liver to process and store bilirubin. Bilirubin is a yellowish material formed as a result of the normal breakdown of red blood cells at the end of their lifespan. This bilirubin is usually processed by the liver which disposes of it through the body in the bile.
In patients with Rotor syndrome, the liver has impaired uptake and storage of conjugated bilirubin, causing conjugated bilirubin to leak back into the bloodstream. As a result, patients develop predominantly conjugated hyperbilirubinemia, although both conjugated and unconjugated fractions may be elevated. As a result of this hyperbilirubinemia, jaundice or a yellowness of the skin and whites of the eyes occurs.jaundice with direct van den Bergh reaction.Acta Medica Philippina. 1948;5:37-49.” style=”position:relative;color:#309b65;cursor:help;border-bottom:1px dotted #309b65;font-weight:bold”>[1]
The positive aspect is that Rotor Syndrome is entirely benign. It has no liver damage, it does not progress to more severe liver disease, and it does not need treatment.
Prevelance
The disease was initially described in 1948 by Filipino doctor Arturo Belleza Rotor and his colleagues, and is very rare, with only a few hundred documented cases worldwide. Although it brings about visible jaundice, people with Rotor syndrome can have normal health and normal life expectancy without the need for medical intervention.[2]
Rotor Syndrome vs Dubin-Johnson Syndrome
Rotor syndrome is frequently associated with Dubin-Johnson syndrome since the two disorders produce similar effects of jaundice as a result of high conjugated bilirubin levels. Yet, these two disorders are different in their underlying cause. The most remarkable difference is that Rotor syndrome presents a liver with a totally normal biopsy, whereas Dubin-Johnson syndrome exhibits characteristic black pigmentation in the liver cells.[3]
Comparison: Dubin-Johnson vs Rotor Syndrome
| Feature | Rotor Syndrome | Dubin-Johnson Syndrome |
|---|---|---|
| Liver Pigmentation | Absent (normal liver) | Present (black pigmentation) |
| Gene Mutation | SLCO1B1 + SLCO1B3 | ABCC2 |
| Affected Protein | OATP1B1 and OATP1B3 | MRP2 |
| Bilirubin Type | Mixed (conjugated + unconjugated) | Predominantly conjugated |
| Bilirubin Level | 2-5 mg/dL (can reach 20 mg/dL) | 2-5 mg/dL (can reach 25 mg/dL) |
| Urinary Coproporphyrin | Elevated (2-5x normal) | Normal or slightly elevated |
| Coproporphyrin I % | ~65% | ~80-90% |
| Oral Cholecystography | Gallbladder visible | Gallbladder not visible |
| Liver Histology | Completely normal | Dark pigment deposits |
| Primary Defect | Hepatic storage and uptake are impaired | Impaired biliary excretion |
| Prognosis | Excellent, benign | Excellent, benign |
Rotor Syndrome Causes
Rotor syndrome is a genetic disease that is transmitted in an autosomal recessive manner. This implies that the individual must inherit both defective copies of both SLCO1B1 and SLCO1B3 genes – one copy of each is inherited by either parent. These are genes that are clustered near chromosome 12.[4]
Rotor Syndrome Mutation
SLCO1B1 and SLCO1B3 encode OATP1B1 and OATP1B3, which are transport proteins responsible for moving bilirubin and other organic compounds into liver cells. The mutation of both genes expresses the syndrome. The functions of the two proteins overlap in that one can partially compensate for the failure of the other.[5]
When mutations occur in both genes, the resulting proteins are either:
- Excessively short and dysfunctional
- Completely absent
The liver is unable to readily absorb the bilirubin in the bloodstream or store it in a normal manner in the liver cells without functional proteins. This results in the buildup of bilirubin in the blood and results in the typical jaundice of Rotor syndrome.
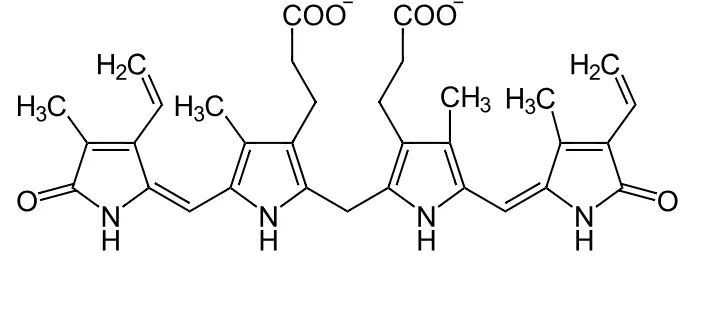
Structure of bilirubin, Rotor type hyperbilirubinemia. By NEUROtiker – Own work,Public Domain
Inheritance Pattern:
- In case both parents are carriers: Each child has an equal 25% chance of having Rotor syndrome, an equal 50% chance of being a carrier, and an equal 25% chance of inheriting two normal genes.
- Carriers (individuals who have a normal gene and a mutated gene) do not have symptoms but have the potential of transmitting the condition to their offspring.
- Consanguinity: A high number of people with Rotor syndrome are born in consanguineous (related) couples, which also increases the chances of inheriting identical recessive genes from both parents.
Rotor Syndrome Symptoms
Jaundice is the hallmark of the Rotor syndrome, but the good news is that it is usually the sole symptom that patients develop. Rotor syndrome does not result in pain, fatigue, and progressive liver damage, which are the characteristics of many other liver diseases.[6]
Primary Symptoms:
Jaundice:

Yellow discoloration of the sclera (icterus) due to jaundice in Rotor Syndrome
- Yellowing of the sclera and skin (scleral icterus).
- Typically occurs soon after birth or during childhood.
- May fluctuate with illness, fasting, or stress.
- It becomes more evident in natural sunlight.
In most cases, the patients of Rotor syndrome do not show any symptoms except the observable jaundice.
Rare Additional Symptoms:
Although rare, the patient can experience:
- Light cases of abdominal discomfort or epigastric pain.
- Occasional low-grade fever
- As jaundice becomes severe, mild fatigue will develop.
Factors That Can Aggravate the Jaundice:
The following conditions may temporarily increase the bilirubin levels and the jaundice:
- Intercurrent illness or infections
- Pregnancy
- Use of oral contraceptives
- Stress in the form of physical or emotional stress
- Fasting or dietary changes
- Certain medications
It is important to mention that even in the case of worsening jaundice, Rotor syndrome is not harmful and does not necessarily signify the presence of liver damage or disease progression.
Age of Onset:
You can observe the syndrome in two periods:
- Neonates are noticed to have slight jaundice soon after birth.
- Children or adults are diagnosed more frequently when the jaundice becomes evident or is identified with the help of regular blood tests.
Rotor Syndrome Diagnosis
Rotor syndrome diagnosis should be carried out systematically to eliminate other causes of jaundice and hyperbilirubinemia. Because it is a diagnosis of exclusion, you need to carry out several tests.
The first assessment is a detailed medical history, such as the onset of jaundice, age, family history of jaundice or liver disease, consanguinity in parents, related symptoms, history of medication, and what aggravates jaundice.[7]
Physical Findings
Physical examination determines the extent of jaundice and examines whether there is hepatomegaly or splenomegaly, which is not expected in Rotor syndrome.
Laboratory Tests
Diagnosis is based on laboratory tests.
Elevated Bilirubin:
- Total serum bilirubin: It is usually 2-5 mg/dL, although it may be up to 20 mg/dl.
- More than half of the serum bilirubin is Conjugated (direct) bilirubin.
- The second type, unconjugated (indirect), is less than the above
The peculiarity is that liver enzymes (ALT, AST, ALP, GGT) are totally normal, along with the level of albumin, and a coagulation test. Complete blood count is best to exclude hemolytic anemia, and reticulocyte and hemoglobin counts are normal.
Urine Complete
The most valuable diagnostic is the urinary coproporphyrin test that demonstrates total coproporphyrin increasing 2-5 times over normal, with coproporphyrin I taking up around 65% of total (in comparison with normal 25%) of total coproporphyrin. This is essential in distinguishing between Rotor and Dubin-Johnson syndrome.[8]
Imaging
Imaging studies play a supportive role in diagnosis.
- The ultrasound of the abdomen demonstrates the normal size and appearance of the liver, excluding the obstruction of the biliary and structural abnormalities.
- Oral cholecystography shows the gallbladder, and it is used to differentiate between Rotor and Dubin-Johnson syndrome, where the gallbladder is not usually visible.[9]
- Hepatobiliary scintigraphy (HIDA scan) – there is sluggish hepatic uptake of radiotracer with prominent kidney excretion and delayed/no gallbladder visualization.
- Although not routinely required, in case a liver biopsy is conducted, it reveals entirely normal liver histology without pigment deposition, as is the case in Dubin-Johnson syndrome.
- Confirm the diagnosis with the help of molecular genetic testing that reveals mutations in both SLCO1B1 and SLCO1B3 genes; it is especially effective when other tests are ambiguous.
Differential Diagnosis:
Rotor syndrome must be distinguished from:[10]
- Dubin-Johnson syndrome: Just like Rotor, though liver pigmentation is also present.
- Gilbert syndrome: Unconjugated Hyperbilirubinemia.
- Viral hepatitis
- Cholestasis induced by drugs: History of drug use, high enzymes.
- Autoimmune hepatitis
- Biliary obstruction; ultrasound has enlarged bile ducts.
- Hemolytic anemia
- Wilson’s disease presents itself with low levels of ceruloplasmin and high levels of copper.
- Crigler-Najjar syndrome is characterized by serious unconjugated hyperbilirubinemia.
Rotor Syndrome Treatment
The most reassuring factor about Rotor syndrome is that it does not need any special treatment. This is a completely harmless condition that never develops into liver damage or hepatopathy. Rotor syndrome does not inflict any damage to the liver or general well-being, so no medications or interventions are needed. The jaundice itself, although visible, is not harmful and does not require treatment.[11]
Educate Patient
The most important aspect of management is educating patients and families that Rotor syndrome is a benign and lifelong condition where jaundice will persist, but is harmless. The life expectancy is entirely normal, no dietary limitations are required, and the condition will never lead to liver disease.

A doctor explaining liver disease to an elderly patient with Rotor Syndrome.
As a rule, no follow-up is necessary, except in cases of:
- New symptoms are observed, which indicate an unrelated disease,
- Other liver disease is suspected, and
- In pregnancy
Medical Management
Since OATP1B1 and OATP1B3 proteins have a role in drug metabolism, patients are to inform all healthcare providers of their diagnosis and be careful with taking some medications that depend on these transporters. A specific issue is the case of irinotecan, a chemotherapy drug, which can lead to more toxicity in patients with Rotor syndrome.[12]
Protect Your Liver
Although the Rotor syndrome on its own is not dangerous, liver protection is still needed. Patients should:
- Stay vaccinated for hepatitis A and B.
- Avoid excessive alcohol
- Avoid hepatotoxic medications
- There are no particular dietary limitations, and regular physical activity and a healthy lifestyle are promoted.
Special Considerations
Some considerations are applicable in special situations.
Fertility
Rotor syndrome does not affect fertility, and pregnancy can be safely carried out by women with the disorder, but jaundice can be aggravated in pregnancy, although it is not malignant. During pregnancy, close monitoring is advised because the diagnosis of the pregnancy-related liver condition may be complicated.
Surgery
No special precaution in surgery or anesthesia is observed, but the diagnosis should be reported to the anesthesiologist.
Genetic counseling
It is advised that genetic counseling should be performed for affected individuals who are planning to have children because it is common to find that parents are asymptomatic carriers, and every child has a probability of 25% of inheriting the condition. Prenatal testing can be done, though it is not generally recommended as the disorder is benign in nature.
Prognosis and Life Expectancy
The prognosis for Rotor syndrome is excellent, and it has no impact on life expectancy. The disorder is non-progressive and benign. It does not cause cirrhosis, liver failure, or cancer, nor does it progress as time goes by.[13]
People are in a normal quality of life, and there are no limitations regarding activities, work, and physical activities. There is no effect on the growth and development of children.
When to Seek Medical Attention:
Rotor Syndrome does not need any treatment, although a patient should visit the doctor in case they have:
- Emerging symptoms on top of jaundice (pain in the abdomen, change in color of urine, light stools)
- Severely worsened idiopathic jaundice.
- Acute hepatitis (symptoms are fever, severe fatigue, and nausea).
- Any dysfunction of the liver
These symptoms indicate another disease that should be evaluated.
Conclusion
Rotor syndrome is a very rare but entirely harmless inherited condition that leads to jaundice throughout life since it leads to a failure of the liver to store bilirubin. Although it is an aggressive form of cancer and can go undetected for months, if caught early in the limited stage, the prognosis is better. The cases of Rotor syndrome are uncommon, and most of the patients spend their lifetime living with the disease, leading to a normal life expectancy and a good life. In case you are suspicious that you or a loved one has Rotor syndrome, you need to talk to a gastroenterologist or hepatologist and be diagnosed accordingly and reassured.
References
[1] Rotor AB, Manahan L, Florentin A. Familial non-hemolytic jaundice with direct van den Bergh reaction.Acta Medica Philippina. 1948;5:37-49.
[2] Stapleton FB, Koontz WC, Hilligoss DM. Rotor syndrome: Review of the literature and report of a family.Clin Pediatr (Phila). 1976;15(9):839-842.
[3] Togawa T, Mizuochi T, Sugiura T, et al. Clinical, pathologic, and genetic features of neonatal Dubin-Johnson syndrome: a multicenter study in Japan.J Pediatr. 2018;196:161-167.e1.
[4] Cheng YY, Chang KC, Chen PL, et al. SLCO1B1 and SLCO1B3 genetic mutations in Taiwanese patients with Rotor syndrome.J Formos Med Assoc. 2023;122(7):648-652. doi:10.1016/j.jfma.2023.03.003
[5] Kagawa T, Oka A, Kobayashi Y, et al. Recessive inheritance of population-specific intronic LINE-1 insertion causes a Rotor syndrome phenotype.Hum Mutat. 2015;36(3):327-332. doi:10.1002/humu.22739
[6] Sticova E, Jirsa M. New insights in bilirubin metabolism and their clinical implications.World J Gastroenterol. 2013;19(38):6398-6407. doi:10.3748/wjg.v19.i38.6398
[7] Shimizu Y, Naruto H, Ida S, Kohakura M. Urinary coproporphyrin isomers in Rotor’s syndrome: a study in eight families.Hepatology. 1981;1(2):173-178. doi:10.1002/hep.1840010214
[8] Shimizu Y, Naruto H, Ida S, Kohakura M. Urinary coproporphyrin isomers in Rotor’s syndrome: a study in eight families.Hepatology. 1981;1(2):173-178. doi:10.1002/hep.1840010214
[9] Bar-Meir S, Baron J, Seligson U, et al. 99mTc-HIDA cholescintigraphy in Dubin-Johnson and Rotor syndromes.Radiology. 1982;142(3):743-746.
[10] Strassburg CP. Hyperbilirubinemia syndromes (Gilbert-Meulengracht, Crigler-Najjar, Dubin-Johnson, and Rotor syndrome).Best Pract Res Clin Gastroenterol. 2010;24(5):555-571. doi:10.1016/j.bpg.2010.07.007
[11] Keppler D. The roles of MRP2, MRP3, OATP1B1, and OATP1B3 in conjugated hyperbilirubinemia.Drug Metab Dispos. 2014;42(4):561-565. doi:10.1124/dmd.113.055772
[12] Teft WA, Welch S, Lenehan J, et al. OATP1B1 and tumour OATP1B3 modulate exposure, toxicity, and survival after irinotecan-based chemotherapy.Br J Cancer. 2015;112(5):857-865. doi:10.1038/bjc.2015.5
[13] Saxena R, Theise N, Crawford JM. Microanatomy of the human liver: exploring the hidden interfaces.Hepatology. 1999;30(6):1339-1346.