
 is a group of genetic disorders characterized by distinctive bone and...){kind=link}

Spondyloepiphyseal Dysplasia Collagen Spondyloepiphyseal dysplasia (SED) is a group of genetic disorders characterized by distinctive bone and cartilage abnormalities in the vertebrae as well as the epiphyses of the long bones. The bones fail to develop properly because defective cartilage cannot serve as a normal growth template during endochondral ossification. In children with this form of dysplasia, the trunk is short in relation to the rest of the body and head; they have joint arthropathy and early-onset degenerative disease of load-bearing joints.
Most people with spondyloepiphyseal dysplasia have mutations in the COL2A1 gene. The COL2A1 gene encodes instructions for making type II collagen.[1] When type II collagen is defective or deficient, cartilage cannot support normal skeletal growth, particularly at the epiphyseal growth plates.
Clinically, this explains why children with SED have a short stature but otherwise normal intelligence and organ development. Clinicians have been able to identify two forms of presentation:
- Congenital SED (SEDc) is present at birth or in early childhood
- Tarda SED (SEDt) appears later in childhood or adolescence
Epidemiology & Global Trends:: Spondyloepiphyseal Dysplasia Collagen
SED is rare. Population studies suggest the overall prevalence is about 3.4 cases per million individuals. The congenital form (SEDc) is more common because it is inherited in an autosomal dominant fashion, wherein a single defective copy of the COL2A1 gene is enough for the disease to manifest. SEDc is seen in 1 in 100,000 to 1 in 250,000 live births.[2]
SED tarda, in contrast, is usually inherited in an X-linked recessive pattern due to mutations in the TRAPPC2 gene (previously SEDL) and therefore primarily affects males, with an incidence of about 1 in 150,000 males.[3]
There are no significant geographic or racial variations in its occurrence.
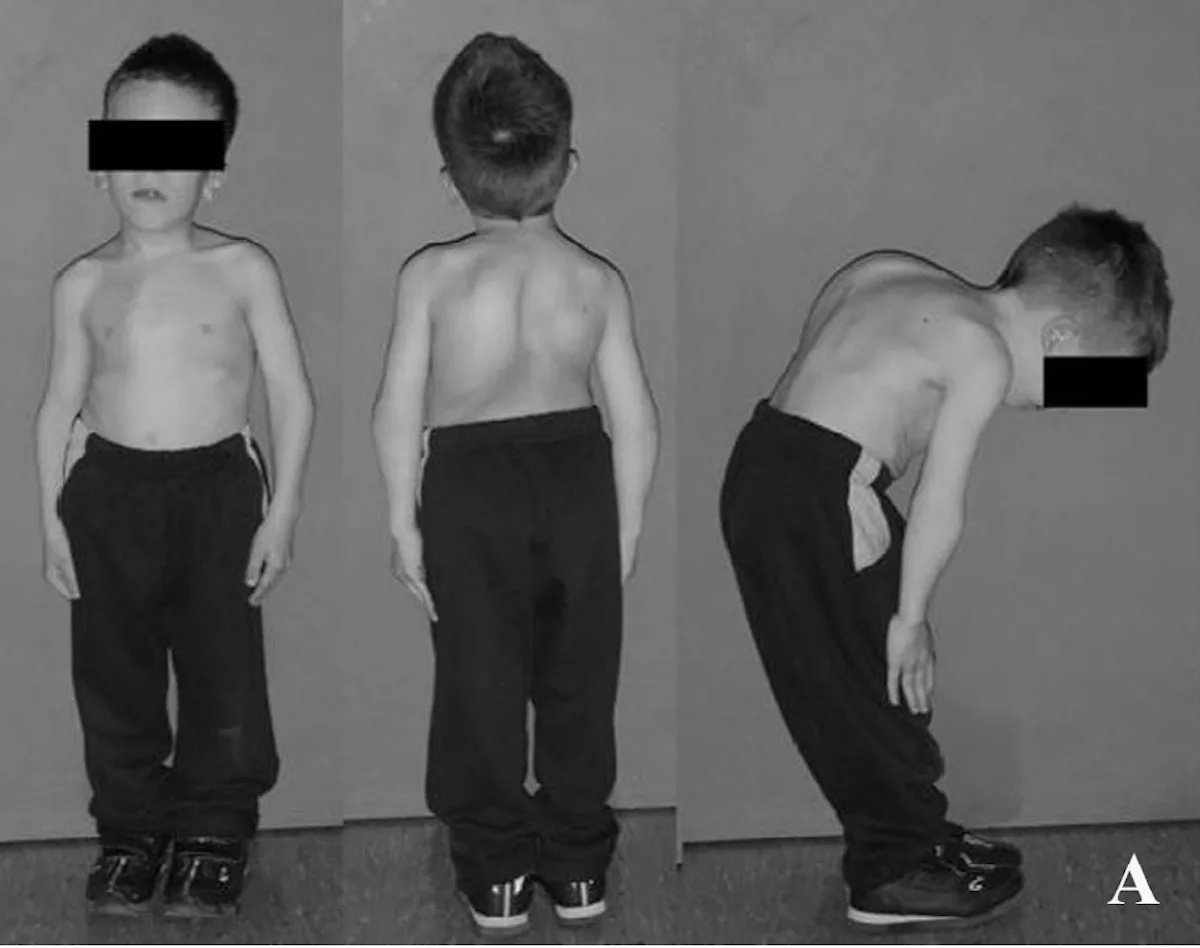
Child with spondyloepiphyseal dysplasia congenita showing short-trunk stature and chest deformity.Image by Konstantinos C. Soultanis, Alexandros H. Payatakes, Vasilios T. Chouliaras, Georgios C. Mandellos, Nikolaos E. Pyrovolou, Fani M. Pliarchopoulou, and Panayotis N. Soucacos from Rare causes of scoliosis and spine deformity: experience and particular features, via Wikimedia Commons, licensed under CC BY 2.0.
Pathophysiology:
The main defect lies in type II collagen, the key structural protein of cartilage, intervertebral discs, and some other components. The COL2A1 gene on chromosome 12q13.11–q13.2 controls the synthesis of this collagen. When it’s mutated, the result is either defective or insufficient collagen, resulting in defective cartilage, which would otherwise serve as a scaffold for bone formation, being too weak and not well-organized.
Because endochondral ossification (the process by which cartilage turns into bone) depends on that scaffold, it’s the bones formed through this specific pathway that are the most affected.
When the skeleton develops based on this defective framework, the vertebral bodies are obviously abnormal: flattened and irregular (platyspondyly). The epiphyses do not properly grow (epiphyseal dysplasia), especially in the weight-bearing joints such as the hips and knees. The affected individuals have unstable joints and are at risk for early osteoarthritis and spinal deformity.
Since type II collagen is also found in the eye, inner ear, and cartilage of the upper airway, these patients also have a risk for non-skeletal signs, symptoms, and complications. In fact, manifestations of myopia (nearsightedness), retinal detachment, and hearing impairment have a relatively high frequency.[4]
In addition, certain mutations result in features that are found in Kniest dysplasia, another type II collagen defect, as well as Stickler syndrome. These conditions are now classified as part of a type II collagenopathy spectrum.
Types of Spondyloepiphyseal Dysplasia
There are other, less common forms of SED, in addition to SED congenita and SED tarda, many of which are the result of mutations in specific genes.
| Subtype | Pattern of Inheritance | Mutated Gene | Birth Length | Age at Presentation | Key Features |
|---|---|---|---|---|---|
| SED congenita | Autosomal dominant | COL2A1 | Short | Birth or infancy | Short trunk, short trunk, flat facies, barrel chest, cleft palate (20-30%), myopia, kyphoscoliosis develops early,coxa varais common |
| SED tarda | X-linked recessive | Progressively short stature, back pain, normal face, humped back vertebrae | Normal | 8 to 15 years old | Progressively short stature, back pain pain, normal face, humped back vertebrae |
| SED with progressive arthropathy | Autosomal dominant | COL2A1 | Variable | Childhood | Early arthritis most prominent here, less severe involvement of growth plates |
| SED Kimberley type | Autosomal dominant | COL2A1 | Short | Infancy | Distinct facial features, mild to moderate spinal findings |
Spondyloepiphyseal Dysplasia vs Achondroplasia:
Both disorders cause short stature, but achondroplasia primarily affects limb length (short-limb dwarfism), whereas SED affects the trunk (short-trunk dwarfism). Achondroplasia involves FGFR3 gene mutations, not collagen defects. Other differentiating features are discussed in the image below:
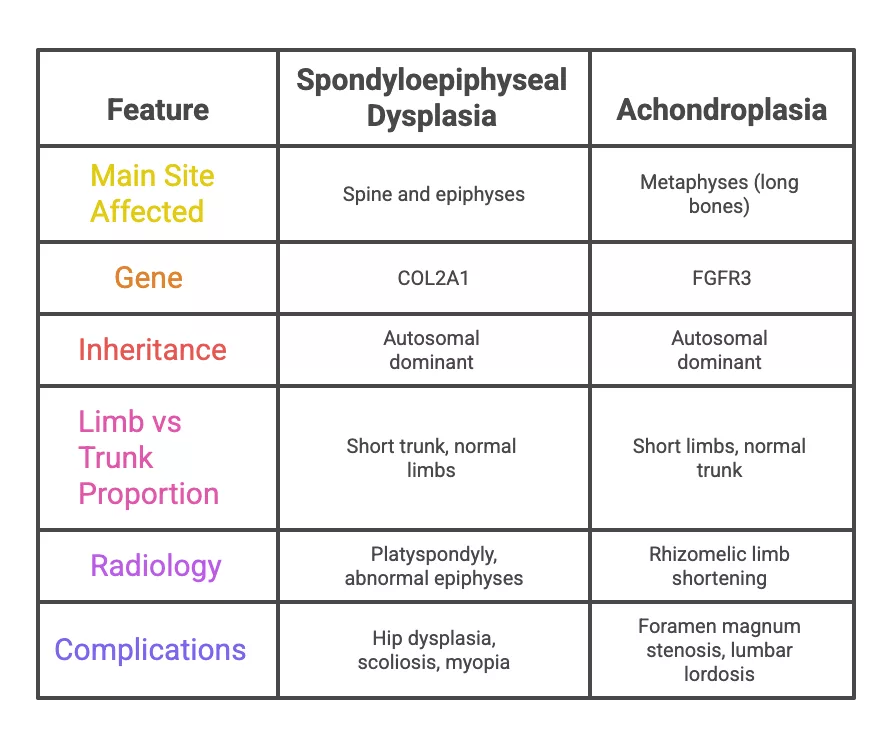
Both spondyloepiphyseal dysplasia (SED) and achondroplasia result in short stature. However, their clinical and radiologic patterns differ markedly, as summarized in this table. The main differentiation is still in the pattern of trunk vs limb shortening.
Clinical Features
The clinical features identified in spondyloepiphyseal dysplasia (SED) are influenced by the subtype. The congenital forms become obvious at the time of birth itself, while tarda types present in late childhood or adolescence. The main pathology seen in all types includes short-trunk dwarfism, joint deformities, spinal abnormalities, and ocular involvement.
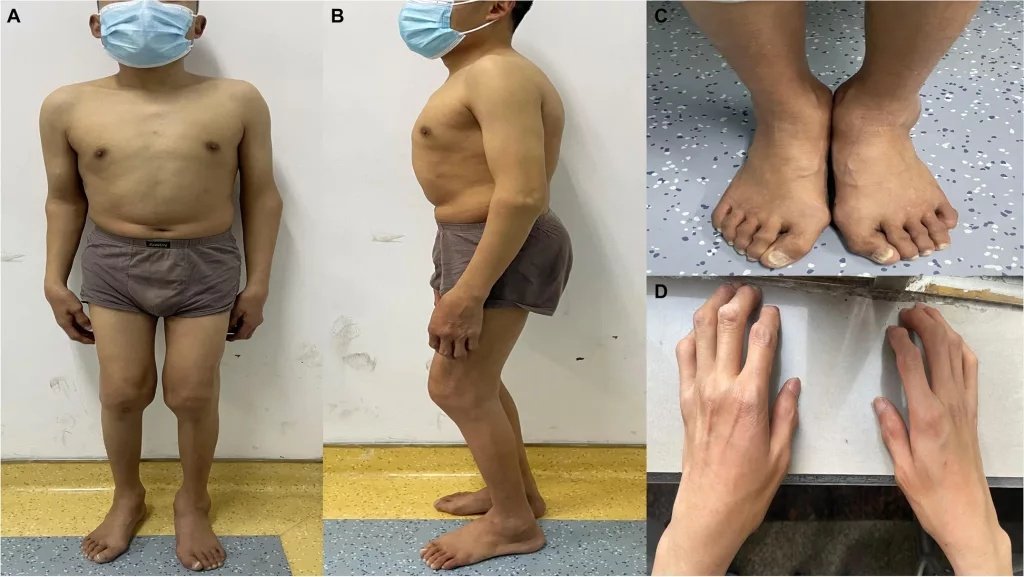
Clinical appearance of a patient with spondyloepiphyseal dysplasia.(a, b) Short trunk, barrel chest, as well as a humpback curvature. (c, d) Swelling of finger and toe joints due to epiphyseal involvement. (Image Courtesy: Chen, Z., Zhang, Z., Ye, F.et al.Multiple disc herniation in spondyloepiphyseal dysplasia tarda: A rare case report and review of the literature.BMC Musculoskelet Disord23, 1087 (2022). https://doi.org/10.1186/s12891-022-06064-4. Available fromBMC. Licenced under CC by 4.0)
1. Body Proportion
Children with SED present with short stature, as in other forms. In the congenital form, though, it is visible from birth. In the tarda forms, it develops gradually. The upper and lower limbs remain nearly proportional to each other; only the trunk is visibly short. The vertebrae are flat, especially in the thorax and lumbar regions.
As the child grows, the height still remains well below average. The final adult height of 90-130 cm is common in congenital forms. In tarda types, it’s still slightly better.
2. Spine and Posture
The spine is nearly always affected. Typical features are:
- Kyphoscoliosis or lordosis
- Atlantoaxial instability, which may compress the spinal cord. This is because the odontoid process is underdeveloped.
- Platyspondyly (flattened vertebrae on X-ray)
Because of spinal instability, even minor trauma may cause neck or upper limb weakness in some patients.
3. Joint Development
Limb shortening affects the upper limb more than the lower limb. Even in apparently normal-length limbs, the epiphyses in long bones are not fully developed. As a result, this leads to:
- Coxa vara
- Hip dislocation or limited motion
- Knee deformities (genu valgum or varum)
- Early osteoarthritis of the hips and/or knees

Neonatal presentation of spondyloepiphyseal dysplasia congenita.Radiograph of a three-hour-old infant with a short trunk, craniofacial anomalies, as well as respiratory distress, showing dysgenesis of vertebral bodies and pelvic bones, consistent with severe congenital skeletal dysplasia. (Image Courtesy: Saleem S, Anwar A, Iftikhar P M, et al. (July 08, 2019) Spondyloepiphyseal Dysplasia Congenita: A Rare Cause of Respiratory Distress. Cureus 11(7): e5101. doi:10.7759/cureus.. 5101. Available fromCureus. Licenced under CC by 3.0)
4. Facial Features
Many patients have a flat midface, low nasal bridge, and occasionally a submucous cleft palate.
There are also ocular findings sometimes because of the presence of type II collagen in the eye:
- High myopia (short-sightedness) is present in 50-80% of individuals with SEDC
- Retinal detachment (5-10% lifetime risk) can lead to permanent vision loss if not treated
5. Hearing and Lung Issues
- In SED, patients report both conductive and sensorineural types ofhearingloss; however:
- Some patients develop restrictive lung disease due to thoracic deformity and scoliosis. Respiratory insufficiency is extremely rare, but the decreased lung capacity may raise the risk of surgery.
6. Neurological Findings
Many cases are reported with cervical compression due to instability of the cervical spine. In rare cases, there have been incidents of sudden death. But most cases will present with neck pain, muscle weakness, and gait disturbance. Once a clinician notices a neurology-related symptom, regular examination becomes compulsory to prevent irreversible damage.
Diagnosis of Spondyloepiphyseal Dysplasia
Spondyloepiphyseal dysplasia (SED) is diagnosed with a combination of genetic testing, imaging studies, and clinical evaluation. Some other skeletal dysplasias can sometimes have similar findings, so part of the process of evaluation is to make sure those conditions can be ruled out and to confirm that SED is the likely diagnosis.
1. Clinical Evaluation
Physicians usually start the diagnostic process by taking a careful growth history and then performing a physical examination.
Clinical features that might prompt consideration of this diagnosis include:
- A short trunk and average limb length
- Spinal curvature: kyphosis, lordosis, or scoliosis
- Hip deformity or limited joint mobility
If these features are noted on physical examination, it raises suspicion, and radiologic studies are performed next.
2. Imaging Studies
The next important diagnostic criterion after physical evaluation is based on radiological findings.[5]
Spinal Findings
- Platyspondyly: Vertebral bodies are flattened
- Anterior wedging of vertebrae, which obviously translates as kyphosis or lordosis
- Biconcave endplates and irregular vertebral contours.
- In some severe congenital cases, atlantoaxial instability may also be seen on cervical spine X-rays.
- SED tarda shows a central vertebral hump on lateral view: Here vertebrae appear to have humped posteriorly with anterior rounding. Thus, SED tarda is differentiated from SED congenita and other dysplasias
Recommended Imaging Views
- Lateral, anteroposterior (AP) spine views
- AP pelvis view + AP lower extremity views
- Lateral cervical spine (with flexion–extension views if atlantoaxial instability is being suspected)
A full skeletal survey in children is best for detecting early abnormalities.
MRI is done to rule out spinal cord compression, especially at the C1–C2 level. This also helps in knowing the status of intervertebral discs, which are thinned or irregular in shape due to abnormal cartilaginous development.[6]
In very advanced cases, even a CT scan might be advised.
Pelvis and Hip
Pelvic radiographs commonly show:
- Coxa vara (femoral neck–shaft angle < 120°)
- Late appearance and ossification of the femoral heads and acetabula
- Flat, shallow hip sockets, which can lead to dislocation and early arthritis
Long Bones and Limbs
- Irregular, small epiphyses
- Sometimes enlarged metaphyses
- Incongruity of articular surfaces of knees and ankles (translation and rotation), leading to valgus, varus, or windswept deformities
- Progressive joint space narrowing
Skull and Facial Bones
- Flat nasal bridge
- Short skull base
- Occasional foramen magnum narrowing

Radiologic findings in spondyloepiphyseal dysplasia congenita (SEDC) with COL2A1 variants:X-rays show vertebral flattening with kyphosis, lumbar lordosis, as well as occasional scoliosis (a–l). Hip images demonstrate flattened acetabular roofs, dysplastic or compressed femoral heads, as well as shortened femoral necks (f–i). On the other hand, parental carriers display milder spinal and hip changes. (Image Courtesy: Zheng W-B, Li L-J, Zhao D-C, et al. Novel variants in COL2A1 causing rare spondyloepiphyseal dysplasia congenita. Mol Genet Genomic Med. 2020;8:e1139. https://doi.org/10.1002/mgg3.1139. Available fromResearch Gate.Licenced under CC by 4.0)
3. Genetic Testing
The most accurate mode of diagnosis is mutation identification in:
- COL2A1 gene → SED congenita (autosomal dominant)
- TRAPPC2 gene → SED tarda (X-linked recessive)
Genetic test results confirm the type, help guide counseling, and differentiate SED from similar disorders such as pseudoachondroplasia or Kniest dysplasia.
Treatment of Spondyloepiphyseal Dysplasia
Spondyloepiphyseal dysplasia (SED) demands an expert-led coordinated multispecialty approach. There is no definitive way to cure SED, but the treatment helps improve the quality of life, ameliorate presenting symptoms, and stop the worsening of signs and symptoms.
1. Orthopedic Management
This is meant to stabilize the spine, preserve joint function, and also for making sure that any deformities don’t deteriorate.
a. Cervical spine:
- Atlantoaxial instability poses a serious risk and, therefore, close observation and flexion-extension X-rays need to be done.
- MRI is recommended if the patient develops any neurological signs (cord compression).
- Spinal fusion surgery can also be performed in some cases (this procedure fuses the affected vertebrae together in order to prevent any cord compression).[7]
b. Hip and lower limbs:
- If coxa vara or hip dislocation is present, osteotomy should be considered (may correct hip deformity and relieve hip pain).
- Conservative treatment (physical therapy, weight control, NSAIDs) should precede surgery.
- Total hip replacement is often needed in the 30s or 40s (due to early arthritis).
c. Spine:
- Children need to be monitored for scoliosis.
- For curves > 25°, braces are used, while > 45–50° or progressive deformity signals surgery.
2. Medical and Supportive Therapy
- No specific drug therapy is of benefit in correcting the collagen defect. Initially, pain medication (acetaminophen, NSAIDs) may assist in relieving arthralgias.
- Growth hormone therapy has a limited role, since the primary dysfunction in the growth plates lies in the tissue itself and is not a hormonal issue.
- Regular evaluation to monitor cervical spine and pulmonary dysfunction is essential.
- CPAP may need to be used in severe cases to assist with ventilation in cases of chest wall dysfunction and hypoventilation.[8]
3. Vision and Hearing Care
Routine vision screening and yearly retinal examination for children with high myopia. Regular audiology check-ups and use of hearing aids improve learning and communication.
4. Physical Therapy and Counselling
- Guided physiotherapy helps patients retain their flexibility and avoid contractures due to disuse. Similarly, postural training to reduce the risk of scoliosis and back pain has been seen to be effective.
- If a family is already known to have a mutation, genetic counseling can help understand the inheritance pattern and recurrence risk. Prenatal testing and early screening can be offered.
- Short stature, need for multiple surgeries, and chronic pain can absolutely take a toll on mental health as well, which would need therapy.
Life Expectancy in Spondyloepiphyseal Dysplasia
SED does not affect a patient’s lifespan much. Even mobility isn’t often affected too much; in fact, patients are usually able to walk without disability until adulthood, although joint pain and premature osteoarthritis are common. Regular physiotherapy to minimize strain on joints and disuse atrophy, management of varicose veins, regular ophthalmologic follow-up, and treatment of joint problems by orthopedists improve quality of life over the years.
Final Word
Spondyloepiphyseal dysplasia (SED) is a rare genetic condition, and unfortunately, as of right now, there is no treatment available for a cure. However, genetic testing, orthopaedic management, and physical therapy have all helped improve the prognosis to some extent.
With the understanding of the disease process, monitoring and proper management, i.e., spinal fusion surgery, physical therapy, etc, most of the patients may lead an efficient life. In the future, with more understanding of collagen biology and gene-based therapy, a more specific treatment might be possible.
References
[1] Li, S., Zhou, H., Qin, H., Guo, H., & Bai, Y. (2013). A novel mutation in the COL2A1 gene in a Chinese family with Spondyloepiphyseal dysplasia congenita.Joint Bone Spine,81(1), 86-89. https://doi.org/10.1016/j.jbspin.2013.06.010
[2] Saleem, S., Anwar, A., Iftikhar, P. M., Anjum, Z., & Tariq, Z. (2019). Spondyloepiphyseal Dysplasia Congenita: A Rare Cause of Respiratory Distress. Cureus, 11(7), e5101. https://doi.org/10.7759/cureus.5101
[3] https://medlineplus.gov/genetics/condition/x-linked-spondyloepiphyseal-dysplasia-tarda/#frequency
[4] Gregersen PA, Savarirayan R. Type II Collagen Disorders Overview. 2019 Apr 25 [Updated 2024 Oct 24]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK540447/
[5] Mousavi F, Knipe H, Silverstone L, et al. Spondyloepiphyseal dysplasia. Reference article, Radiopaedia.org (Accessed on 14 Oct 2025) https://doi.org/10.53347/rID-54316
[6] Offiah, A. C., & Hall, C. M. (2020).The radiologic diagnosis of skeletal dysplasias: Past, present and future.Pediatric Radiology, 50(11), 1650-1657. https://doi.org/10.1007/s00247-019-04533-y
[7] Serhan Er, M., Abousamra, O., Rogers, K., Akyol, Y., Palocaren, T., Takemitsu, M., Campbell, J. W., & Mackenzie, W. G. (2017). Upper Cervical Fusion in Children With Spondyloepiphyseal Dysplasia Congenita. Journal of pediatric orthopedics, 37(7), 466–472. https://doi.org/10.1097/BPO.0000000000000702
[8] Nguyen, D. B., Khirani, S., Griffon, L., Baujat, G., Michot, C., Marzin, P., Rondeau, S., Luscan, R., Couloigner, V., Pejin, Z., Zerah, M., Cormier-Daire, V., & Fauroux, B. (2021). Sleep-disordered breathing and its management in children with rare skeletal dysplasias. American journal of medical genetics. Part A, 185(7), 2108–2118. https://doi.org/10.1002/ajmg.a.62236