
 or, more specifically...){kind=link}

Tibial Torsion Abnormal Tibial torsion is the rotation or twist along the longitudinal axis of the lower leg (shin bone) or, more specifically, the tibia. The condition primarily affects children. It gives the appearance of intoeing or ‘pigeon-toed feet’. It typically manifests during toddlerhood. Tibial torsion is a common cause of abnormal foot positioning in children as they begin walking. There are generally two types of tibial torsion.
External tibial torsion usually develops gradually with growth and is less common than internal torsion. It can cause out-toeing and may persist if severe. Internal tibial torsion is common at birth and typically resolves spontaneously by early childhood, usually by the age of 4–5 years. Persistent or severe torsion may indicate a neuromuscular problem and, in some cases, can contribute to bowleg deformities.[1]
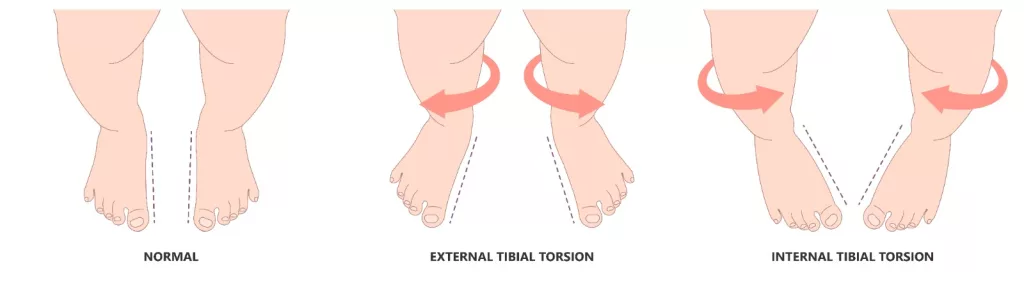
Visual difference between internal and external tibial torsion.
Etiology of Tibial Torsion: Tibial Torsion Abnormal
The etiology of tibial torsion is multifactorial. It can involve both developmental and genetic components, with contributing factors.
Developmental Causes
Internal tibial torsion is often attributed to intrauterine positioning, where the tibia rotates inward as the legs adapt to the confined space of the womb.[2] External tibial torsion can be present on its own or can be associated with other musculoskeletal disorders, including bowlegs, femoral torsion, or cerebral palsy.[3]
Genetic and Familial Factors
The evidence that tibial torsion runs in families suggests its hereditary predisposition to the condition. The children’s degree of tibial torsion and walking style resembles that of their parents.[4]
Idiopathic etiology
Several cases are idiopathic, meaning the exact cause is unknown. These cases likely result from complex interactions of genetic, environmental, and mechanical developmental factors affecting the tibial bone during growth.
How Tibial Torsion Develops?
The exact pathophysiology remains incompletely understood. Most torsional changes appear developmental and related to gait mechanics rather than purely congenital factors. Severe or persistent internal tibial torsion may increase medial compartment pressures in the knee during axial loading, potentially predisposing patients to osteoarthritis later in life.[5]
Symptoms of Tibial Torsion
Tibial torsion causes a patient to walk with their toes either facing inward (intoeing) or outward (out-toeing), rather than forward. This is observed when children make their first steps. It is usually painless, and children may appear clumsy, run awkwardly, and trip often.
External tibial torsion may be associated with symptomatic flat feet, tarsal coalitions, or knee problems if combined with femoral anteversion, including patellar instability or anterior knee pain.[6]
Diagnosis of Tibial Torsion
Diagnosis involves a combination of clinical examination and imaging techniques. Primary diagnosis is clinical.
Clinical Examination
Clinical diagnosis involves physical assessment of leg and foot rotation.
- The healthcare provider measures the angle between the thigh and foot (usually with a goniometer). It is the angle between the axis of the thigh and the foot. An angle greater than 10° of internal rotation indicates internal tibial torsion.
- The second physical evaluation includes the measurement of the foot progression angle. A negative angle indicates in-toeing.
Although clinical methods are more accessible, their reliability has some limitations compared to imaging; hence, images are necessary.
Imaging Tests
- The use of Computed tomography (CT) and Magnetic resonance imaging (MRI) is the gold standard of tibial torsion. They give precise data in three dimensions and also give a precise determination of the axes of the anatomy.[7]
- Ultrasound is a radiation-free alternative but requires specialized equipment. For tibial torsion, ultrasound is less commonly used due to its difficulty in reconstructing 3D torsional data.
- Radiographs (X-rays) may also assist, but are less precise for torsional measurements. They cannot quantify torsion as precisely as CT or MRI, but a tibial torsion X-ray can help identify indirect signs of abnormal tibial rotation, assess limb alignment, and rule out concurrent structural abnormalities such as genu varum/valgum or deformities related to ricketsor skeletal dysplasias
- In case of tibial torsion, imaging shows abnormal rotation of the tibia along its longitudinal axis. Rotation can be either internal or external.
Treatment of Tibial Torsion
In young children, internal tibial rotation usually improves on its own with the child’s growth. Most of the internal torsion improvements occur before school age and are not associated with any significant problems. External tibial torsion generally does not improve with growth and development. However, they do not cause symptoms in most of the children. The treatment of tibial torsion primarily depends on three factors. These are:
- Age of the patient
- Severity of the condition
- Functional impact of the condition
Treatment is based on these factors, including both non-surgical and surgical treatments.
Non-Surgical Treatment
Physical therapy and exercises that strengthen the muscles can be helpful in some situations in order to improve functioning. Physicians take into account dynamic splints like the Friedman counter splint applied in case of torsion. It inhibits inward rotational motion and permits other motions. Traditional braces and special shoes were once employed, but are not recommended, since there is no significant impact on the course of this condition.
Surgical Treatment for Tibial Rotation
Patients who have chronic internal tibial rotation and external tibial rotation, which present severe functional or painful situations, are subject to surgical therapy.[8]
Osteotomy involves cutting and rotating the tibia to align the toes forward. Internal fixation with screws, wires, or external fixators is used based on age and bone maturity. Surgical corrections enable people to become active again and alleviate joint pain. Realignment surgery in patients with significant symptoms might decrease their risk of future arthritis. Osteotomy surgery has become routine and acceptably safe with good results. Other limb deformities (as well as tibial torsion) can be treated with osteotomy, including the anteversion of the femur.

Internal Tibial Torsion. a: Before treatment, b: After treatment. Image courtesy: Efficacy of a Tibia Counter Rotator System for the Treatment of Internal Tibial Torsion in Children by Kim et al, 2022,doi.org/10.3390/children9070970, available via: https://www.mdpi.com/children/children-09-00970/article_deploy/html/images/children-09-00970-g002.png, CC BY 4.0.
Tibial Torsion vs. Femoral Anteversion
Tibial rotation and femur anteversion are two different anatomical cases. They both are deformities of rotation but in different sites, as well as clinical manifestation, and functional outcome. Tibial torsion involves twisting of the distal tibia, whereas femoral anteversion affects the proximal femur. The summary of these two conditions is provided in Table 1.
Table 1: Difference between Tibial Torsion and Femoral Anteversion
| Features | Tibial Torsion | Femoral Antevesion |
|---|---|---|
| Involved bone | Tibia (shinbone) | Femur (thigh) |
| Location of the twist | Twisting of the distal lower leg along the tibial axis. | Twisting of the proximal femoral neck. |
| Clinical signs | Intoeing/out-toeing due to foot alignment | In-toeing gait due to thigh internal rotation. |
| Diagnostic methods | Physical examCT axial exam | Physical exam o hip rotationCT femoral anteversion measurement |
These conditions might either occur alone or both. They may lead to gait abnormalities. The distinction is essential for proper clinical diagnosis, management, and planning of surgery.
How does Tibial Torsion Differ from Metatarsus Adductus?
Both conditions can cause in-toeing in children; however, their anatomical origins differ. Tibial torsion involves rotation of the tibia (shinbone) along its longitudinal axis, whereas metatarsus adductus affects the forefoot, causing the front part of the foot to curve inward. Clinically, tibial rotation presents as the entire foot pointing inward when standing or walking, whereas metatarsus adductus shows a distinct medial curvature of the forefoot while the hindfoot remains aligned. Tibial torsion typically resolves spontaneously by age 4–5, whereas mild metatarsus adductus often corrects by age 1–2; severe cases of either condition may require intervention. Differentiating between these two is essential for accurate diagnosis, monitoring, and management.
Final Remarks
Tibial torsion is a frequent phenomenon, which is associated with shinbone rotation. It is common among children, and is commonly in-toeing or out-toeing of the feet. The natural process entails automatic self-correction in early childhood, which is in line with natural musculoskeletal development. Nonetheless, physical therapy may be the most appropriate in the case of severe torsion or in cases that are associated with or occur after early childhood.
References
[1] Rerucha, C. M., Dickison, C., & Baird, D. C. (2017). Lower extremity abnormalities in children. American family physician, 96(4), 226-233.
[2] Carreiro, J. E. (2009).An osteopathic approach to children. Elsevier Health Sciences.
[3] Min, J. J., Kwon, S. S., Kim, K. T., Choi, Y., Sung, K. H., Lee, K. M., & Park, M. S. (2021). Evaluation of factors affecting external tibial torsion in patients with cerebral palsy.BMC musculoskeletal disorders,22(1), 684.
[4] BLUMEL, J., Eggers, G. W. N., & EVANS, E. B. (1957). Eight cases of hereditary bilateral medial tibial torsion in four generations.JBJS,39(5), 1198-1202.
[5] Huang, C., Chan, P. K., Chiu, K. Y., Yan, C. H., Yeung, S. S., Lai, C. W. K., … & Fu, S. N. (2023). The association between tibial torsion, knee flexion excursion and foot progression during gait in people with knee osteoarthritis: a cross-sectional study. BMC Sports Science, Medicine and Rehabilitation, 15(1), 110.
[6] Snow, M. (2021). Tibial torsion and patellofemoral pain and instability in the adult population: current concept review.Current reviews in musculoskeletal medicine,14(1), 67-75.
[7] Hawi, H., Kaireit, T. F., Krettek, C., & Liodakis, E. (2022). Clinical assessment of tibial torsion differences. Do we always need a computed tomography?.European Journal of Trauma and Emergency Surgery,48(4), 3229-3235.
[8] Davids, J. R., Davis, R. B., Jameson, L. C., Westberry, D. E., & Hardin, J. W. (2014). Surgical management of persistent intoeing gait due to increased internal tibial torsion in children.Journal of Pediatric Orthopaedics,34(4), 467-473.