
{kind=link}

Temporal Arteritis Headache Temporal arteritis, or Giant cell arteritis, is a chronic inflammatory disorder that develops swelling and inflammation of the walls of the arteries. This leads to narrowing or blockage of the arteries, which decreases the supply of blood to vital organs and tissues. Such a decrease in blood flow may cause tissue damage and severe complications, like permanent loss of vision, stroke, and potentially life-threatening cardiovascular complications. The most common symptom of TA is a severe, throbbing headache.
Although the disease is known as temporal arteritis, as temporal arteries are usually involved, in reality, the inflammation may also occur in other blood vessels in the body. It usually affects women around or above 50 years of age. The term giant cell is used to describe a particular cell in the immune system that occurs in the inflamed arterial walls when viewed under a microscope. The disease may also involve the aorta and its major branches. In the case of the aorta, the disease is known as giant cell aortitis.
The condition is defined as either an autoimmune or autoinflammatory disease. However, it is more accurately classified as an immune-mediated vasculitis, i.e, the immune system of the body malfunctions and targets healthy blood vessels. The inflammatory process of temporal arteritis involves various layers of the arterial wall, such as the outer lining, middle layer, and inner lining. The inflammation may result in the development of granulomas, i.e, clumps of immune cells, which are characteristic of the disease under a microscope.
Recognizing the Symptoms: Temporal Arteritis Headache
Early diagnosis and treatment of temporal arteritis requires the identification of its symptoms.
Primary Symptoms
New, persistent headache is the most typical symptom of temporal arteritis, and it normally involves the temples. It is very severe and throbbing, which is not similar to any other headaches that have ever been experienced by the patient. Patients often complain of tenderness when palpating the scalp or temples, and some of them complain that the temporal arteries are swollen or rope-like under the skin. Scalp pain may even be so intense that hair brushing or even putting a head on a pillow is painful.

Illustration of temporal arteritis (giant cell arteritis) highlighting inflamed temporal arteries and arterial wall thickening.
Jaw claudication is also another typical symptom of temporal arteritis. This is the pain or tiredness of the muscles in the jaw that appear during eating or speaking. The pain usually becomes more pronounced with further usage of the jaw and does improve with rest. This symptom is a strong indicator of temporal arteritis when it is present. It is used to differentiate between TA and other conditions that would cause headaches.
Vision-Related Symptoms
One of the most severe temporal arteritis symptoms and a medical emergency is vision issues. These may range from temporary vision impairment to sudden and permanent loss of vision. Patients can have either double vision, blurred vision, or the feeling that a curtain is being dragged in one eye.
Others complain of a temporary loss of vision that intermittently occurs and is called amaurosis fugax, which is a very serious warning sign of imminent irreversible blindness until treatment is administered promptly.
General Systemic Symptoms
In addition to the cranial symptoms, the temporal arteritis usually has the general ones that may complicate the diagnosis. Flu-like symptoms, such as persistent fatigue and weakness, unexplained weight loss, low-grade fever, loss of appetite, night sweats, and the feeling of being unwell, characterize many patients.
Associated Conditions
Temporal arteritis is closely related to a disease, polymyalgia rheumatica, which causes pain and stiffness of the muscles surrounding the shoulders, neck, and hips. Symptoms of polymyalgia rheumatica are also present in about 40 to 60 percent of patients with temporal arteritis.
In cases of involvement of the larger blood vessels outside the head, patients report limb claudication or pain or fatigue of the arms or legs during exercise. Asymmetries in blood pressure between arms and no or weak pulses in the extremities may also point to involvement of large vessels, which is even more dangerous and may need long-term observation.
Risk Factors and Causes
The specific cause of temporal arteritis is still not known, but some factors have been identified that can lead to this condition. The knowledge of these factors can assist in identifying those who are at greater risk and possibly in informing the prevention strategies.
Age Factor
The biggest risk factor of temporal arteritis is age. The condition is nearly always present in people above the age of 50 years, with an average age of onset of approximately 70 years. Its prevalence rises drastically as age advances, with the highest prevalence between the ages of 70 and 80 years.
Genetic Predisposition
Genetic factors that predispose to temporal arteritis have been determined. Some human leukocyte antigen types, especially HLA-DRB1 04, are notably higher in patients with the disorder, especially among individuals of Northern European origin. Nevertheless, genetics alone is not sufficient to cause temporal arteritis, and so the disease requires some environmental or infectious stimulus to occur.
Gender and Ethnicity
Temporal arteritis is about two to three times more frequent in women than in men. But when men develop the condition, they seem to be at a greater risk of getting serious complications, especially vision loss.
Temporal arteritis mostly attacks individuals of Northern European, especially Scandinavian origin. The prevalence of the condition is lower in African, Asian, and Hispanic populations, which indicates that both genetic and environmental factors have significant roles in the development of the disease.
Potential Triggers
Research has identified traces of the varicella-zoster virus, the virus that causes chickenpox as well as shingles, in a large percentage of temporal artery biopsies of those with the condition. This observation implies that the inflammatory cascade is active in vulnerable people due to viral infection. Nonetheless, there is a need for further studies to establish this association and how infections can cause chronic arterial inflammation.
Diagnostic Approach for Temporal Arteritis
The first stage of the diagnostic process is the medical history and physical examination. The doctors will enquire about the symptoms, such as their time of onset, severity, and change over time. The physician further checks the temporal arteries and palpates to check for tenderness, swellings, and a weak pulse. The temporal arteries can be nodular, thick, or bulbous. Your doctor will check your blood pressure in both arms to identify any asymmetry, and also observe your eyes to identify slow blood flow.
Laboratory Testing
The following blood tests can help to substantiate the diagnosis of temporal arteritis.
- ESR: more than 60 millimeters per hour, and in some cases, it is more than 100.
- CRP is usually high in temporal arteritis.
- Complete blood counts
Imaging Studies
The use of modern imaging methods has become a very significant part of the diagnosis of temporal arteritis.
- A typical observation visible on Color Doppler ultrasound of the temporal arteries is the halo sign, which appears as a dark ring around the vessel wall of the artery, indicating swelling of the vessel wall.
- For inflammation of the arterial walls and blood flow through the arteries, magnetic resonance imaging and angiography are helpful.
- PET scans have the advantage of identifying inflammation in large blood vessels within the body, particularly effective in finding large vessel involvement
Temporal Artery Biopsy
The gold standard in the confirmation of temporal arteritis is the temporal artery biopsy. This is done with the help of local anesthesia, and a piece of the temporal artery, which is usually 1.5 to 3 centimeters in length, is excised to be examined. A pathologist examines the tissue sample to locate typical signs of inflammation, including giant cells, granulomas, and foci of damage to the layer of the artery. Nonetheless, a negative biopsy does not fully exclude the possibility because the distribution of inflammation is not uniform in the arteries.
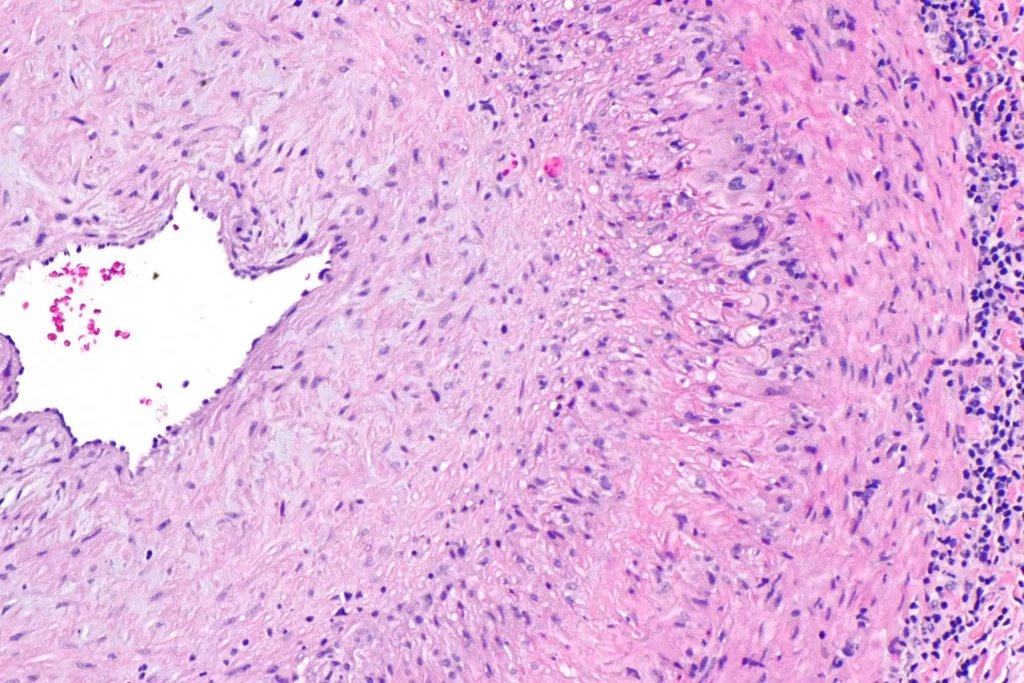
Intermediate-magnification H&E micrograph of a temporal artery biopsy showing giant cell arteritis, with a narrowed arterial lumen and multinucleated giant cells at the intima–media junction.CCBY-SA 3.0, Wikimedia Commons.
Treatment Strategies
Temporal arteritis must be treated immediately when it is suspected or even before it is confirmed through biopsy to avoid irreversible complications. The main aim of treatment is to decrease inflammation within a short period and to avoid organ damage.
Corticosteroid Therapy
The cornerstone of treatment of temporal arteritis is high-dose corticosteroids, which are usually prednisolone or prednisone. The treatment normally starts at 40 to 60 milligrams per day, or, where vision is involved, the treatment may start by taking even greater doses. Others with severe visual symptoms are on intravenous methylprednisolone for a few days and then switch to oral therapy.
Symptomatic improvement in most patients is reported dramatically in a matter of days after corticosteroid treatment. The corticosteroid dose is tapered slowly after the first high-dose period, which normally lasts a few weeks. The majority of patients need one to two years of therapy, although others may need to take corticosteroids longer.
Additional Medications
Due to the severe side effects that accompany the long-term use of corticosteroid therapy, immunosuppressive agents are commonly combined with corticosteroids so that lower doses of corticosteroid can be used.
- Methotrexate is useful in the suppression of the immune system, and corticosteroids may be tapered faster.
- Tocilizumab is a more recent and specific biological drug that inhibits interleukin-6, one of the main inflammatory substances in the development of temporal arteritis. Studies have indicated that tocilizumab can greatly improve the outcome and decrease the use of corticosteroids.
- Aspirin in low doses is commonly prescribed by many doctors to minimize the threat of blood clots and ischemic complications.
- Proton pump inhibitors to avoid corticosteroid-related gastrointestinal issues.
- The supplementation with calcium, vitamin D, and the use of bisphosphonate drugs will prevent the bone loss and osteoporosis caused by the chronic use of corticosteroids.
Potential Complications
Temporal arteritis may cause severe and even fatal complications in the absence of early diagnosis and treatment.
Vision Loss
Vision loss is the most adverse complication of temporal arteritis. Until corticosteroid therapy became routine, as many as half of the patients would undergo a certain level of loss of vision. Now that it is treated immediately, this risk has been minimized to about one percent or lower.
The loss of vision is rather sudden and painless, usually in one eye, but may also involve both eyes in case of a delayed treatment. In patients who receive treatment within 24 hours of vision change, about 58 percent of patients have visual improvement.
Cardiovascular Complications
One of the potential serious complications is stroke as a result of inflammation occurring in the carotid arteries or the vertebral arteries that carry blood to the brain. Temporal arteritis may affect the aorta and cause aortic aneurysm, dissection, or rupture. Research indicates that patients who have developed a temporal arteritis are at risk of developing aortic aneurysms about twice as often as their age mates. The coronary arteries may also be subject to the inflammatory process, which raises the chance of a heart attack.
Adverse Effects of the Treatment
The prolonged corticosteroid use may result in osteoporosis, weight gain, a rise in blood sugar and diabetes, high blood pressure, cataracts, glaucoma, increased vulnerability to infections, mood changes, muscle weakness, and skin thinning. These side effects render the importance of steroid-sparing medications.
Prognosis and Life Expectancy
With the advent of corticosteroid therapy, the prognosis of patients with temporal arteritis has improved significantly. Through early diagnosis and proper treatment, the majority of patients are free of their symptoms in a few days. With the start of proper treatment in time, the chances of severe complications are minimal. The majority of patients can taper off corticosteroids in one to two years of treatment, although it takes some patients longer. During treatment, relapses may take place, especially in the first year, and with the reduction of corticosteroid doses. In case of a relapse, reintroduce the corticosteroid dose to manage the symptoms.
Long-term studies have demonstrated that, due to proper care, patients with temporal arteritis have a life expectancy that is the same as that of the general population. The standardised mortality ratio is about 1.0, that is, patients with temporal arteritis die on average as long as persons without the condition. Although there is a slight increase in mortality risk during the first five years after diagnosis, these risks decrease with time.
Conclusion
Temporal arteritis is a severe but curable condition mainly afflicting people at the age of 50 and above. Knowing the symptoms, the need to consult a doctor in time, and following the prescribed treatment will help avoid complications and stay healthy. Any person who is above 50 years and develops new headaches, vision changes, or pain in the jaw during chewing must have an urgent medical examination. Timely diagnosis and treatment will help avoid severe complications and enable patients to remain independent and enjoy a good quality of life.
References
[1] Horton BT, Magath TB. Arteritis of temporal vessels: report on 7 cases. Proc Staff Meet Mayo Clin. 1937;12:548-553.
[2] Weyand CM, Goronzy JJ. Giant-cell arteritis and polymyalgia rheumatica. N Engl J Med. 2014;371(1):50-57.
[3] Hunder GG. The early history of giant cell arteritis and polymyalgia rheumatica: first descriptions to 1970. Mayo Clin Proc. 2006;81(8):1071-1083.
[4] Salvarani C, Pipitone N, Versari A, Hunder GG. Clinical features of polymyalgia rheumatica and giant cell arteritis. Nat Rev Rheumatol. 2012;8(9):509-521.
[5] Dejaco C, Singh YP, Perel P, et al. 2015 Recommendations for the management of polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. 2015;74(10):1799-1807.
[6] Crowson CS, Matteson EL, Myasoedova E, et al. Contemporary prevalence estimates for giant cell arteritis and polymyalgia rheumatica, 2015. Semin Arthritis Rheum. 2017;47(2):253-256.
[7] Schmidt WA, Kraft HE, Vorpahl K, Völker L, Gromnica-Ihle EJ. Color duplex ultrasonography in the diagnosis of temporal arteritis. N Engl J Med. 1997;337(19):1336-1342.
[8] Karahaliou M, Vaiopoulos G, Papaspyrou S, et al. Colour duplex sonography of temporal arteries before decision for biopsy: a prospective study in 55 patients with suspected giant cell arteritis. Arthritis Res Ther. 2006;8(4):R116.
[9] Sharma P, Srinivasan P. Temporal artery biopsy in giant cell arteritis: clinical perspectives and histological patterns. Front Med (Lausanne). 2024;11:1453462.
[10] Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology (Oxford). 2017;56(4):506-515.
[11] Stone JH, Bao M, Han J, et al. Long-term effect of tocilizumab in patients with giant cell arteritis: open-label extension phase of the Giant Cell Arteritis Actemra (GiACTA) trial. Lancet Rheumatol. 2021;3(5):e328-e336.
[12] Chen JJ, Leavitt JA, Fang C, Crowson CS, Matteson EL, Warrington KJ. Evaluating the incidence of arteritic ischemic optic neuropathy and other causes of vision loss from giant cell arteritis. Ophthalmology. 2016;123(9):1999-2003.
[13] Maleszewski JJ, Younge BR, Fritzlen JT, et al. Clinical and pathological evolution of giant cell arteritis: a prospective study of follow-up temporal artery biopsies in 40 treated patients. Mod Pathol. 2017;30(6):788-796.
[14] Martinez-Lado L, Calviño-Díaz C, Piñeiro A, et al. Relapses and recurrences in giant cell arteritis: a population-based study of patients with biopsy-proven disease from northwestern Spain. Medicine (Baltimore). 2011;90(3):186-193.