
{kind=link}

Signs Seizure Look A seizure in itself is not a disease; it is a symptom of abnormal, excessive electrical activity in the brain, and can happen anywhere, at any time, which is why they are so disruptive to daily life.
When most people think of a seizure, they picture someone shaking violently and losing consciousness, but that is a misconception because of which, epilepsy is considered synonymous with a seizure. But a seizure can look like something as simple as someone suddenly staring off into space, a sudden jerk of the arm, or a brief moment of confusion. This gap between public knowledge and clinical reality isn’t unique, but in the case of seizures, it can be disastrous.
What is a Seizure?: Signs Seizure Look
The brain functions through electrical signals, which are essentially neurons communicating constantly in organised, controlled patterns. A seizure occurs when there is a sudden, uncontrolled burst of electrical activity in one or more areas of the brain. This abnormal electrical surge disrupts whatever that brain region normally controls: movement, sensation, emotion, consciousness, or memory.[1]
Unlike popular knowledge, most seizures don’t last for minutes; most are between 30 seconds and 2 minutes. And any seizure lasting more than 5 minutes is a medical emergency (status epilepticus). A single seizure does not equal a disease like epilepsy; epilepsy is defined as two or more unprovoked seizures.
The difference between provoked and unprovoked seizures is that provoked seizures have an identifiable trigger (such as fever, low blood sugar, alcohol withdrawal, or drug toxicity), while unprovoked seizures do not.
What are the Different Types of Seizures?
The latest standard to classify seizures is the International League Against Epilepsy (ILAE) 2017 classification, according to which seizures are broadly divided into two major categories: focal (partial) onset and generalised onset.[2]
Focal onset seizures:
Focal seizures begin in one area of the brain, and are less dramatic than generalised ones. Some subtypes are:
- Focal aware seizures, previously called simple partial seizures
- Focal impaired awareness seizures, called complex partial seizures in the old classification
- Focal to bilateral tonic-clonic seizures are focal seizures that start in one region but then spread to both hemispheres.
Generalized Onset Seizures:
In generalized onset seizures, both hemispheres are involved from the start. They can be:
- Tonic-clonic (grand mal) seizures are the classic, most recognised type
- Absence (petit mal) seizures are brief, sudden lapses in awareness
- Tonic, atonic, and clonic seizures involve changes in the muscle tone
- Myoclonic seizures are brief, shock-like muscle jerks
When the onset of a seizure cannot be determined, it can be classed into a third category: seizures of unknown onset. Being able to correctly classify a seizure is essential for clinicians because different types respond to different medications, and the wrong treatment may be disastrous.
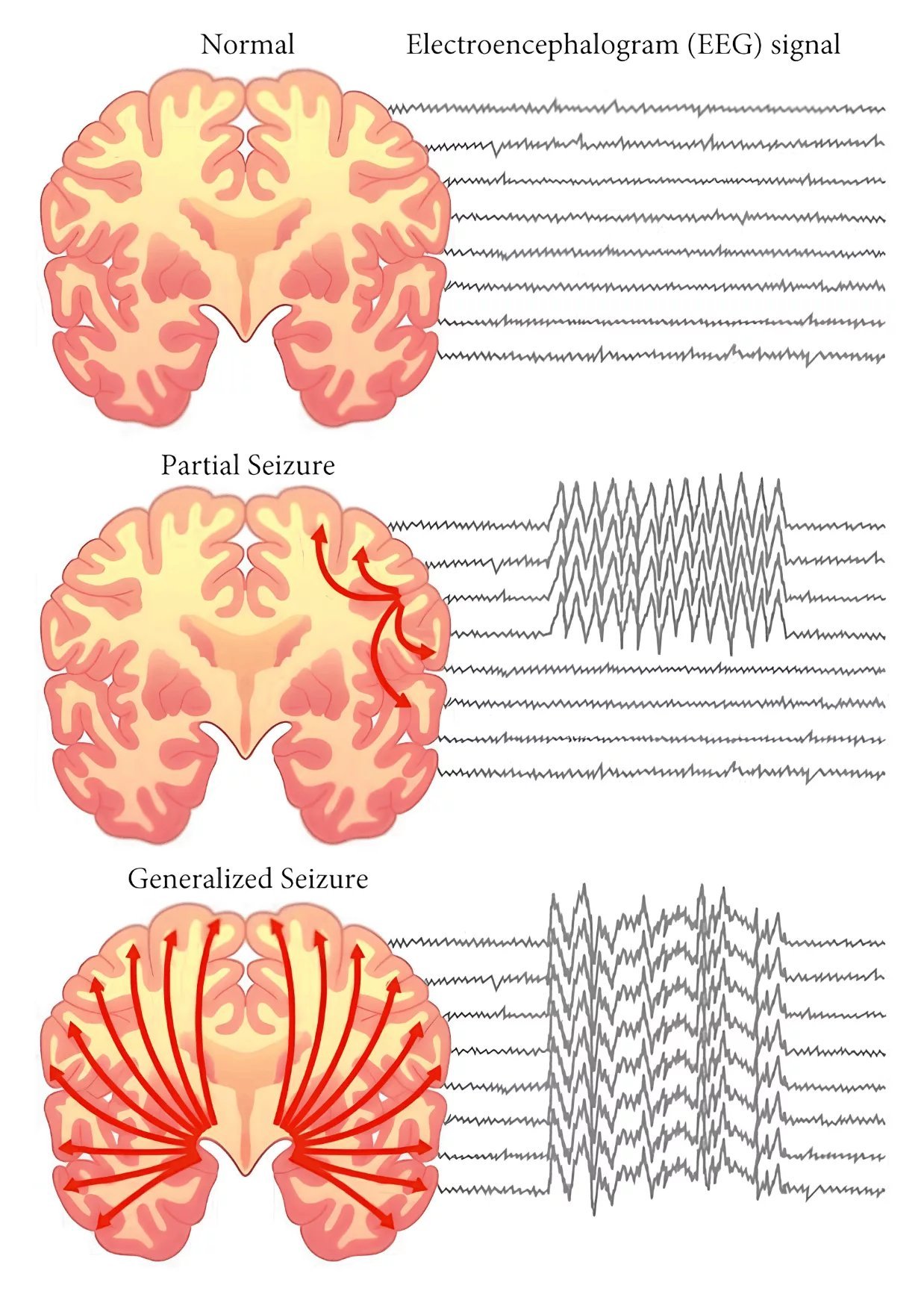
EEG signals in the normal brain compared with a focal seizure and a generalized seizure (Image Courtesy: Sadiq, Muhammad Tariq, Akbari, Hesam, Rehman, Ateeq Ur, Nishtar, Zuhaib, Masood, Bilal, Ghazvini, Mahdieh, Too, Jingwei, Hamedi, Nastaran, Kaabar, Mohammed K. A., Exploiting Feature Selection and Neural Network Techniques for Identification of Focal and Nonfocal EEG Signals in TQWT Domain, Journal of Healthcare Engineering, 2021, 6283900, 24 pages, 2021. Available fromWileyand licensed under CC by 4.0)
What Does a Seizure Look Like?
A seizure can look different based on its type. Each type can have distinct symptoms. For example:
Tonic-clonic seizure:
Tonic-clonic seizures often start with a sudden cry or vocalisation at onset, caused by air forced through the vocal cords by muscle contraction. The first phase is the tonic phase, where the person falls, and the body goes rigid; most injuries occur during this. This is followed by the clonic phase, which involves a rhythmic jerking of the limbs.
A common occurrence is the person biting their tongue or inner cheek. Another important clinical sign, which is often embarrassing for the patient, is urinary or fecal incontinence.
Once the seizure ends, the postictal phase begins, where the person is confused, disoriented, and often so exhausted that they just want to sleep. This phase might last for minutes to hours, and is a key clinical distinguishing feature from syncope (fainting), where recovery is rapid.[3]
Common symptoms of an epileptic seizure (Image Courtesy: Zarqa Altaf, Mukhtiar Ali Unar, Sanam Narejo, Muhammad Ahmed Zaki and Naseer-u-Din. “Generalized Epileptic Seizure Prediction using Machine Learning Method”. International Journal of Advanced Computer Science and Applications (IJACSA) 14.1 (2023). Available fromResearchGateand licensed under CC by 4.0)
Absence Seizure:
These involve the person suddenly going into a blank stare, mid-sentence or mid-activity. There is no falling or convulsing; the person just stops what they were doing, and their eyes may flutter or roll slightly upwards. Then the person immediately resumes activity, and oftentimes, they themselves aren’t aware that anything happened. Absence seizures are frequently missed or mistaken for daydreaming or ADHD, especially in children, but they also occur in adults.
Focal Aware Seizure:
These are actually what are sometimes called auras, but clinically, an aura is a focal aware seizure, not merely a warning. The seizure involves experiencing abnormal sensations (tingling, numbness), unusual smells or tastes (often described as burning rubber or metallic), déjà vu, or a sudden unexplained fear or emotion. The person remains fully conscious, though, and can describe the experience.
Focal Impaired Awareness Seizure:
These are focal but slightly different in that the person appears awake but is unresponsive or only partially unresponsive. The characteristic feature is automatism, i.e., repetitive, semi-purposeful movements the person is completely unaware of, maybe lip smacking, chewing, picking at clothing, hand rubbing, or repeating words or phrases. Postictal confusion follows after the seizure, which separates it from an absence seizure.
Myoclonic seizures are brief, sudden muscle jerks often of the arms or shoulder, and we see these classically in the morning after waking up, causing the person to drop things. Atonic seizures, on the other hand, are a sudden, complete loss of muscle tone where the person just falls to the ground without any warning; these have a high risk of facial or head injury. Similar falls can be caused by tonic seizures.
Warning Signs of a Seizure
Not every seizure has a warning, especially generalised onset seizures, which typically begin without any preceding signal. In cases where a warning does exist, it is called an aura, but the aura itself is a focal aware seizure. However small, an aura gives the person a few precious seconds to get to safety, sit down, or at least move away from hazards.
Some commonly observed aura types are:
- Sensory: tingling, numbness, visual signs like flashing lights, unusual and often unpleasant smells or tastes
- Autonomic: patients describe it vividly, like a wave of feeling rising from the stomach toward the chest
- Psychic: a dreamy or detached feeling, déjà vu or jamais vu, sudden unexplained fear or panic
- Motor: twitching of a limb, the head turning to one side (a versive seizure)
Some people notice a pre-ictal pattern hours before a seizure: can be mood changes, irritability, anxiety, or a headache. Not the same as aura, but it is still a pattern worth tracking. Patients are encouraged to keep a seizure diary to identify personal patterns.
Absence Seizures in Adults
Absence seizures are strongly associated with children, but the fact is that they can both persist into adulthood or first appear in adults. Rather than in isolation, in adults, absence seizures are more likely to occur along with other seizure types. And the presentation tends to be atypical with a longer duration and postictal confusion. This is why they are commonly misdiagnosed as dissociative episodes, TIAs, or a migraine with aura.[4]
Since the blank stare tell isn’t always seen in adults, the diagnostic hallmark is the EEG finding: 3 Hz generalised spike-and-wave discharges. To record an EEG, clinicians sometimes use deliberate hyperventilation to provoke the seizure.
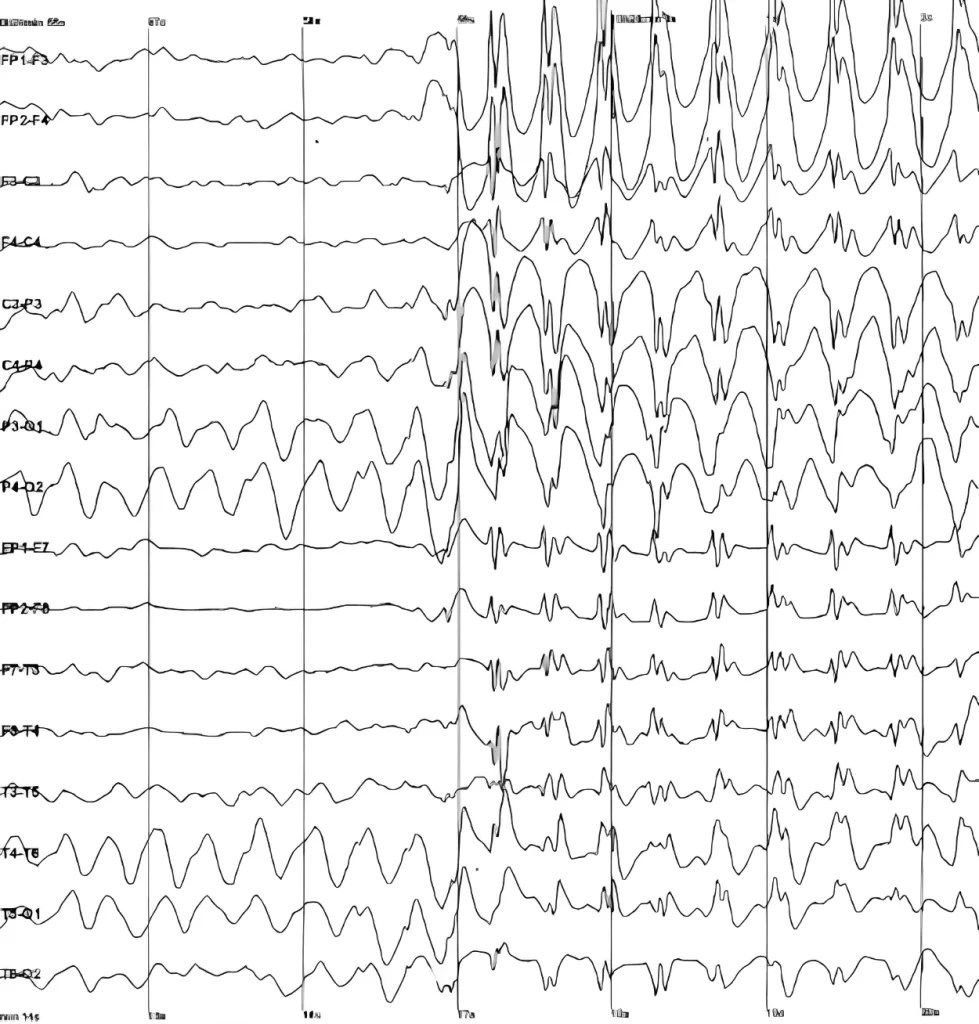
An EEG tracing showing generalised spike-and-wave discharges, the hallmark finding in absence seizures. The sudden shift from normal background activity to high-amplitude spike-and-wave patterns is clearly visible. (Image Courtesy: Der Lange viaWikimedia Commonsand licensed under CC by SA 2.0)
What Can Cause a Seizure?
Seizures are the consequence of a whole range of conditions, from electrolyte imbalance to infections to drugs that can alter the electrical signals in the brain; some of these are:
- Epilepsy: the most common cause
- Structural anomalies like a stroke, brain tumor, traumatic brain injury, hippocampal sclerosis, cortical dysplasia[5]
- Metabolic causes can cause provoked seizures, e.g., hypoglycemia, hyponatremia, hypocalcemia, or hepatic encephalopathy. Fortunately, a lot of these are reversible.
- Infections like meningitis, encephalitis, and brain abscesses are leading causes of epilepsy in many parts of the world
- Alcohol is a major cause, both in intoxication and withdrawal
- Use of drugs like cocaine, amphetamines, tramadol, and tricyclic antidepressants; abrupt withdrawal from benzodiazepines or anti-seizure medications causes seizures as well.[6]
- Autoimmune diseases like anti-NMDA receptor encephalitis are increasingly recognised, especially in young women presenting with psychiatric symptoms alongside seizures[7]
- Seizures in pregnancy, eclampsia, are an emergency
- Fever, e.g., febrile seizures in children
Triggers of Seizures
Triggers are conditions or substances that lower the threshold in someone who is already exposed to a cause of a seizure.
- Sleep deprivation is one of the most potent and consistent triggers
- If someone misses their anti-seizure medication, breakthrough seizures are very common
- Alcohol and recreational drugs can trigger seizures
- Stress and emotional disturbance
- Systemic infections lower the seizure threshold
- Hormonal changes; catamenial epilepsy is when seizures occur around menstruation due to fluctuating oestrogen and progesterone levels[8]
- Photosensitivity is a very common trigger in generalised seizures. Around 3% of people with epilepsy get triggered by flashing lights like TV screens, video games, and even sunlight flickering through trees
- Reflex epilepsies are seizures triggered specifically by eating, reading, or music
Diagnosis of Seizures
A proper diagnosis of a seizure type is best done by observing an episode; a detailed eyewitness account is often more useful than any test. This is why witnesses are encouraged to record the episode on video if safe to do so. If needed, there are several diagnostic tests that can be done:

A cap fitted with electrodes records the brain’s electrical activity during an EEG — the most important diagnostic test for seizures. (Image Courtesy: Chris Hope viaWikimedia Commons,licensed under CC BY 2.0)
- EEG is the most important test as it directly records the brain’s electrical activity. The catch is that seizures don’t happen on demand, so a normal EEG cannot rule out epilepsy. Prolonged video-EEG monitoring is the gold standard.[9]
- MRI can identify structural causes like tumors or vascular malformations
- Blood tests can pinpoint metabolic and electrolyte-related causes
- Serum prolactin rises after a generalised tonic-clonic seizure, and peaks at 10-20 minutes
- PNES (psychogenic non-epileptic seizures): also called functional seizures, these are episodes that look exactly like epileptic seizures, but there is no abnormal electrical activity. It gets misdiagnosed as epilepsy very often. Serum prolactin can help diagnose it, but video-EEG is the only definitive diagnostic tool.[10]
Seizure Safety
A seizure cannot be stopped mid-episode, but knowing what to do during one can make a real difference to the outcome.
During a tonic-clonic seizure, it is important to stay calm and note the duration of the seizure. Since the head is at risk of injury during the episode, it should be cushioned with something soft, and the surrounding area should be cleared. A common cause of death or complication in seizures is airway obstruction. After the convulsions stop, the patient should be rolled into the recovery position to protect the airway.
It’s also important to know that several safety myths instead cause harm, e.g., restraining the patient, or putting something in the mouth to keep the tongue from being ‘swallowed’.[11] Giving the patient food or water before they become fully conscious is also not encouraged because of the risk of airway obstruction.
A witness must immediately call emergency services if:
- They know it’s the patient’s first episode, or if another seizure follows without recovery
- The seizure lasts for more than 5 minutes (may be status epilepticus)[12]
- The person doesn’t regain consciousness
- There has been an injury during the seizure
- The person is pregnant or has diabetes (the seizure may have been caused by severe hypoglycemia)
Fatality in Epilepsy
Sudden unexpected death in epilepsy (SUDEP) is a real risk, but only about 1 in 1000 adults with epilepsy die per year.[13] In fact, fatality is strongly associated with an unwitnessed tonic-clonic seizure during the night or poor adherence to medication. Good seizure control significantly reduces the risk, and some people may be considered for medication withdrawal after a prolonged seizure-free period, guided by a specialist.
The person affected by seizures has to follow several safety tips in their daily life as well. For example, showers over baths, never swim alone, caution around heights and machinery, keeping a card along that can guide witnesses to call an emergency contact in case of an episode.
Then there are legal obligations as well, most notably, traffic authorities need to be informed about the seizures, and most countries require there to be a seizure-free period before driving can be allowed.
Final Takeaway
Around 70% of people with epilepsy are able to achieve good seizure control by adhering to the right medicine. Anti-seizure medications (ASMs) are prescribed on an individualised basis based on seizure type, age, sex, and other health conditions. Individualisation is especially important in women of childbearing age, because some ASMs carry significant teratogenic risk, e.g., sodium valproate.
Sometimes an initial ASM might fail and need to be replaced, but if two appropriate ASMs fail, it is recognised as drug-resistant epilepsy, and prompts a referral for other strategies: surgical evaluation, or neuromodulation therapies like vagus nerve stimulation.[14]
Seizures still remain a stigma in society, and this stigma, along with the constant anxiety about when the next episode may occur, takes a toll on a person. Yet, this aspect gets overlooked when dealing with seizure management. Along with medication, psychological care needs to be made part of the treatment from the start.
References
[1] Lovik K, Murr NI. Seizure. [Updated 2023 Feb 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430765/
[2] Anwar H, Khan QU, Nadeem N, Pervaiz I, Ali M, Cheema FF. Epileptic seizures. Discoveries (Craiova). 2020 Jun 12;8(2):e110.
[3] Fisher, R. S., & Engel, J. J., Jr (2010). Definition of the postictal state: when does it start and end?. Epilepsy & behavior : E&B, 19(2), 100–104. https://doi.org/10.1016/j.yebeh.2010.06.038
[4] Ozdemir HH, Demir CF, Cura HS. Absence status seen in an adult patient. J Neurosci Rural Pract. 2013 Jul;4(3):342-4. doi: 10.4103/0976-3147.118809.
[5] Garner, G. L., Streetman, D. R., Fricker, J. G., Bui, N. E., Yang, C., Patel, N. A., Brown, N. J., Shahrestani, S., Rangel, I. C., Singh, R., & Gendreau, J. L. (2022). Focal cortical dysplasia as a cause of epilepsy: The current evidence of associated genes and future therapeutic treatments. Interdisciplinary Neurosurgery, 30, 101635.
[6] Ostroumova TM, Ostroumova OD, Akimova ES, Kochetkov AI. [Drug-induced seizures: prevalence, risk factors, treatment and prevention]. Zhurnal Nevrologii i Psikhiatrii Imeni S.S. Korsakova. 2019 ;119(11):86-97. DOI: 10.17116/jnevro201911911186.
[7] Kayser MS, Dalmau J. Anti-NMDA Receptor Encephalitis in Psychiatry. Curr Psychiatry Rev. 2011;7(3):189-193. doi: 10.2174/157340011797183184.
[8] Verrotti A, D’Egidio C, Agostinelli S, Verrotti C, Pavone P. Diagnosis and management of catamenial seizures: a review. Int J Womens Health. 2012;4:535-41. doi: 10.2147/IJWH.S28872. Epub 2012 Sep 28.
[9] Maganti RK, Rutecki P. EEG and epilepsy monitoring. Continuum (Minneap Minn). 2013 Jun;19(3 Epilepsy):598-622. doi: 10.1212/01.CON.0000431378.51935.d8.
[10] Reuber, M. Psychogenic nonepileptic seizures: diagnosis, aetiology, treatment and prognosis. Swiss Arch. Neurol. Psychiatry Psychother. 2005, 156, 47-57. https://doi.org/10.4414/sanp.2005.01574
[11] Rossi, K. C., Baumgartner, A. J., Goldenholz, S. R., & Goldenholz, D. M. (2020). Recognizing and refuting the myth of tongue swallowing during a seizure. Seizure, 83, 32–37. https://doi.org/10.1016/j.seizure.2020.09.023
[12] Kaplan, P., & Johnson, E. (2020). Status Epilepticus: Definition, Classification, Pathophysiology, and Epidemiology. Seminars in Neurology, 40(6), 647–651. https://doi.org/10.1055/s-0040-1718722
[13] Harden C, Tomson T, Gloss D, Buchhalter J, Cross JH, Donner E, French JA, Gil-Nagel A, Hesdorffer DC, Smithson WH, Spitz MC, Walczak TS, Sander JW, Ryvlin P. Practice Guideline Summary: Sudden Unexpected Death in Epilepsy Incidence Rates and Risk Factors: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Epilepsy Curr. 2017 May-Jun;17(3):180-187. doi: 10.5698/1535-7511.17.3.180.
[14] Ryvlin P, Jehi LE. Neuromodulation for Refractory Epilepsy. Epilepsy Curr. 2021 Dec 15;22(1):11-17. doi: 10.1177/15357597211065587.