
 or RH fever is best known as the leading cause of Rheumatic Heart Disease (RHD), which remains...){kind=link}

Hidden Threat Sore Acute Rheumatic Fever (ARF) or RH fever is best known as the leading cause of Rheumatic Heart Disease (RHD), which remains the most common cause of acquired heart disease in children and young adults worldwide, but particularly in developing nations and marginalized communities. It begins with a sore throat, but can end with cardiac damage.
Rheumatic fever is a disease that represents a paradox in that the immune system, instead of fighting an infection, starts targeting the body instead. In most high-income countries, the prevalence has dropped, but there are still incidences of resurgence in some communities.
What Causes Rheumatic Fever?: Hidden Threat Sore
At its core, rheumatic fever is a delayed, non-suppurative autoimmune response to a Group A β-hemolytic Streptococcus (GAS) infection, commonly called strep throat.
Unlike a typical infection, where the bacteria attack the body directly, the pathology of RH fever is driven by mistaken identity: molecular mimicry. The body’s immune system produces antibodies to target the ‘M-proteins’ on the surface of the streptococcus bacteria.[1]
Unfortunately, these proteins look very much like the proteins in our own heart, joints, and brain. So the immune system mistakenly attacks its own healthy tissue, specifically in these organs, leading to the multisystem inflammation of RH fever. This is usually 2 to 4 weeks after an untreated or poorly treated strep infection.
Epidemiology and Global Impact
Statistically, the burden of ARF is staggering. Rheumatic fever is most common in children aged 5 to 14 years. In high-income countries, the rate is less than 2 per 100,000. In endemic regions like South Asia and Sub-Saharan Africa, that number can be as high as 51. An interesting trend is that certain populations in high-income countries, including Indigenous communities in Australia, experience some of the highest recorded rates, reaching 150–380 per 100,000 children.[2]
According to the World Health Organization (WHO), Rheumatic Heart Disease (RHD) affects over 40 million people worldwide. It kills 300,000 to 400,000 people each year, most often from heart failure or stroke.[3]
Presentation & Diagnosis of Rheumatic Fever
Clinicians use the Revised Jones Criteria to establish a diagnosis of ARF. This requires objective evidence of a prior Group A Streptococcus infection (via throat culture or elevated ASO titers) plus two major criteria, or one major and two minor criteria.
| Category | Major Criteria | Minor Criteria |
|---|---|---|
| Low-Risk Populations | • Carditis (Clinical or Subclinical)• Polyarthritis• Chorea• Erythema Marginatum• Subcutaneous Nodules | • Polyarthralgia• Fever (≥ 38.5°C)• ESR ≥ 60 mm/hr and/or CRP ≥ 3.0 mg/dL• Prolonged PR Interval |
| Moderate/High-Risk Populations | • Carditis (Clinical or Subclinical)• Monoarthritis or Polyarthritis• Polyarthralgia• Chorea• Erythema Marginatum• Subcutaneous Nodules | • Monoarthralgia• Fever (≥ 38°C)• ESR ≥ 30 mm/hr and/or CRP ≥ 3.0 mg/dL• Prolonged PR Interval |
The Revised Jones Criteria for Acute Rheumatic Fever: Diagnosis requires evidence of preceding Group A Strep infection + 2 Major OR 1 Major & 2 Minor criteria.4Gewitz MH, Baltimore RS, Tani LY, Sable CA, Shulman ST, Carapetis J et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015;131:1806–18.
ASO Titers and ESR
There’s no pathognomonic blood test; we rely on the lab to provide two critical values:
- We look for Antistreptolysin O (ASO) titers. A significantly elevated value tells us that the body recently fought a strep infection.
- Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) aren’t specific to RH fever, but they indicate an active inflammatory response in the body.
Major Criteria:
- Carditis: A hallmark of rheumatic fever is inflammation of the heart muscle (endocardium, myocardium, or pericardium) and valves. In case of valves, this inflammation leaves the valves with permanent scarring. This scarring disrupts the functioning and often leads to permanent valvular regurgitation or stenosis. The mitral valve is more commonly affected than the others.[4]
- Migratory Polyarthritis: The most common feature is intense pain and swelling in large joints (knees, ankles, elbows) that ‘migrates’, meaning it moves from one large joint (like the knee) to another (the ankle or elbow) over several days.
- Sydenham’s Chorea: Chorea is involuntary, purposeless, jerky movements, especially of the hands and face. An interesting feature about RH fever is that chorea appears months after the initial infection. In school-going children, this can often manifest as a sudden, inexplicable deterioration in handwriting or emotional lability (unusual crying or irritability).
- Subcutaneous Nodules: Small, firm, painless, under-the-skin bumps that often develop near bony surfaces, such as the shins or spine.
- Erythema Marginatum: The classic rheumatic fever rash. It consists of transient, non-itchy, pinkish-red, map-like patches. It has a ringed character which consists of a non-pruritic erythematous ring area with a pale center, and the border expands outwardly. It is worsened by heat, like a hot water shower. The rash most often occurs on the trunk and inner sides of the limbs.

The classic rheumatic fever rash: erythema marginatum covering the upper arm: map-like patches with a red border and pale center (Image courtesy: Cole Ettingoff viaWikipedia Commons)
Minor Criteria:
We call these minor because they aren’t specific enough to point towards ARF in the absence of major clinical signs. But to a medical professional, the minor criteria are equally telling:
- Fever (typically ≥ 38.5°C).
- Arthralgia (joint pain without the visible swelling or redness seen in arthritis).
- Elevated inflammatory markers (ESR or CRP).
- ECG changes, specifically a prolonged PR interval (delay in the electrical conduction of the heart), a subtle sign that the heart muscle is under stress.
Recognizing the Signs of Rheumatic Fever
An inadequately treated infection is what majorly leads to rheumatic fever, and if not timely diagnosed, could lead to cardiac damage. As such, early detection could prove a miracle against complications. The following signs after a sore throat should alert parents and caregivers to visit a physician immediately:
- Joint pain that migrates from one limb to another (over 24-48 hours).
- Shortness of breath, even at rest, chest pain, or a persistent dry cough (signs of carditis).
- Unusual fatigue or a racing heart (palpitations).
- Flat, ring-like rashes on the trunk or arms.
- Sudden, uncontrollable movements or changes in handwriting.

Erythema marginatum in a Nigerian adolescent girl with acute rheumatic fever, showing patches with pale centers and raised borders (Image courtesy: Animasahun, B.A., Lawani, F.O., & Lamina, M.O. Erythema marginatum: an uncommon presentation of acute rheumatic fever in a Nigerian adolescent girl—a case report. Egypt Pediatric Association Gaz 69, 22 (2021). Available fromSpringerand licensed under CC by 4.0)
Microscopic Findings
To truly understand why the heart damage in RH fever is so persistent, one has to look at the cellular level. While the joint inflammation is transient and leaves no trace, the heart undergoes specific structural changes.
The hallmark of this is the Aschoff body.[5] These are localized areas of interstitial inflammation within the heart muscle (myocardium). If you were to examine these under a microscope, you would see:
- Fibrinoid necrosis (small areas of dead collagen and tissue)
- Anitschkow cells (enlarged macrophages with characteristic caterpillar-like nuclei)
- Lymphocytic infiltration
As these Aschoff bodies heal, they don’t return to normal tissue; they turn into fibrous scar tissue, characteristic of Rheumatic heart disease.
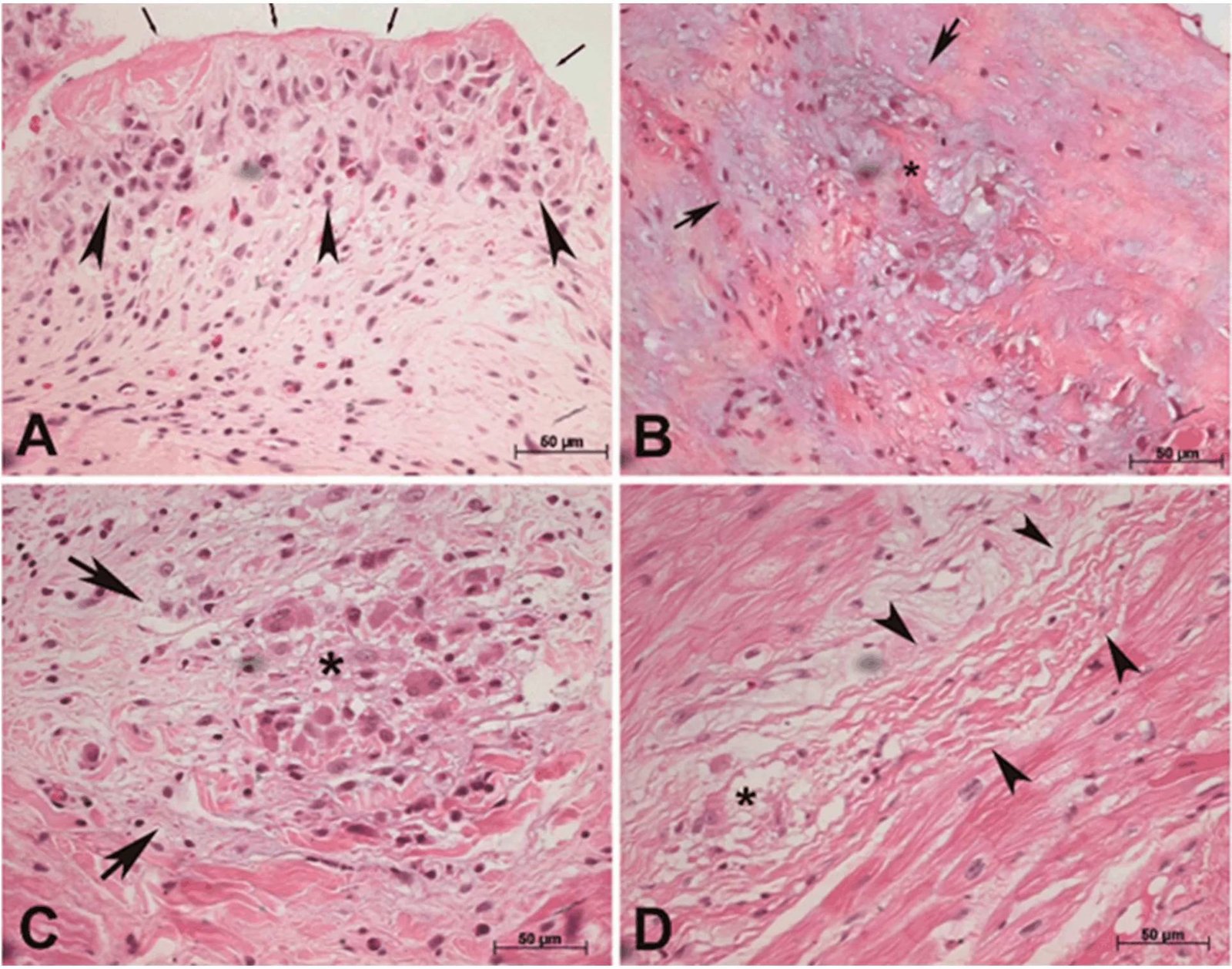
The Histological Evolution of Rheumatic Heart Disease (H&E Stain, 400x): (A) Acute Vegetation: Showing fibrinoid necrosis (arrows) and inflammatory infiltration in the aortic valve. (B) Exudative Stage: Early-phase Aschoff body with collagen fragmentation and tissue edema (*). (C) Proliferative Stage: A mature myocardial granuloma featuring pathognomonic multinucleated Aschoff cells (arrows). (D) Cicatricial Stage: The healing phase where active inflammation is replaced by permanent fibrosis and scarring (arrowheads). (Image courtesy: Vieira, P. P. A. C., Pereira, R. F., Branco, C. E. B., Rosa, V. E. E., Vieira, M. L. C., Demarchi, L. M. M. F., Silva, L. S., Guilherme, L., Tarasoutchi, F., & Sampaio, R. O. (2023). Incidental Diagnosis of Rheumatic Myocarditis during Cardiac Surgery—Impact on Late Prognosis. Diagnostics, 13(20), 3252. Available fromMDPIand licensed under CC by 4.0)
Treatment for Rheumatic Fever
As medical professionals, when we discuss the cure for rheumatic fever, we look at three distinct goals: treating the initial strep infection, the resulting autoimmune fever, or preventing a recurrence.
Primary Prevention
For rheumatic fever, the best treatment is prevention. That means to try to never let it develop in the first place. If a patient is diagnosed with strep throat, a full 10-day course of oral Penicillin (or a single intramuscular injection) kills the bacteria before the immune system can begin its ‘mistaken identity’ attack on the heart and joints.[6]
Treating the Acute Episode
In case the autoimmune response has already started, i.e., the patient is now showing clinical features of rheumatic fever like joint pain or carditis, the focus shifts to management.
- Even if the sore throat is gone, we give antibiotics to get rid of every trace of the Streptococcus bacteria, so the immune system cannot be triggered.
- Since the fever is an autoimmune reaction (not a direct bacterial attack), we use high-dose Aspirin or Naproxen to manage the joint inflammation and fever. If the heart has been involved (carditis), corticosteroids like Prednisolone can be introduced to reduce heart inflammation.
These medications stop the symptoms; they obviously do not reverse the autoimmune process; they simply wait for it to burn out. The goal at this stage is to protect the organs.
Secondary Prevention
This is the most critical stage for a patient who has already had one bout of rheumatic fever. This single bout of ARF makes one highly susceptible to recurrences.
Repeated episodes have the potential to be more severe, which exponentially increases heart damage, so patients are put on continuous prophylaxis, usually a monthly injection of Penicillin G Benzathine. This continues for years (often until age 21 or for 10 years after the last attack) to ensure the heart is not damaged further by a second or third episode of RH fever.[7]
Takeaway
Rheumatic fever is entirely preventable. The dramatic progression from a simple sore throat to permanent heart valve damage has to be disrupted. The cure begins with complete treatment of every strep throat infection with a full course of antibiotics.
As the old medical adage goes, Rheumatic Fever licks the joints but bites the heart. While the intense pain in the knees and elbows will eventually fade without leaving a trace, the damage to the heart valves is often permanent.
If you or your child have fever, migrating joint pain, or a circular rash after a sore throat, rush to the doctor to get evaluated as soon as possible. Timely clinical intervention is the only way to protect the heart from lifelong complications.
References
[1] Cunningham M. W. (2014). Rheumatic fever, autoimmunity, and molecular mimicry: the streptococcal connection. International reviews of immunology, 33(4), 314–329.
[2] Parnaby, M. G., & Carapetis, J. R. (2010). Rheumatic fever in indigenous Australian children. Journal of paediatrics and child health, 46(9), 527–533.
[3] Manuel, V., Mocumbi, A. O., & Zühlke, L. (2025). Rheumatic Heart Disease: Global Failure in Tackling a Common Killer. CJC Open.
[4] Gewitz MH, Baltimore RS, Tani LY, Sable CA, Shulman ST, Carapetis J et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation. 2015;131:1806–18.
[5] Manjunath, C., Srinivas, P., Ravindranath, K., & Dhanalakshmi, C. (2014). Incidence and patterns of valvular heart disease in a tertiary care high-volume cardiac center: A single center experience. Indian Heart Journal, 66(3), 320-326.
[6] Freant, L. J., & Hopkins, R. A. (1997). Aschoff Bodies in an Operatively Excised Mitral Valve. Cardiovascular Pathology, 6(4), 231-236.
[7] Gerber MA, Baltimore RS, Eaton CB, Gewitz M, Rowley AH, Shulman ST, et al. Prevention of rheumatic fever and diagnosis and treatment of acute streptococcal pharyngitis: a scientific statement from the American Heart Association.Circulation. 2009;119(11):1541–1551.doi:10.1161/CIRCULATIONAHA.109.191959.
[8] Al-Jazairi, A., Al-Jaser, R., Al-Halees, Z., Shahid, M., Al-Jufan, M., Al-Mayouf, S., Al-Rajhi, A., & Al-Hajjar, S. (2017). Guidelines for the secondary prevention of rheumatic heart disease: Endorsed by Saudi Pediatric Infectious Diseases Society (SPIDS). International journal of pediatrics & adolescent medicine, 4(1), 47–50.